










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 n.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.06.004
FULL LENGTH ARTICLE
Uterine artery Doppler screening as a predictor of pre-eclampsia
Yasmin CasmodI, *; Barbara Van DykI; E. NicolaouII
IDepartment of Radiography, Faculty of Health and Sciences, University of Johannesburg, Johannesburg, South Africa
IIDepartment of Obstetrics and Gynaecology, Faculty of Health Sciences, University of the Witwatersrand, South Africa
ABSTRACT
Hypertensive disorders represent the second most common cause of maternal death, affecting 5-10% of pregnancies worldwide and accounting for 19% of maternal deaths in South Africa. Pre-eclampsia is believed to develop from inadequate trophoblast invasion of the maternal spiral arteries. Doppler imaging permits non-invasive evaluation of the uteroplacental circulation and is invaluable in the management of high risk pregnancies.
A prospective quantitative experimental study tested the hypothesis that uterine artery (UA) spectral Doppler screening is able to identify patients at risk for developing pre-eclampsia.
Convenience sampling allowed for the recruitment of 144 patients (11-14 weeks gestation) who attended the antenatal clinic at Rahima Moosa Mother and Child Hospital between November 2008 and July 2010. A complete record of 121 participants was available for the final analysis.
The results of this study revealed that 7 (5.8%) participants developed pre-eclampsia. Race was identified as the most significant independent variable with an odds ratio of 1.5; 26 and 9 to 1 for developing PET in the 1st, 2nd and 3rd trimesters respectively.
Uterine Artery Doppler is promising. An ultrasound screening programme in high risk pregnant women would offer clinicians the opportunity to pre-empt the disease before it manifests clinically.
Keywords: High risk pregnancy; Pre-eclampsia; Uterine artery doppler; Uterine artery notching; Pulsatility index
1. Introduction
A key aim of antenatal care is to identify and manage pregnancies at risk for complications (Kurdi, Campbell, Aquilina, England, & Harrington, 1998). Hypertensive disorders represent the second most common cause of maternal death, affecting 5-10% of all pregnancies worldwide (Wolde, Segni, & Woldie, 2011), and accounting for 19% of maternal deaths in South Africa (Moodley, 2010).
Normal placentation is achieved through successful trophoblast invasion of the maternal decidua and myometrium via the dilated spiral arteries. In the process, a low resistance vascular bed with a high blood flow is created (Ozkaya, Ozkan, Ozeren, & Corakci, 2007). Physiological changes during pregnancy convert the spiral arteries from small muscular arteries to dilated uteroplacental vessels, which are able to accommodate the hemodynamic forces of pregnancy (Swanepoel, 2004). Unsuccessful trophoblast invasion, with consequent under perfusion of the placenta, leads to the release of hormones into the maternal circulation which is believed to be the underlying mechanism for the development of pre-eclampsia (Yu, Papageorghiou, Parra, Palma Dias, & Nicolaides, 2003).
Doppler ultrasound is an invaluable tool in the management of high-risk pregnancies. Direct assessment of trophoblast invasion in human pregnancy is not possible; however, the use of Doppler imaging permits non-invasive evaluation of the uteroplacental circulation by comparing systolic and diastolic waveforms (Ghidini, Locatelli 2008), (El-Hamedi, Shillito, Simpson, & Walker, 2005). In recent years the question whether uterine artery (UA) spectral Doppler analysis could be used as a screening tool to predict pre-eclampsia before the clinical onset of the disease has thus been asked. In previous studies the clinical value of UA Doppler has been promising (Harrington, Fayyad, Thakur, & Aquilina, 2004, p. 50) in the prediction of severe adverse outcomes in patients at high risk for pre-eclampsia (El-Hamedi et al., 2005).
There is evidence to support the belief that trophoblast invasion is maximal in the first trimester (Melchiorre, Leslie, Prefumo, Bhide, & Thilaganathan, 2009, p. 524) and that pre-eclampsia, deriving from a relative failure of this event, validates Doppler evaluation of the UA as from the first trimester of pregnancy (Melchiorre, Wormald, Leslie, Bhide, & Thilaganathan, 2008). This screening test, performed as an adjunct to routine ultrasound examinations, does not involve significant extra costs and can identify a cohort of patients who will benefit most from increased surveillance during pregnancy (Papageorghiou & Leslie, 2007).
The aim of this article is to document our experience in demonstrating the sensitivity of UA spectral Doppler screening in the prediction of pre-eclampsia.
2. Materials and methods
A prospective quantitative experimental study was conducted to test the hypothesis that UA spectral Doppler screening is able to identify patients at risk of developing pre-eclampsia.
A convenience sampling method was applied by recruiting all patients (between 11 and 14 weeks gestation) who attended the antenatal clinic at Rahima Moosa Mother and Child Hospital between November 2008 and July 2010. Patients with the following conditions were excluded from the study:
• Multiple gestations, as these pregnancies are known to have a higher incidence of placental insufficiency.
• Fetal abnormalities, as the possibility that those patients might opt for a pregnancy termination existed and data collection would thus be incomplete.
• Patients on treatment for hypertensive disorders - results from those patients would not provide a true reflection as the patients were already on medication.
After explaining the objectives of the study, written informed consent was obtained from the women who agreed to participate. Once a viable intra-uterine pregnancy had been confirmed, UA spectral Doppler assessment was performed on a GE Vivid 3 ultrasound unit, using a transabdominal approach. To ensure consistency of results, the researcher was the only person performing the scans and the ultrasound unit was serviced and calibrated on a regular basis.
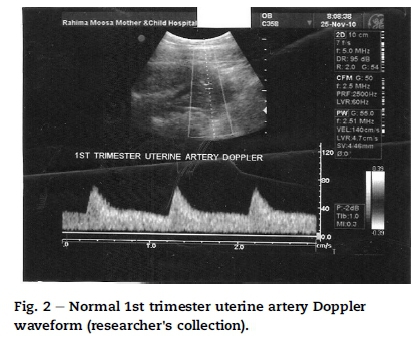
The probe was placed lateral to the uterus and the transducer gently tilted medially until the UA was identified where it crossed over the external iliac artery (Fig. 1). The sample gate was placed over the entire diameter of the artery and pulsed wave Doppler was used to obtain three consecutive UA waveforms. The pulsatility index (PI) was then measured bilaterally.

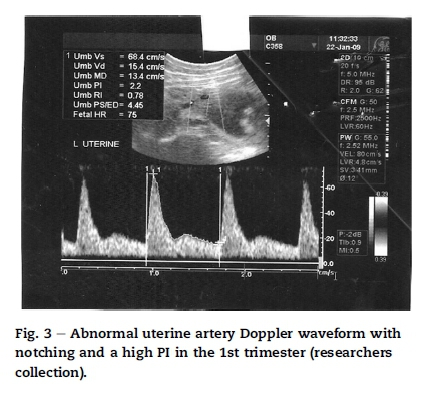
The Doppler assessment was repeated during the 22-24 week scan and again between 28 and 32 weeks gestation. Ultrasound criteria for demonstration of high resistance flow were guided by Gomez et al. (2008, Table 1, p. 130). and current practice in the Fetal Medicine unit at Chris Hani Baragwanath Hospital (Nicolaou (personal communication), 2012). The presence of UA notching and a PI > 1.5 during the first trimester were considered indicative of increased vascular resistance in the placental bed. Even though notching may be considered normal in the first and early second trimester, it was recorded to facilitate the comparison of variables (Table 2).
Fig. 2 demonstrates a normal UA waveform in the first trimester while Fig. 3 demonstrates a high resistance waveform with notching obtained in the first trimester.
Biographical data, fetal gestational age, wellbeing and growth and uterine artery Doppler indices were routinely recorded and compared for each patient.
Descriptive and inferential statistical analyses were performed with SPSS version 18.0 and presented as frequencies, ranges, cross-tabulations and odds ratios. Calculating odds ratios is a useful way of using information in cross-tabulations when one dimension of the table is an outcome of interest. The odds ratio can be defined as the likelihood of an event occurring in one group compared to the likelihood of it occurring in another group.
The study was approved by the Ethics Committees of the Faculty of Health Sciences, University of Johannesburg and the CEO of Rahima Moosa Mother and Child Hospital. Participation was voluntary and anonymity was ensured by means of a research number. Scans were performed according to standard protocols and safe ultrasound practice was maintained at all times. If abnormal uterine artery Doppler waveforms were detected, the referring clinician was informed immediately.
3. Results
A total of 144 participants were recruited; however, 23 participants had to be excluded from the final analysis due to incomplete data. Records of 121 participants were thus available for the final analysis.
• For the purpose of this study the predictor variable was defined as the Doppler ultrasound examination, the dependent variables as the uterine artery PI and notching, while the development of PET was defined as the outcome variable. These are influenced by race, maternal age, BMI, parity, previous history of PET and gestational weeks at time of delivery and are the independent variables.
3.1. Predisposing factors
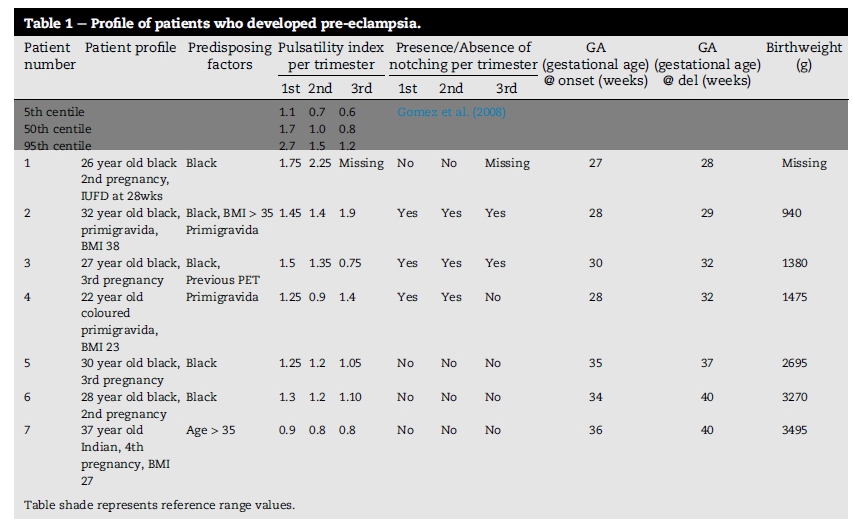
Of the seven (5.8%) patients who developed pre-eclampsia, five (73%) were black, one (14%) was coloured and one (14%) was Indian. The majority (57%) were in their teens or twenties, while two (29%) were between the ages of 30 and 34, and one (14%) was of advanced maternal age (>35). A single participant had a previous pregnancy complicated by hypertension, four (57%) had no previous complications, while two (29%) were primigravidas.
3.2. PI values
In our study, first trimester PI values ranged between 0.9 and 1.75 and therefore none was above the 95th centile as suggested by Gomez et al. (2008). However, two had a PI value of 1.5 or above. In the second trimester, only one out of the seven patients had a PI value above the 95th centile, measuring 2.25, while in an additional four cases, a PI value above the 50th centile was measured. In the third trimester, two out of the seven patients had a PI value above the 95th centile, while two additional cases had PI values above the 50th centile.
3.3. Uterine artery notching
Three out of the seven patients who developed pre-eclampsia had UA notching in the first and second trimesters and two out of the seven in the third trimester. The outcome for one patient was not available due to the fact that she delivered at 27 weeks gestation.
3.4. Odds ratios
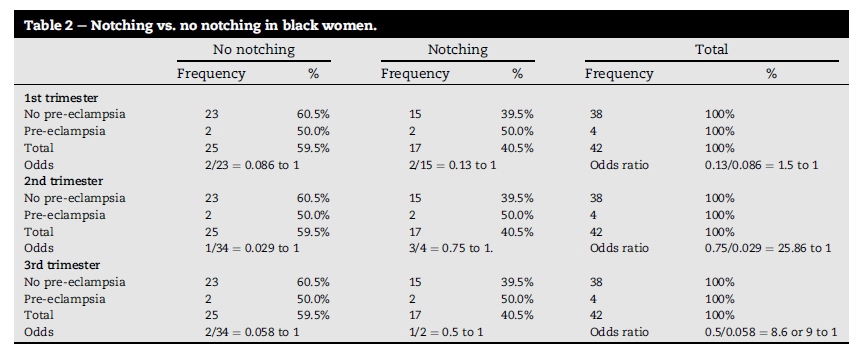
Race is strongly associated with the development of PET and since it seemed to be the most significant independent variable in the study, the odds ratio for developing PET was calculated for black participants only.
The odds for black women of developing pre-eclampsia were calculated as follows:
1st trimester
1. Odds without notching: 2/23 = 0.086 to 1.
2. Odds with notching: 2/15 = 0.13 to 1.
3. Odds ratio notching vs. no notching: 0.13/0.086 = 1.5 to 1.
2nd trimester
1. Odds without notching: 1/34 = 0.029 to 1.
2. Odds with notching: 3/4 = 0.75 to 1.
3. Odds ratio notching vs. no notching: 0.75/0.029 = 25.86 or 26 to1.
3rd trimester
1. Odds without notching: 2/34 = 0.058 to 1.
2. Odds with notching: 1/2 = 0.5 to 1.
3. Odds ratio notching vs. no notching: 0.5/0.058 = 8.6 or 9 to 1.
Black women with notching in the first trimester are thus 1.5 times, in the second trimester 26 times and in the third trimester 9 times more likely to develop pre-eclampsia than those without notching.
4. Discussion
4.1. Incidence of pre-eclampsia
Hypertensive disorders complicate approximately 5-10% of pregnancies worldwide (Wolde et al., 2011, p. 147). In our study 5.8% of the population developed pre-eclampsia, demonstrating the magnitude of the problem in Gauteng, South Africa.
4.2. Predisposing factors
As is evident from previous studies, black women have a higher incidence of developing pre-eclampsia than other race groups (Assis, Viana, & Rassi, 2008, p. 15). This was confirmed in our study with 72% of the patients who developed pre-eclampsia being black.
4.3. PI values
The mean first trimester PI value of 1.3 in our study is considerably lower than 1.7 (50th centile) proposed by Gomez et al. (2008), however, in clinical practice a first trimester PI value of >1.5 is deemed as elevated and warrants monitoring (Nicolaou (personal communication), 2012). With only one of seven PI values above Gomez's 50th centile value in the first trimester, five in the second trimester and four in the third trimester, it can be concluded that PI values did not perform well as a predictor of pre-eclampsia when Gomez's guidelines or a cut-off value of 1.5 were used.
4.4. Uterine artery notching and odds ratios
The presence of notching in the second trimester has been associated with a high probability for developing pre-eclampsia (Hernandez-Andrade et al., 2002, p. 440). In the study, UA notching predicted the disease in three out of the four most severe cases who developed PET before 32 weeks, in both the first and second trimesters. This compares favourably with the suggestion that the clinical value of UA Doppler looks promising in the prediction of severe adverse outcomes in patients at high risk for pre-eclampsia (Harrington et al., 2004, p. 50) (El-Hamedi et al., 2005, p. 142).
Since the majority (73%) of pre-eclamptic patients were black, cross-tabulations were completed using notching as a predictor of pre-eclampsia in the first, second and third trimesters in the black population. Once again the presence of notching in the second trimester was the best predictor for the development of pre-eclampsia, with an odds ratio of 26:1. Odds ratios for black women with notching did not fare as well in the other trimesters, with a risk increase of 1.5:1 in the first and 9:1 in the third trimesters.
5. Implications for practice
UA Doppler screening is beneficial to patients at high risk for developing PET so that preventative therapies can be initiated early in pregnancy (Mcleod, 2008, p. 727); however, as the researcher is not a clinician, treatment options are not discussed in this paper.
Although the researcher's findings do not promote routine UA Doppler screening in the general population, they suggest an association between severe PET, requiring delivery before 32 weeks gestation, and PI values > 1.5 and/or uterine artery notching in the second trimester. In an attempt to identify women at high risk for severe PET early, it is recommended that the following factors be considered as inclusion criteria in a first trimester screening programme:
1) Primigravidas
2) Patients with a BMI >30
3) Patients with a previous history of PET
4) Patients with pre-existing hypertension
While other studies advocate for the inclusion of biochemistry and blood pressure (BP) readings in a screening programme, the researcher, as a sonographer, only attempted to develop an ultrasound screening protocol. The combination of low PAPP A and abnormal UA Doppler waveforms almost invariably predicts adverse pregnancy outcomes (Nicolaou (personal communication), 2012); therefore, when used together, biochemistry and ultrasound screening have the ability to improve the sensitivity of screening for PET.
The following ultrasound guidelines are recommended when screening for PET (Fetal medicine unit, Chris Hani Baragwanath Hospital).
5.1. First trimester screening
1. Determine the gestational age for monitoring of fetal growth.
2. UA Doppler assessment.
• Patients with PI values > 1.5 and uterine notching only require BP monitoring on a two-weekly basis.
5.2. Second trimester follow-up
1. Routine fetal anatomy scan at 22 weeks gestation.
2. Liquor volume assessment for signs of oligohydramnios.
3. Biometric fetal growth monitoring.
4. UA Doppler assessment.
• Patients with PI values < 1.0 (50th centile) and/or absent notching do not need a follow-up third trimester scan.
5. Patients who screen positive for PET, with ultrasound or clinically, should be followed up in the third trimester at 28 weeks.
5.3. Third trimester follow-up
1. Biometric growth monitoring for signs of fetal growth restriction (FGR).
2. Liquor volume assessment for signs of oligohydramnios.
3. UA Doppler assessment. Patients with:
a) clinical signs of PET and/or
b) PI values of > 0.8 (50th centile) and/or
c) UA notching and/or
d) ultrasound features in keeping with FGR
Should be followed up with ultrasound on a four-weekly basis as follows:
1. Biometric growth assessment for signs of FGR.
2. Liquor volume assessment for signs of oligohydramnios.
3. Umbilical artery Doppler assessment for signs of increased placental resistance.
a. Umbilical artery resistance > 0.75 requires two-weekly monitoring.
b. Umbilical artery absent or reversed end diastolic flow requires Doppler monitoring every second day:
I. Umbilical artery for signs of deterioration
II. Middle cerebral artery for signs of brain sparing
III. Ductus venosus for signs of reversed flow
4. Time of the delivery is determined by the clinician, based on ultrasound findings and the clinical condition of the patient.
5.4. Limitations of the study
Due to a lack of patients presenting at the antenatal clinic early in pregnancy, the study was completed on the available data. The small numbers may hamper generalisation of the results to other populations.
Since the hospital is situated in a predominantly coloured community, the majority of participants were coloured, representing only 9% of the South African population (Mid year population estimates, n.d.).
Very few participants had their BMIs recorded and therefore BMI could not be proven as a strong predisposing factor for PET as seen in other studies.
Furthermore, the interpretation of PI values in the cases with PET may be problematic since the nomogram employed in this study was not specifically developed for a South African population.
6. Conclusion
The findings of our study do not support the introduction of routine UA Doppler screening in all patients who attend the antenatal clinic at Rahima Moosa Hospital in Gauteng. Pre-eclampsia, however, remains the main cause for perinatal morbidity and mortality in South Africa. Since an abnormal Doppler flow pattern and resistance to flow in the UA are strong predictors of the most severe cases of PET, it is recommended that patients at high risk for these adverse pregnancy outcomes be offered ultrasound screening. Since biochemical screening is not readily available in the South African public sector, clinicians have to depend on the clinical manifestation of the disease before taking action. An ultrasound screening programme in pregnant women who are at high risk of developing PET would offer clinicians the opportunity to pre-empt the disease before it manifests clinically by initiating treatment as from the first trimester.
A larger prospective multicentre trial in South Africa is long overdue and guidelines based on the outcome of our study can be used to determine the value of routine UA Doppler screening in Gauteng in a high-risk population.
References
Assis, T. R., Viana, F. P., & Rassi, S. (2008). Study on the major maternal risk factors in hypertensive syndromes. Arquivos Brasileiros de Cardiologia, 91(1), 11e16. [ Links ]
El-Hamedi, A., Shillito, J., Simpson, N. A. B., & Walker, J. J. (2005). A prospective analysis of the role of uterine artery Doppler waveform notching in the assessment of at-risk pregnancies. Hypertension in Pregnancy, 24(2), 137e145. [ Links ]
Ghidini, A.,&Locatelli, A. (2008).Monitoring of foetalwell-being: Role of uterine artery Doppler. Seminars in Perinatology, 32, 258e262. [ Links ]
Gomez, O., Figueras, F., Fernandez, S., Bennasar, M., Martinez, J. M., Puerto, B., et al. (2008). Reference ranges for uterine artery mean pulsatility index at 11-41 weeks gestation. Ultrasound in Obstetrics and Gynaecology, 32, 128e132. [ Links ]
Harrington, K., Fayyad, A., Thakur, V., & Aquilina, J. (2004). The vale of uterine artery Doppler in the prediction of uteroplacental complications in multiparous women. Ultrasound in Obstetrics and Gynaecology, 23, 50e55. [ Links ]
Hernandez-Andrade, E., Brodszki, J., Lingman, G., Gudmundsson, S., Molin, J., & Marsal, K. (2002). Uterine artery score and perinatal outcome. Ultrasound in Obstetrics and Gynaecology, 19(5), 438e442. [ Links ]
Kurdi, W., Campbell, S., Aquilina, J., England, P., & Harrington, K. (1998). The role of colour Doppler imaging of the uterine arteries at 20 weeks gestation in stratifying antenatal care. Ultrasound in Obstetrics and Gynaecology, 12, 339e345. [ Links ]
Mcleod, L. (2008). How useful is uterine artery Doppler ultrasonography in predicting pre-eclampsia and intrauterine growth restriction. Canadian Medical Association Journal, 178(6), 727e729. [ Links ]
Melchiorre, K., Leslie, K., Prefumo, F., Bhide, A., & Thilaganathan, B. (2009). First trimester uterine artery Doppler indices in the prediction of small for gestational age pregnancy and intrauterine growth restriction. Ultrasound in Obstetrics and Gynaecology, 33, 524e529. [ Links ]
Melchiorre, K., Wormald, B., Leslie, K., Bhide, A., & Thilaganathan, B. (2008). First trimester uterine artery Doppler indices in term and preterm pre-eclampsia. Ultrasound in Obstetrics and Gynaecology, 32, 133e137. [ Links ]
Mid year population estimates. (n.d.). Retrieved from http://www.statssa.gov.za/publications/P0302/P03022011.pdf. [ Links ]
Moodley, J. (2010). Maternal deaths associated with eclampsia in South Africa: Lessons to learn from the confidential enquiries into maternal deaths, 2005-2007. South African Medical Journal, 100(11), 717e719. [ Links ]
Nicolaou, E. (personal communication, 2012). [ Links ]
Ozkaya, U., Ozkan, S., Ozeren, S., & Corakci, A. (2007). Doppler examination of the uteroplacental circulation in early pregnancy: Can it predict adverse outcome? Journal of Clinical Ultrasound, 35(7), 382e386. [ Links ]
Papageorghiou, A. T., & Leslie, K. (2007). Uterine artery Doppler in the prediction of adverse pregnancy outcome. Current Opinion in Obstetrics and Gynaecology, 19(2), 103e109. [ Links ]
Swanepoel, H. S. (2004). Uterine artery doppler. Obstetrics and Gynaecology Forum, 14(2), 4e9. [ Links ]
Wolde, Z., Segni, H., & Woldie, M. (2011). Hypertensive disorders of pregnancy in Jimma University Specialised hospital. Ethiopian Journal of Health Science, 21(3), 147e154. [ Links ]
Yu, C. K. H., Papageorghiou, A. T., Parra, M., Palma Dias, R., & Nicolaides, K. H. (2003). Randomised controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks gestation. Ultrasound in Obstetrics and Gynaecology, 22, 233e239. [ Links ]
Received 16 August 2015
Accepted 13 June 2016
Available online 16 September 2016
Peer review under responsibility of Johannesburg University.
E-mail addresses: yasminc@uj.ac.za, yasmin@polka.co.za (Y. Casmod).
* Corresponding author.


{kind=link}
{kind=link}