










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 no.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.06.001
SPECIAL EDITION 2016
Chiropractic manipulative therapy of the thoracic spine in combination with stretch and strengthening exercises, in improving postural kyphosis in woman
Kim Castello Branco; M. Moodley*
Faculty of Health Sciences, University of Johannesburg, South Africa
ABSTRACT
PURPOSE: This study serves to determine the effectiveness of either chiropractic spinal manipulative therapy to the thoracic spine or stretch and strengthening exercises (stretching the pectoralis major muscle and strengthening the rhomboid, middle and inferior trapezius muscles) versus the combined treatment of chiropractic spinal manipulative therapy to the thoracic spine in conjunction with stretch and strengthening exercises.
METHOD: A randomised study design with thirty female participants between the ages of twenty and thirty nine was selected. Group 1 (n = 10) received chiropractic spinal manipulative therapy to the thoracic spine. Group 2 (n = 10) received chiropractic spinal manipulative therapy to the thoracic spine as well as stretch and strengthening exercises i.e. stretching the pectoralis major muscles and strengthening the rhomboid, middle and inferior trapezius muscles. Group 3 (n = 10) received stretch and strengthening exercises. The stretch and strengthening exercises were performed in the consultation rooms to ensure that the participants were complying with the treatment and doing the exercises properly. The study consisted of seven consultations for Group 1 (they received treatment once a week for six weeks) and for Groups 2 and 3 there were nineteen consultations (they received three treatments a week for six weeks). Objective data was recorded at the beginning of the first, fourth and seventh consultations for Group 1, and the first, tenth and nineteenth consultations for Groups 2 and 3. On the seventh consultation (for Group 1) and nineteenth consultation for Groups 2 and 3, only data collection was done. Objective data were obtained by using the Flexicurve® Ruler measurements for the angle of kyphosis. Visual analysis was done by taking lateral (sagittal) view photographs at the beginning of the initial and final consultations.
RESULTS: Statistical analysis revealed significant statistical changes for the intragroup results for all three groups. No significant statistical difference was found between the groups for the inter-group analysis.
CONCLUSION: The study showed that all three treatment protocols for Groups 1, 2, and 3 were effective. However, Group 1 had not shown a great improvement in their postural kyphosis, Group 3 had shown a relatively good improvement in their posture, while Group 2 had shown the best results with regards to improvement of the participants' posture. Therefore, in conclusion, Groups 2 and 3 treatment protocols can be used effectively to treat postural kyphosis but Group 2's treatment protocol, consisting of chiropractic spinal manipulative therapy to the thoracic spine in combination with stretch and strengthening exercises, will yield the best results.
Keywords: Chiropractic; Exercises; Flexicurve® Ruler; Kyphosis; Women
1. Introduction
Thoracic kyphosis is defined as an increase in the normal thoracic curvature of the spine (Teixeira & Carvalho, 2007). Postural kyphosis most commonly presents in young women owing to a number of factors, such as: sitting with a slouched posture; carrying heavy bags or backpacks to school or university; watching television; breast development leading to insecurity in some individuals (thereby causing shoulder protraction); and heavy manual work, as well as those owing to fashion trends, such as wearing high heeled shoes (Britnell et al., 2005).
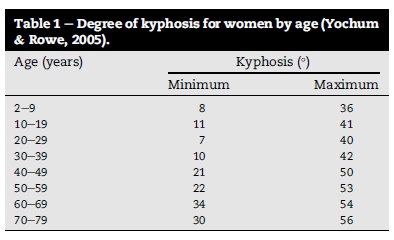
The normal range of kyphosis is between twenty and forty degrees, but it does vary with age and gender (Heary & Albert, 2007). The angle of kyphosis increases with age and this increase is greater in females than males (Yochum & Rowe, 2005). It has been shown that women are more susceptible to societal influences and psychological factors such as depression, insecurity and anxiety, leading to poor postural habits (Lewis & Valentine, 2010).
Studies have shown that teenage girls tend to develop kyphosis as a result of discomfort and insecurities that are experienced with breast development and altered body image. Women with large breasts have a tendency to have an increased kyphosis because of the increased weight of the breast tissue. In older women (twenty five to forty five years of age), the increased kyphosis has been attributed to certain sporting activities, financial stresses, physical abuse, pregnancy and wearing high heeled shoes (Britnell et al., 2005).
Hrysomallis and Goodman, stated that one of the causes of postural deviations such as kyphosis was weak and/or lengthened agonist muscle groups combined with a strong and tight antagonistic muscle group (Hrysomallis & Goodman, 2001). Stretch and strengthening exercises should be given in order to try and correct the postural deviation. The trapezius (middle and inferior parts) and rhomboid muscles need to be strengthened and the pectoralis major muscle needs to be stretched (Hrysomallis & Goodman, 2001). These exercises can help correct the postural kyphosis, as well as decrease the "rounded shoulder" effect that results from poor posture (Gatterman, 2004).
According to Gatterman, the mechanical effects of chiropractic spinal manipulative therapy are that it causes changes in joint alignment and corrects abnormal joint movement and spinal curves. There are various causes of altered joint function, such as: acute or repetitive injury, abnormal posture, poor coordination, age, defects that may be congenital or developmental and various diseases (Gatterman, 2005).
According to Pickar and Wheeler, spinal manipulative therapy increases joint mobility, thereby silencing gamma motor neurons. Gamma motor neuron activation is elevated in fixated spinal segments. When there is an increase in gamma motor neuron activation, joint mobility is impaired because the muscle stretch reflex is able to detect small changes in muscle length. Therefore, spinal manipulative therapy increases joint mobility, thus causing a barrage of impulses in muscle spindle afferents, decreasing gamma motor neuron activity. This will then cause a reduction in the gain of the gamma-loop through an undetermined neural pathway (Pickar & Wheeler, 2001).
Pickar (2002) stated that gamma motor neuron mechanoreceptors reset muscle spindles, which then restores muscle tonus. Increase in muscle strength has been noted (by using an electromyogram) after spinal manipulative therapy. Therefore, spinal manipulative therapy has shown to improve muscle function, either through facilitation or disinhibition of neural pathways (Pickar, 2002).
Spinal manipulative therapy will stretch the adjacent musculature of the vertebral level being adjusted. This "stretch" in the muscles activates the muscle spindles and Golgi tendon organ reflexes. The spinal manipulation will result in decreased hypertonicity in the muscles and therefore alter the tone of the muscle (Esposito & Philipson, 2005).
Instruments that are used to assess kyphosis must be viewed in terms of their accuracy, reliability, practicality and cost. The Flexicurve® Ruler was used to measure the angle of thoracic kyphosis in this quantitative study. It has been proven to be a valid and reliable means to measure thoracic kyphosis and is also inexpensive (Teixeira & Carvalho, 2007).
2. Materials and methods
2.1. Selection criteria
A selection of thirty female participants between the ages of twenty and thirty nine years was recruited for this study. This specific sample group was chosen because most cases of postural kyphosis occur in females (Hanfy, Awad, & Allah, 2012). The specific age group chosen was selected to limit structural changes that occur with increasing age (in the middle and elder years) (Britnell et al., 2005). All participants had no contra-indications to the application of chiropractic spinal manipulative therapy to the thoracic spine, no current musculoskeletal injury and no thoracic scoliosis or Pottenger's saucer that would affect the outcome of the study. The participants could not receive any other form of treatment that would interfere with the results of the study, including manual therapy such as massage, chiropractic treatment, physiotherapy as well as medication use such as muscle relaxants or anti-inflammatory drugs.
Participants that met the inclusion criteria were assigned into one of the three groups. Each group consisted of ten participants. Participants were assigned to their group by drawing a number from a box. The box contained 30 pieces of paper labelled 1, 2 or 3 (representing the group numbers). The number that the participant drew from the box was the group number that they were allocated to.
Group 1 received chiropractic spinal manipulative therapy to restricted thoracic spine segments. Group 2 received chiropractic spinal manipulative therapy to restricted thoracic spine segments as well as stretch and strengthening exercises (stretching the pectoralis major muscle and strengthening the rhomboid, middle and inferior trapezius muscles). Group 3 received stretch and strengthening exercises only.
2.2. Methodology
Participants were recruited by word of mouth as well as by making use of advertisements which were placed around the University of Johannesburg Doornfontein Campus and the Chiropractic Day Clinic. This research study took place at the Chiropractic Day Clinic. Willing female participants' had their angle of kyphosis measured, which had to fall within the angle of kyphosis for their required age group (Table 1).
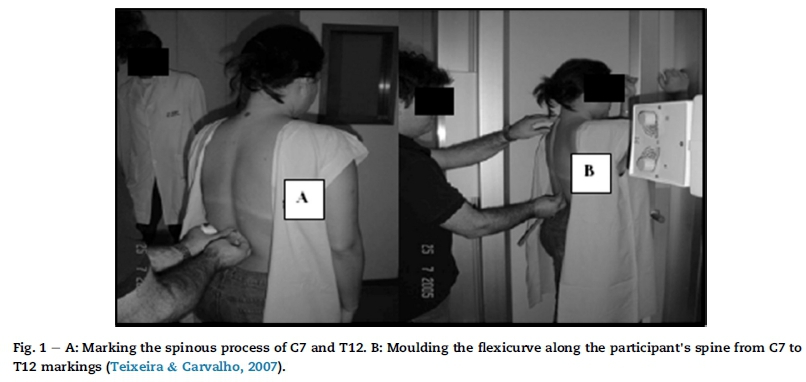
Each participant's angle of kyphosis was measured using the Flexicurve® Ruler. The C7 and T12 spinous processes were marked. The Flexicurve® Ruler was moulded to the participant's spine from the markings C7 to T12. The curve formed from the ruler was traced to paper. A straight line was drawn connecting the C7 and T12 points, and the lengths of E, L1 and L2 were measured. The angle of kyphosis was calculated using: Theta = arc tan (E/L1) + arc tan (E/L2). See Fig. 1 and Fig. 2.
A photograph of each participant's postural kyphosis was taken in a lateral (sagittal) plane. The plumb line was also used to measure the participants' kyphosis on the initial and final consultations.
Group 1 received treatment once a week for six weeks. Each treatment consisted of chiropractic spinal manipulative therapy to restricted thoracic spine segments. Each participant's angle of kyphosis was taken on the first, fourth and seventh consultations prior to receiving treatment. On the seventh consultation, only data collection was done, there was no treatment given.
Groups 2 and 3 received three treatments a week for six weeks. Group 2 participants received chiropractic spinal manipulative therapy to restricted thoracic spine segments once a week for six weeks and stretch and strengthening exercises three times a week for six weeks. Group 3 participants received stretch and strengthening exercises three times a week. Each participant's angle of kyphosis (for Groups 2 and 3) was taken on the first, tenth and nineteenth consultations prior to receiving treatment. On the nineteenth consultation, only data collection was done, there was no treatment given.
The combination, phalangeo-metacarpal and anterior thoracic diversified manipulative techniques was used in this study. All techniques chosen produced a consistent result with the application of a controlled force, leverage, direction and velocity to the specific restricted thoracic facet joints (Bergmann & Peterson, 2011).
Postural advice (on how to sit and stand correctly) was given to all three groups.
3. Results
The Shapiro-Wilk test for normality was performed to determine if the data was normally distributed, with a statistical significant level set at p ≤ 0.05.
3.1. Inter-group analysis
3.1.1. Clinical interpretation
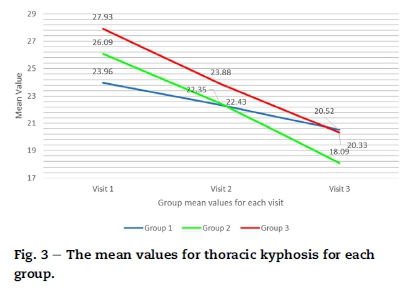
As seen in Fig. 3, Group 1 had a mean decrease in thoracic kyphosis of 14.33%. Group 2 had a mean decrease in thoracic kyphosis of 30.66% and Group 3 had a mean decrease in thoracic kyphosis of 27.22%.
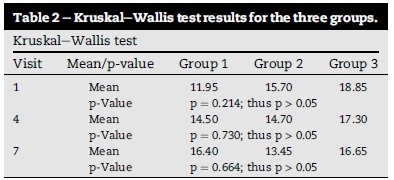
For the inter-group analysis, the non-parametric Kruskal-Wallis test was used to examine differences between the three groups at each time period.
The Kruskal-Wallis test results presented in Table 2 show that the p-value at visit one was not statistically significant (p = 0.21). The baseline reading of p = 0.21 showed that the groups started off comparable. However, the p-value remained greater than 0.05 at visit four (p = 0.73) and visit seven (p = 0.66). Therefore, there was no statistical difference (p > 0.05) noted between the three groups at each of the three visits. As there were no significant statistical differences present within the Kruskal-Wallis test inter-group results, the Mann-Whitney U test was not performed.
3.2. Intra-group analysis
3.2.1. Clinical interpretation
3.2.1.1. Group 1
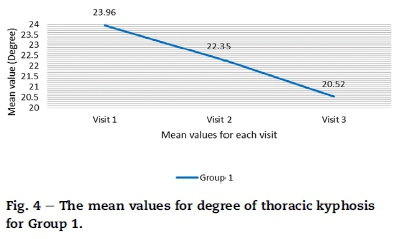
In Fig. 4 at visit one, Group 1 had a mean thoracic kyphosis of 23.96°. At visit four, the mean thoracic kyphosis was 22.35°. At visit seven, the mean thoracic kyphosis was 20.52°. The mean decrease in thoracic kyphosis was 14.33%. As seen from the line graph, there is a linear decrease, indicating that the degree of kyphosis had decreased within this group from visits one to seven.
3.2.1.2. Group 2
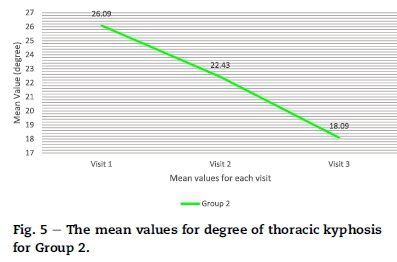
In Fig. 5 at visit one, Group 2 had a mean thoracic kyphosis of 26.09°. At visit four, the mean thoracic kyphosis was 22.43°. At visit seven, the mean was 18.09°. The mean decrease in thoracic kyphosis was 30.66%. As seen from the line graph, there is a linear decrease, indicating that the degree of kyphosis had decreased within this group from visits one to seven.
3.2.1.3. Group 3
In Fig. 6 at visit one, Group 3 had a mean thoracic kyphosis of 27.93°. At visit four, the mean thoracic kyphosis was 23.88°. At visit seven, the mean thoracic kyphosis was 20.33°. The mean decrease in thoracic kyphosis was 27.22%. As seen from the line graph, there is a linear decrease, indicating that the degree of kyphosis had decreased within this group from visits one to seven.
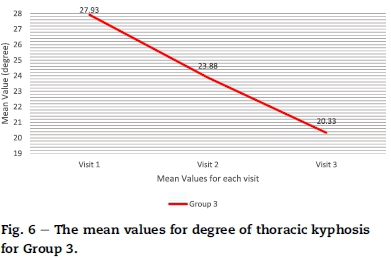
Fig. 4 shows that the mean decrease in thoracic kyphosis for Group 1 was 14.33% and had a decrease in the degree of kyphosis by 3.44°. The mean decrease in thoracic kyphosis for Group 2 (as seen in Fig. 5) was 30.66% and had a decrease in the degree of kyphosis by 8.00°. Fig. 6 showed that the mean decrease in thoracic kyphosis for Group 3 was 27.22% and had a decrease in the degree of kyphosis by 7.60°. Thus Group 2 had the best improvement clinically as the change in their degree of thoracic kyphosis was the greatest.
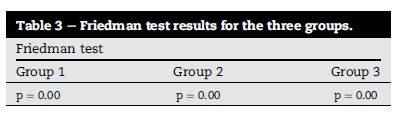
For the intra-group analysis, the Friedman test was used and, if positive, the Wilcoxon Signed Ranks test was used.
The results presented in Table 3 were statistically significant (p ≤ 0.05) in all three groups. Group 1 had a p-value of 0.00, Group 2 had a p-value of 0.00 and Group 3 had a p-value of 0.00. The Wilcoxon Signed Ranks test was used for within group analysis to demonstrate where these changes occurred.
From the results presented in Table 4, the test revealed that there was a significant statistical improvement in all three groups (p ≤ 0.05) from visits one to four, as well as from visits one to seven.
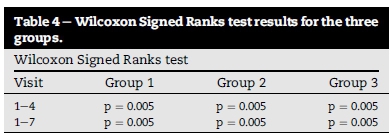
As there was a statistical significant difference between visits one to four and visits one to seven in all three groups, this indicates that the treatment was effective in reducing kyphosis from the onset of the treatment to the end. Therefore, there was a consistent change from the first to final visits in all three groups.
3.3. Visual analysis
From the photographs taken, visually there was a minor improvement in each participant's posture assessed, using the plumb line over the course of the study. After analysing each participant's initial and final photograph it could be seen that Groups 2 and 3 had shown the greatest improvement visually, whereas Group 1 visually had not shown much improvement in their posture.
4. Discussion
Levangie and Norkin (2005) stated that faulty posture, if continued on a daily basis, over time results in structural changes such as ligamentous or muscle shortening or lengthening. Hrysomallis and Goodman (2001) stated that one of the causes of postural deviations such as kyphosis was owing to having a weak and lengthened agonist muscle group combined with a strong and tight antagonistic muscle group.
It was evident from the results that all three groups had a significant improvement in their posture. The results of the study suggested that the combination group (of spinal manipulative therapy to the thoracic spine and stretch and strengthening exercises) produced the best results in decreasing the degree of postural kyphosis.
With regards to the intra-group analysis, clinically, all three groups had shown a decrease in the mean values for the degree of thoracic kyphosis. However, Group 2 had the greatest decrease in the mean value. This result indicated that the Group 2 treatment protocol was the most effective in improving postural kyphosis, which could be due to the mechanical effects of spinal manipulative therapy combined with the effect of performing stretch and strengthening exercises. Statistically, all three groups had shown that there was a change in their degree of kyphosis over time.
Gatterman (2005) stated that some of the mechanical effects of chiropractic spinal manipulative therapy were that it causes changes in joint alignment, abnormal joint movement and spinal curves. Pickar (2002) stated that increased joint mobility, increased muscle strength and decreased muscle spasm were some of the effects of spinal manipulative therapy. Chiropractic spinal manipulative therapy stretches the adjacent musculature of the vertebral level being adjusted. This "stretch" in the muscles will then activate the muscle spindles and golgi tendon organ reflexes, which will decrease the state of hypertonicity in the muscles and therefore alter the tone of the muscle (Esposito and Philipson, 2005 and Pickar, 2002).
Hrysomallis and Goodman (2001) stated that stretch and strengthening exercises should be given in order to try and correct the postural deviation. The trapezius (middle and inferior parts) and rhomboid muscles need to be strengthened and the pectoralis major muscles need to be stretched. These exercises can help correct the postural kyphosis as well as decrease the "rounded shoulder" effect that occurs due to these postural effects (Gatterman, 2004).
The study showed that the treatment protocols for Groups 1, 2 and 3 were effective in treating postural kyphosis. Nevertheless, taking the above information into account, it suggests that Group 2 treatment protocol was the most effective. Evidence also suggests that Group 2 and 3 treatment protocols were more effective than Group 1's treatment protocol. Therefore, Group 2 had shown the best results, owing to the mechanical and neurological effects of spinal manipulative therapy in combination with the effect that the exercises performed has on posture.
5. Conclusion
It was evident from the results that the participants in the three groups had responded well to their treatment protocols. Regarding objective measurements, Groups 1, 2 and 3 demonstrated clinical and statistical improvements in their degree of thoracic kyphosis i.e. there was a decrease in the degree of kyphosis. It was found that Group 2 responded best, with its combined treatment protocol. However, in the inter-group analysis there were no statistically significant differences found in the thoracic kyphosis values between the three groups.
Therefore, in conclusion, Groups 2 and 3 treatment protocols can be used effectively to treat postural kyphosis, but Group 2's treatment protocol will yield the best results.
Acknowledgements
This study was funded by the University of Johannesburg.
References
Bergmann, T. F., & Peterson, D. H. (2011). Chiropractic technique principles and procedures (3rd ed.). USA: Elsevier Mosby. pp. 85, 209, 213, 221. [ Links ]
Britnell, S. J., Cole, J. V., Isherwood, L., Sran, M. M., Britnell, N., Burgi, S., et al. (2005). Postural health in women: the role of physiotherapy. Journal of Obstetricians and Gynaecologists of Canada, 27(5), 493e500. [ Links ]
Esposito, S., & Philipson, S. (2005). Spinal adjustment technique: The chiropractic art. Australia: Craft Printing. pp. xi, 2, 3, 4, 7, 8. [ Links ]
Gatterman, M. A. (2004). Chiropractic management of spine related disorders (2nd ed.). Lippincott Williams and Wilkins. pp. 41, 82e83, 302. [ Links ]
Gatterman, M. A. (2005). Foundations of chiropractic subluxation (2nd ed.). Missouri: Elsevier Mosby. pp. 11, 34, 35, 36, 136e138, 140e141. [ Links ]
Greendale, G. A., Nili, N. S., Huang, M. H., Seeger, L., & Karlamangla, A. S. (2011). The reliability and validity of three non-radiological measures of thoracic kyphosis and their relations to the standing radiological Cobb angle. Osteoporosis International, 22, 1897e1905. [ Links ]
Hanfy, H. M., Awad, M. A., & Allah, A. H. A. A. (2012). The effect of exercise on postural kyphosis in females after puberty. Indian Journal of Physiotherapy & Occupational Therapy Letter, 6(3), 190e194. [ Links ]
Heary, R. F., & Albert, T. J. (2007). Spinal deformities, the essentials (p. 193). New York: Thieme Medical Publishers. [ Links ]
Hrysomallis, C., & Goodman, C. (2001). A review of resistance exercise and posture realignment. Journal of Strength and Conditioning Research, 15(3), 385e390. [ Links ]
Levangie, P. K., & Norkin, C. C. (2005). Joint structure and function: A comprehensive analysis (4th ed.). Philadelphia: F.A. Davis Company. pp. 481, 482, 484, 486, 487, 493. [ Links ]
Lewis, J. S., & Valentine, R. E. (2010). Clinical measurement of the thoracic kyphosis. A study of the intra-rater reliability in subjects with and without shoulder pain. BMC Musculoskeletal Disorders, 11(39), 1471e2474. [ Links ]
Pickar, J. G. (2002). Neurophysiological effects of spinal manipulation. The Spine Journal, 2(5), 357e371. [ Links ]
Pickar, J. G., & Wheeler, J. D. (2001). Response of muscle proprioceptors to spinal manipulative-like loads in the anaesthetized cat. Journal of Manipulative and Physiological Therapeutics, 24(1), 2e11. [ Links ]
Teixeira, F. A., & Carvalho, G. A. (2007). Reliability and validity of thoracic kyphosis measurements using the flexicurve method. Revista Brasileira de Fisioterapia, 11(3), 1. [ Links ]
Yochum, T. R., & Rowe, L. J. (2005). Essentials of skeletal radiology (3rd ed., Vol. 1, p. 215). Philadelphia: Lippincott Williams and Wilkins. [ Links ]
Received 5 October 2015
Accepted 2 June 2016
Available online 21 August 2016
E-mail addresses: mmoodley@uj.ac.za, mikhamoo123@gmail.com (M. Moodley).
Peer review under responsibility of Johannesburg University.
* Corresponding author.


{kind=link}
{kind=link}