










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 n.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.07.005
FULL LENGTH ARTICLE
The FitTrack Index as fitness indicator: A pilot study
Dina Christina Janse van RensburgI, II, *; Catharina Cornelia GrantI, II; Audrey Jansen van RensburgI, II; Roelf Petrus Gerhardus BothaI; Paola Silvia WoodII, III, IV; Kim NolteIII, IV; Lizelle FletcherV; Peet Jacobus du ToitII, V, VII, VIII; Michael Sean PepperVIII, IX; Pieter Ernst KrugerII, III, IV
ISection Sports Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IIExercise SMART Team, University of Pretoria, South Africa
IIIDepartment of Biokinetics, Faculty of Health Sciences, University of Pretoria, South Africa
IVInstitute for Sports Research, Faculty of Humanities, University of Pretoria, South Africa
VInstitute for Food, Nutrition and Well-being, University of Pretoria, South Africa
VIDepartment of Statistics, Faculty of Natural and Agricultural Sciences, University of Pretoria, South Africa
VIIDepartment of Human Physiology, Faculty of Health Sciences, University of Pretoria, South Africa
VIIIInstitute for Cellular and Molecular Medicine, University of Pretoria, South Africa
IXDepartment of Immunology, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: The FitTrack Index is a web-based programme developed in South Africa and widely used by athletes to indicate their fitness. A need exists for a self-managed, non-invasive tool to evaluate and categorise health-related fitness in different population groups. The aim of this study was to compare the FitTrack Index with a reliable measure of cardio-respiratory fitness as indicated by maximal oxygen uptake (direct VO2max
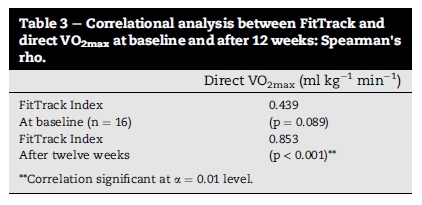
Methods & results: During a 12-week cross-sectional, descriptive pilot study the direct laboratory tested VO2max indicated a moderate to strong correlation with the FitTrack Index (Spearman's rho = 0.439, p = 0.089 at baseline; Spearman's rho = 0.853, p < 0.001 after 12 weeks).
CONCLUSIONS: These results suggest that the web-based FitTrack Index may be considered an appropriate tool to evaluate exercise capacity and cardiovascular fitness in healthy individuals following an aerobic training programme
Keywords: Aerobic fitness; Exercise ability; Recreational fitness; Cardiovascular fitness; Fitness indication; VO2max
1. Introduction
Cardiorespiratory fitness testing is a measure known to be a strong and independent predictor of cardio-vascular disease (CVD) and mortality (Bouchard, Shephard, & Stephens, 1993). Not only is it a quantitative clinical diagnostic and prognostic health indicator, but also a dynamic tool to evaluate exercise ability and aerobic fitness (Thompson et al., 2003). A recent publication by Duncan, Kutlubaev, Dennis, Greig, and Mead (2012) define physical fitness as 'the collective term for a set of physiological attributes, which people have or achieve that determine the ability to perform physical activity'. Being a health-related component of physical fitness, cardiorespiratory fitness is defined as the ability of the circulatory, respiratory, and muscular systems to supply oxygen during sustained physical activity ( Jackson et al., 2009 and Lee et al., 2010). Health problems, and especially non-communicable diseases, can fundamentally be attributed to the physical activity patterns of humans that have changed over decades (Archer & Blair, 2011). Based on meaningful research and epidemiological studies over the past years, it is widely accepted that higher levels of cardiorespiratory fitness and physical activity patterns are associated with better health outcomes (Myers et al., 2015).
The gold standard for measuring cardiorespiratory fitness is the determination of maximal oxygen uptake (VO2max), measured by the volume of oxygen an individual consumes while exercising at maximum capacity. It has been used as a predictor of survival and performance in several clinical and athletic populations (Paterson et al., 2004 and Stringer, 2010). VO2max analysis determines an athlete's capacity to perform sustained exercise and is linked to aerobic endurance (Reiman & Manske, 2009). However, VO2max analysis is expensive, and laboratory linked.
The American College of Sports Medicine's guidelines for health/fitness lists the components of physical activity as the FITT-VP principles of exercise prescription, and includes: Frequency (how often?), Intensity (how hard?), Time (duration or how long?), Type (mode or what kind?), with the addition of total Volume (the product of Frequency, Intensity, and Time or amount) and Progression (advancement). For cardiorespiratory fitness and body composition they recommend: a frequency of 3-5 days/week; at an intensity of 55/65%-90% of maximum heart rate (HRmax); and duration of 20-60 min of continuous or intermittent training for exercises rhythmical and aerobic in nature, e.g. walking-hiking, running-jogging, cycling-bicycling, cross-country skiing, aerobic dance/group exercise, rope skipping, rowing, stair climbing, swimming, skating, and various endurance game activities or some combination thereof (ACSM's Guidelines for Exercise Testing and Prescription, 2013).
Health related physical fitness relates directly to a person's health status and being physically active plays an essential role in ensuring health and well-being. Physical activity benefits many parts of the body and can reduce many of the risk factors for non-communicable diseases (Guiney and Machado, 2013 and Mezzani et al., 2013). The need exists for a fast, non-invasive and accessible tool that recreational athletes could use to evaluate and categorise health-related fitness, and track their progress. The FitTrack Index (Training Plans for Cycling and Running) is a web-based fitness tracking programme developed for athletes from different sport settings. The programme is designed to combine an athlete's exercise intensity, exercise duration and their specific sport practiced to give an indication of their overall fitness.
The FitTrack programme has not been validated against a reliable measure of cardiorespiratory fitness, such as direct VO2max. This paper investigates the appropriateness of the web-based FitTrack Index as a self-managed tool to evaluate exercise ability and cardiovascular fitness, and indicate progress in physical fitness in recreational individuals following an aerobic training programme. The aim was to compare the FitTrack Index with direct VO2max measurements, assessed at baseline and after 12 weeks of self-determined activities (walking, running or a combination thereof).
2. Methods
The association between a fitness programme (FitTrack Index) and validated direct VO2max measures of aerobic fitness was evaluated. Data were sampled on two occasions with 12 weeks between measurements. No standardised intervention was followed during the 12-week period. However, participants were encouraged to follow an aerobic programme of their choice from the FitTrack website. The participant's FitTrack Index was determined on-line on the website, based on data logged 3 to 4 times a week for 12 consecutive weeks. The direct VO2max measurements were taken twice - once during week 1 (at baseline) and again during week 12 of the study. The focus of the project was to determine the associations between the different instruments used to measure activity/fitness and not the effect of exercise per se.
2.1. Participants
Volunteer participants were enrolled by means of advertisements and word of mouth. Participant inclusion criteria stated healthy male and female volunteers. Participant exclusion criteria included persons who reported a history of cardiovascular disease; had suffered lung or respiratory tract infections 2 weeks prior to the study; were using any medication that could influence cardiovascular control; and those who reported endocrine- or metabolic disorders. Only participants with complete data sets and who persisted from baseline to week 12 (n = 16) of the study were included in the data analyses.
2.2. Ethical clearance
The research protocol was approved by the Ethics Committee of the Faculty of Health Sciences, University of Pretoria (Number 135/2011). In a pre-study orientation and screening session, all participants were informed relating to the aims of the study and gave written consent. The study complied with the guidelines for good clinical practice (GCP).
2.3. FitTrack Index
On the web programme, two formulas are used to calculate the FitTrack Index total. The first calculates points for a specific workout (exercise event) and the second calculates a fitness score based on past workouts. FitTrack workout points are calculated based on exercise intensity, exercise duration and the specific sport practiced. Exercise intensity is calculated as a function of average heart rate, maximum heart rate and/or rate of perceived exertion (RPE). The FitTrack fitness score is calculated on a 42-day (6-week) moving average of the workout points. Fig. 1 is an example of how the score is displayed to athletes.
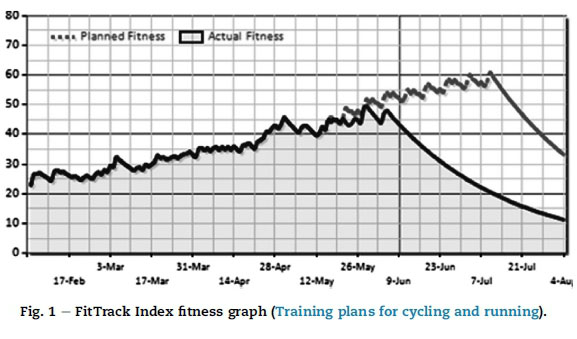
Participants registered on the FitTrack website, and with their own expected fitness goal in mind and a clear estimation of their current fitness status, chose an exercise programme ranging from 'beginner' to 'advanced'. Each programme described the goal based outcomes of the exercise programme and the recommended fitness level the participant should be at. The participants' selected exercise programme was loaded onto their profile and they received a 7-day schedule of their daily training sessions. As the participants completed their daily exercise sessions and logged their activity on the website, their 'predicted' fitness score was plotted on a graph. Their actual FitTrack Index (the black line) either increased or decreased and could be compared with their predicted fitness line (the grey line). The more conscientious participants follow their exercise programme and the more frequently they log their exercises, the closer the FitTrack Index approximates a true value.
2.4. Direct VO2max measurement
Cardiopulmonary fitness assessment using direct VO2max measurements were determined by means of respiratory gas analysis equipment in a laboratory. An incremental exercise testing protocol was used to determine direct VO2max (Bentley, Newell, & Bishop, 2007). Individuals were exposed to ergometric testing with progressive intensity increase each minute, until maximum exertion was reached. Oxygen and carbon dioxide fractions were analysed, and peak oxygen usage at maximum exercise expressed in millilitres of oxygen, per minute, per kilogram of body weight (ml kg−1 min−1).
Prior to assessment participants were permitted 5 min of light stretching and a 5 min run at approximately 10 km/h to warm up. Thereafter, the treadmill speed was increased by 1 km/h every minute and a 0.5% inclination grade every 2 min. A plateau in O2 uptake, a rate of perceived exertion (RPE) equal to or greater than 18, a respiratory exchange ratio (RER) >1.15, a heart rate (HR) of 85% of age-predicted maximum and volitional exhaustion were used to verify that VO2max was reached (Rowland, 1996). Pulmonary gas exchange and HR were analysed continuously during the test with the use of an automated ergo-spirometer and electrocardiograph (COSMED K4b2). VO2max was recorded as the highest oxygen uptake (VO2) averaged over 30 s of the test, and reported in relative terms (ml kg−1 min−1).
2.5. Statistical analysis
The information obtained from the participants was captured and analysed by means of the IBM SPSS Statistics Version 19 package. Descriptive statistics were calculated to summarise the information. Correlational analysis was employed to evaluate the strength of comparison between the FitTrack Index and direct VO2max. The Spearman rank correlation coefficient (Spearman's rho) was calculated since the association between VO2max and the FitTrack Index is not linear. A 5% level of significance (α = 0.05) was used to determine if there was a statistically significant monotonic relationship between the variables.
3. Results
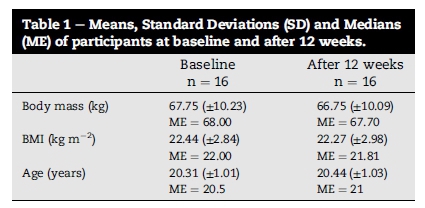
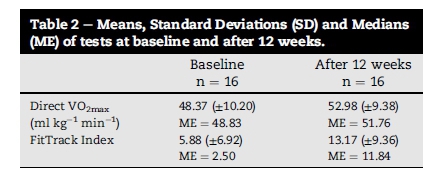
Descriptive statistics of the participants and of the tests completed at baseline and after 12 weeks of exercise intervention are presented in Table 1 and Table 2 respectively. Little difference was found in body mass and Body Mass Index (BMI) over the 12-week period.
The correlations were both positive and significant. A moderate correlation was found between baseline FitTrack Index and direct measurement of VO2max. The 12-week correlation coefficient indicates a strong relationship between the FitTrack Index and the direct VO2max.
The lower correlation coefficient at baseline can be explained by the fact that the initial starting point/value when joining the FitTrack Index was a personal estimated value, as explicated in the methods section. The more conscientious the participants followed their exercise programme and the more frequently they logged their exercises, the closer to a true value their fitness curve was reflected.
4. Discussion
A highly significant correlation between the FitTrack Index and the directly determined VO2max measurements after 12 weeks was observed. In accordance with the Landis and Koch (1977) classification scale, the strength of correlation observed in this study was 'almost perfect' for cardiovascular fitness. This suggests that the web-based FitTrack Index programme may be used as a self-managed, non-invasive indicator of cardiovascular fitness.
Maximal capacity for oxygen consumption is typically expressed as the VO2max, which indicates full cardio-pulmonary potential (Arts and Kuipers, 1994 and Vanhees et al., 2005), and is widely used for athletes and the general public as a measure of aerobic fitness (Stringer, 2010). Laboratory-determined VO2max is the preferred method for assessing physical fitness (Vanhees et al., 2005) and to accurately predict maximal oxygen uptake as an indicator of dynamic exercise capacity (Carey, 1997 and Larsen et al., 2002). Regardless of the method used to determine VO2max, exercise training is acknowledged to improve peak oxygen uptake. Research suggests that moderate regular exercise should be considered as a worthwhile means of treating poor mental and physical self-perceptions (Fox, 1999 and Penedo and Dahn, 2005). Increased aerobic capacity also promotes a cascade of cardio-protective outcomes, such as various anti-arrhythmic and anti-ischemic effects (Vanhees et al., 2005).
Results from this study suggest that the FitTrack Index programme may be used as a tool in healthy population studies and athlete groups as an indicator of exercise ability and aerobic fitness. Correlation between the FitTrack Index and direct VO2max were highly significant as indicated in Table 3.
The augmented association strength between the FitTrack Index and direct VO2max determination from baseline to 12 weeks is attributed to the methodology employed behind the calculation of the FitTrack score. VO2max results at baseline are correlated with a predicted beginning FitTrack fitness score, based on the athletes estimated fitness measure at onset, whilst results after 12 weeks are correlated with a concurrent calculated FitTrack fitness index based on exercise sessions logged by the participant throughout the training programme. For this reason, the calculation represents a more accurate fitness score. The FitTrack fitness score is calculated using a 6 week moving average of all points received for workouts logged. It indicates a trend-following pointer and highlights the athlete's fitness progress. This further accentuates the compelling accord between the FitTrack Index and VO2max as an indicator of aerobic fitness. VO2max is influenced by factors such as exercise history (training), genetics, sex, age, body temperature, respiration and body fat (Larsen et al., 2002). Both active and sedentary individuals' VO2max values increase when serious aerobic training is undertaken (Klissouras, 1972).
The FitTrack Index as a web-based fitness progress programme was developed to assist expert and recreational athletes in obtaining access to training programmes designed by professional experienced coaches for different sport settings and competition events. Training programmes adjusted to the level of fitness of the athlete, provide an easy simple and motivated way of training and tracking fitness progress. Intensity, duration and frequency of workouts are used to calculate a fitness score for every training session logged, and fitness improvement is tracked accordingly. By following a validated fitness-measuring programme the athlete will stay enthusiastic and inspired in achieving their goal, while improving their physical fitness and visually observing the advance in their cardiorespiratory fitness level.
It is important to stress that the focus of this study was not to determine the effect of exercise, but rather the correlation of different fitness measuring instruments. In this case, a comparison between the FitTrack Index and direct measurements of VO2max, an accredited indicator of improved aerobic fitness, was specifically assessed (Martin & Coe, 1997). Since the outcomes of the study confirm highly significant correlations between the FitTrack Index and direct VO2max results, it is apparent that the FitTrack score may be considered an appropriate evaluation of exercise capacity and cardiovascular fitness. This further substantiates FitTrack as a fitness-measuring instrument that is able to accurately, and in concordance with conventional cardiopulmonary methodologies, indicate changes in physical fitness in individuals following an aerobic training programme.
5. Conclusion
Comparison between the FitTrack Index and exercise capacity, as indicated by direct measurements of VO2max, was specifically assessed. This study confirmed that there is a highly significant association or an 'almost perfect' strength of correlation, between the FitTrack Index and VO2max fitness assessment measured after a 12-week period when comparing cardiovascular fitness. The FitTrack Index and scoring method may therefore be considered an appropriate self-managed tool to evaluate exercise ability and cardiovascular fitness and indicate changes in physical fitness in individuals following an aerobic training programme.
Future research will include longitudinal studies aimed at assessment of the FitTrack Index score and its correlation to cardio respiratory measures, and comparison with other fitness components such as indirect VO2max techniques and muscular endurance and strength.
Author disclosure
This manuscript reports on original research, and has not previously been published neither is it submitted elsewhere for publication. No conflict of interest exists in any part of the manuscript. Informed consent was signed by all participants.
Acknowledgements
Research was partly funded by Momentum, South Africa (Reference No.: TP1208066080).
References
American College of Sports Medicine. (2013). ACSM's guidelines for exercise testing and prescription. Lippincott Williams & Wilkins. [ Links ]
Archer, E., & Blair, S. N. (2011). Physical activity and the prevention of cardiovascular disease: From evolution to epidemiology. Progress in Cardiovascular Diseases, 53(6), 387e396. [ Links ]
Arts, F. J. P., & Kuipers, H. (1994). The relation between power output, oxygen uptake and heart rate in male athletes. International Journal of Sports Medicine, 15(5), 228e231. [ Links ]
Bentley, D. J., Newell, J., & Bishop, D. (2007). Incremental exercise test design and analysis: Implications for performance diagnostics in endurance athletes. Sports Medicine, 37(7),575e587. [ Links ]
Bouchard, C., Shephard, R. J., & Stephens, T. (1993). Physical activity, fitness, and health consensus statement. Champaign, IL: Human Kinetics Publishers. [ Links ]
Carey, D. G. (1997). Comparative ability of four submaximal exercise tests to predict changes in maximal oxygen uptake consequent to an aerobic training programme. Biology of Sport, 14(2), 135e144. [ Links ]
Duncan, F., Kutlubaev, M. A., Dennis, M. S., Greig, C., & Mead, G. E. (2012). Fatigue after stroke: A systematic review of associations with impaired physical fitness. International Journal of Stroke: Official Journal of the International Stroke Society, 7(2), 157e162. http://dx.doi.org/10.1111/j.1747-4949.2011.00741.x. [ Links ]
Fox, K. R. (1999). The influence of physical activity on mental wellbeing. Public Health Nutrition, 2(3), 411e418. [ Links ]
Guiney, H., & Machado, L. (2013). Benefits of regular aerobic exercise for executive functioning in healthy populations. Psychonomic Bulletin & Review, 20(1), 73e86. [ Links ]
Jackson, A. S., Sui, X., Hebert, J. R., Church, T. S., & Blair, S. N. (2009). Role of lifestyle and aging on the longitudinal change in cardiorespiratory fitness. Archives of Internal Medicine, 169(19), 1781e1787. http://dx.doi.org/10.1001/archinternmed.2009.312. [ Links ]
Klissouras, V. (1972). Genetic limit of functional adaptability. Internationale Zeitschrift Fu¨ r Angewandte Physiologie, Einschliesslich Arbeitsphysiologie, 30(2), 85e94. [ Links ]
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), 159e174. [ Links ]
Larsen, G. E., George, J. D., Alexander, J. L., Fellingham, G. W., Aldana, S. G., & Parcell, A. C. (2002). Prediction of maximum oxygen consumption from walking, jogging, or running. Research Quarterly for Exercise & Sport, 73(1), 66e72. [ Links ]
Lee, D., Artero, E. G., Sui, X., & Blair, S. N. (2010). Mortality trends in the general population: The importance of cardiorespiratory fitness. Journal of Psychopharmacology (Oxford, England), 24(4), 27e35. http://dx.doi.org/10.1177/1359786810382057. [ Links ]
Martin, D. E., & Coe, P. N. (1997). Better training for distance runners (2nd ed.). Champaign, IL: Human Kinetics Publishers. [ Links ]
Mezzani, A., Hamm, L. F., Jones, A. M., McBride, P. E., Moholdt, T., Stone, J. A., et al. (2013). Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: A joint position statement of the European association for cardiovascular prevention and rehabilitation, the American association of cardiovascular and pulmonary rehabilitation and the Canadian association of cardiac rehabilitation. European Journal of Preventive Cardiology, 20(3), 442e467. [ Links ]
Myers, J., McAuley, P., Lavie, C. J., Despres, J.-P., Arena, R., & Kokkinos, P. (2015). Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Progress in Cardiovascular Diseases, 57(4), 306e314. [ Links ]
Paterson, D. H., Govindasamy, D., Vidmar, M., Cunningham, D. A., & Koval, J. J. (2004). Longitudinal study of determinants of dependence in an elderly population. Journal of the American Geriatrics Society, 52(10), 1632e1638. [ Links ]
Penedo, F. J., & Dahn, J. R. (2005). Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry, 18(2), 189e193. [ Links ]
Reiman, M. P., & Manske, R. C. (2009). Functional testing in human performance. Human Kinetics. [ Links ]
Rowland, T. W. (1996). Developmental exercise physiology. Champaign, IL: Human Kinetics. [ Links ]
Stringer, W. W. (2010). Cardiopulmonary exercise testing: Current applications. Expert Review of Respiratory Medicine, 4(2), 179e188. http://dx.doi.org/10.1586/ers.10.8. [ Links ]
Thompson, P. D., Buchner, D., Pina, I. L., Balady, G. J., Williams, M. A., Marcus, B. H., et al. (2003). Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the council on clinical cardiology (subcommittee on exercise, rehabilitation, and prevention) and the council on nutrition, physical activity, and metabolism (subcommittee on physical activity). Circulation, 107(24), 3109e3116. [ Links ]
Training plans for cycling and running. FitTrack in partnership with momentum multiply wellness & rewards. Retrieved from: http://www.fittrack.co.za. [ Links ]
Vanhees, L., Lefevre, J., Philippaerts, R., Martens, M., Huygens, W., Troosters, T., et al. (2005). How to assess physical activity? how to assess physical fitness? European Journal of Cardiovascular Prevention and Rehabilitation: Official Journal of the European Society of Cardiology, Working Groups on Epidemiology & Prevention and Cardiac Rehabilitation and Exercise Physiology, 12(2), 102e114. [ Links ]
Received 21 June 2015
Accepted 14 July 2016
Available online 6 October 2016
* Corresponding author. P.O. Box 12651, Hatfield, 0028, South Africa. Fax: +27 12 362 3369
E-mail address: Christa.jansevanrensburg@up.ac.za (D.C. Janse van Rensburg).
Peer review under responsibility of Johannesburg University.

