










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 no.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.07.002
FULL LENGTH ARTICLE
Critical thinking ability of 3rd year radiography students
Tracey PieterseI, *; Heather LawrenceII; Hesta Friedrich-NelIII
IMIRS Department, Faculty of Health Sciences, University of Johannesburg, John Orr Building, Room 6305b, Doornfontein Campus, Corner Siemert and Beit Streets, Doornfontein, Johannesburg, 2000, South Africa
IIMIRS Department, Faculty of Health Sciences, University of Johannesburg, John Orr Building, Room 6306e, Doornfontein Campus, Corner Siemert and Beit Streets, Doornfontein, Johannesburg, 2000, South Africa
IIIDepartment of Clinical Sciences, Faculty of Health and Environmental Sciences, Central University of Technology, Free State (CUT), Private Bag X20539, Bloemfontein, 9300, South Africa
ABSTRACT
BACKGROUND: eveloping the critical thinking skills of student radiographers is imperative in an era of rapidly advancing technology. The status of the students' ability to demonstrate critical thinking skills needed to be explored for the Department of Radiography at a comprehensive university to determine if a more explicit curriculum was needed to facilitate these skills.
AIM: The aim of this article is to present results of a study conducted to determine the critical thinking ability of 3rd year radiography students at a Comprehensive University in South Africa.
METHOD: The research study used a descriptive exploratory design to collect both quantitative and qualitative data. Quantitative data was collected by scoring the participants ability to think critically when answering clinical scenarios posed in the form of vignettes given to the students under assessment conditions. The qualitative data was generated by in-depth field notes made inductively by the researcher.
RESULTS: The findings of this study indicated that the majority of participants demonstrated a minimal ability to think critically.
CONCLUSION: The study results imply that in order to improve critical thinking skills of student radiographers, there is a need for curriculum adjustment, to nurture and encourage these skills. It is recommended that facilitators adopt methods to integrate these skills in the curriculum.
Keywords: Critical thinking; Radiography
1. Introduction
The South African Qualifications Authority (SAQA) have published critical cross-field outcomes (SAQA, 2012) that need to be achieved by students in higher education, in addition to the programme specific outcomes. Critical thinking is listed as one of the 12 critical cross-field outcomes, but research in critical thinking in a radiography context in South Africa is lacking, making it valid to question the ability of these students to achieve this skill.
Critical thinking goes beyond merely acquiring knowledge. It is thinking at a higher level, requiring the use of gained knowledge within context, taking into account various factors, justifying actions and reflecting upon those actions (Castle, 2006, Castle, 2011a, Chee Choy and San Oo, 2012 and Jones, 2012). It is important for students to possess critical thinking skills in order to problem solve, become reflective practitioners and base decisions on sound evidence (Agwu et al., 2007, Castle, 2009 and Ugwu et al., 2010).
The aim of this article is to present the results of a study conducted to determine the critical thinking ability of 3rd year radiography students.
1.1. Background and problem statement
In the Department of Radiography at a comprehensive university in South Africa, students are assessed according to Bloom's taxonomy of learning. This is a model which structures learning and thinking from the very basic foundation of knowledge and understanding (skills assessed in first year students), to more complex and deeper thinking and learning of evaluation and synthesis (skills assessed in final year students) (Bloom, 1984 and Forehand, 2012). The higher levels of learning (evaluation and synthesis) require the use of critical thinking skills, and this is important since demonstrating critical thinking is paramount in modern medicine where health professionals are expected to become reflective practitioners and evidence-based caregivers (Castle, 2006).
No specific curriculum is in place in the Department of Radiography at this specific university to nurture and encourage critical thinking in students. By the time students reach their third and final year within the National Diploma course, it is assumed that they have gained these skills along the way, through tutorials, work-integrated experiential learning and traditional lecture-based teaching. Although no specific curriculum exists within the Department of Radiography for teaching and learning of critical thinking, assessments given to students progress from the lower levels of learning, which include knowledge and understanding of information in first year, to the higher levels of learning, which include analysis, synthesis and evaluation in third year.
At the time of the study the Department of Radiography was preparing to introduce a new curriculum as per the recently registered four year, 480-credit professional bachelor's degree (SAQA, 2012). Evolving from a three year National Diploma (National Qualifications Framework (NQF) exit level 6), to a four year professional degree (NQF exit level 8). This degree aims to develop students who can demonstrate an ability to identify, analyse and deal with complex and/or real-world problems and issues, using evidence-based solutions and theory-driven arguments (SAQA, 2012), as well as an ability to critically analyse, synthesize and produce an independent evaluation of data (SAQA, 2012). It has, however, been noted in radiography literature that whilst students are expected to demonstrate critical thinking skills, the required skills are not adequately defined, taught or assessed (Castle, 2009). A study was therefore warranted within the Diploma driven environment to give the department of radiography the opportunity to determine the ability of 3rd year graduating students to think critically so that interventions could be implemented into the new Degree programme to improve these skills if it was found that these skills were lacking in the current teaching paradigm.
In a South African context, critical thinking skills among radiography students has not been assessed previously, and it is therefore an unknown factor. Furthermore, guidelines to facilitate the development of these specific skills in a South African radiography context are not available and cannot be developed until the current status of critical thinking in radiography students is known. The question that arose was "to what extent could 3rd year radiography students think critically and how can the design and delivery of the curriculum be adapted to make provision for and best facilitate the teaching and learning of these skills?".
1.2. Research aim
This article aims to present the results of a study conducted to determine the critical thinking ability of 3rd year radiography students. A follow on to this article will be written to present guidelines for the facilitation of critical thinking in radiography students.
2. Literature review
Critical thinking skills are imperative for radiography students, who, in the modern era are faced with a challenge of having not only to learn factual information, but also being taught how to make sense of the amount of information that is available to them and to enable them to synthesize information, to apply the information in order to problem solve and to reflect upon their judgement within a given clinical context (Kowalczyk and Leggett, 2005, Mc Inerney and Baird, 2016 and Spencer, 2008).
In health care, the core of critical thinking can be defined as the ability to analyse, evaluate, reflect, examine information in order to form self-regulatory and purposeful judgements within context, and problem solve (Facione and Facione, 1996 and Facione, 2011). Critical thinkers will therefore examine information before evaluating all the evidence and make a judgement based on the evidence (Mann, 2012 and Castle, 2011b). Thus, a critical thinker takes into account context, various concepts, methods and criteria, before making a decision based on clinical evidence (Castle, 2006, Chee Choy and San Oo, 2012, Facione, 1990 and Jones, 2012). Low application of critical thinking skills can be linked to misinterpretation, mistaken evaluation and rash generalization within the clinical radiography environment (Agwu et al., 2007). Pathology may be missed or misdiagnosed on poor quality diagnostic radiographs, placing the patient at great risk (Kowalczyk & Leggett, 2005). Furthermore, radiography training programmes worldwide are increasingly driven to produce graduates with academic knowledge which can be incorporated into a rapidly changing clinical environment (Castle, 2011b and Ng et al., 2008).
Critical thinking causes individuals to constantly improve their skills for personal and professional growth, thus enabling health care workers to problem solve and make better decisions in the clinical environment (Popil, 2011 and Vacek, 2009). In a South African setting, following a worldwide trend, critical thinking is integral in paving the way for radiographers to develop the thinking skills necessary for extended roles within the clinical environment to become a reality (Mc Inerney & Baird, 2016). To encourage the development of critical thinking skills will require radiography educators to produce graduates who think beyond routines and protocols, reflect in daily practice with the ability to differentiate good practice from ineffective practice and therefore apply self-correction (Agwu et al., 2007, Kowalczyk and Leggett, 2005 and Mc Inerney and Baird, 2016).
The purpose, therefore, of teaching critical thinking in radiography is to keep up with the expansion of scientific knowledge, and to integrate knowledge of technology, science and pathology so as to competently perform duties within an imaging department which ultimately lead to improved patient care and patient management as a whole (Mc Inerney & Baird, 2016). Teaching strategies that improve critical thinking are those strategies utilized by educators to encourage student participation and inquiry, as opposed to traditional lecture methods (Wessel & Williams, 2004). In the past, radiography education in tertiary education institutions was considered to be 'teacher centred', where the instructor provides the theory, and students passively absorb the information, with little interaction. This 'lecture-based' education strategy does not challenge students to enquire, research, or independently review topics; therefore, little transfer of knowledge relating to the clinical environment is achieved. Students ultimately lose their motivation, experience overload and struggle to apply the knowledge in the clinical setting at a later stage (Gqweta, 2012, Kowalczyk and Leggett, 2005, Mann, 2012 and Raymond and Profetto-McGrath, 2005).
It is therefore necessary to design a curriculum in such a way, as to develop critical thinking skills in radiography students, and to facilitate the application thereof in the clinical environment (Agwu et al., 2007, Chee Choy and San Oo, 2012, Mc Inerney and Baird, 2016, Tufekci et al., 2011 and Yildirum et al., 2011). In addition, it is also necessary to enlighten facilitators on the implementation and assessment of critical thinking skills and the need to teach such skills, and to guide facilitators carefully in the process whilst developing their own critical thinking skills, since they themselves may not possess high critical thinking ability (Chee Choy and San Oo, 2012 and Mann, 2012).
3. Methodology
3.1. Design
The research study used a descriptive exploratory design to collect both quantitative and qualitative data. Quantitative data was collected by scoring the participants ability to think critically when answering clinical scenarios posed in the form of vignettes given to the students under assessment conditions. The qualitative data was generated by in-depth field notes made inductively by the researcher. This was achieved by reading the participants' responses to each vignette, reflecting upon the data and rereading the response. This enabled the researcher to make in-depth field notes using an inductive reasoning process (Creswell, 2013) to reflect on the logic of the students responses to each vignette. The inductive reasoning process was framed by reflecting on the students responses whilst referring to the scoring rubric and 4-point Likert scale for each vignette.
3.2. Data collection tool
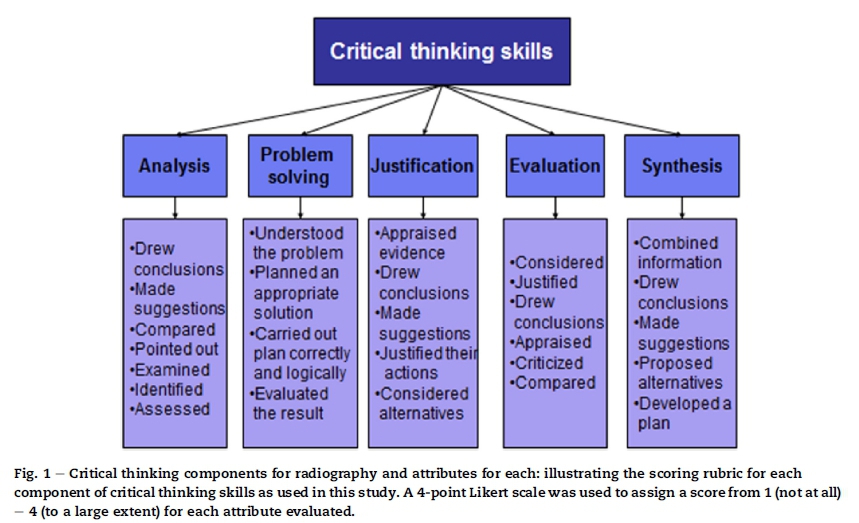
The ability of students to think critically was assessed by asking students to pose a solution to a vignette (in the form of a clinical scenario) designed to extract each component of critical thinking identified in this study (as illustrated in Fig. 1).
For the purpose of this study, critical thinking skills were divided into five components namely analysis, problem solving, justification, evaluation and synthesis and each assessed using a purposefully constructed vignette considered integral to radiography. The five components of critical thinking were selected from the work of Facione (2011) and from Castle (2006) as the pioneer in critical thinking for radiography. The components selected were found to be appropriate in a South African context as they related to the critical crossfield outcomes described for the South African radiography curriculum which require graduates who can demonstrate an ability to identify, analyse and deal with complex and/or real-world problems and issues, using evidence-based solutions and theory-driven arguments as well as an ability to critically analyse, synthesize and produce an independent evaluation of data (SAQA, 2012).
Before formulating the vignettes and scoring rubric, an extensive literature search was conducted utilizing the following databases: Academicsearch complete, AMED, CINAHL, Ebscohost, Education, ERIC, Health Source, MEDLINE, Science Direct, Africa Wide Information, PsychINFO, and using the keywords: assessment of critical thinking skills, critical thinking skills. Each vignette was specifically designed in consultation with an expert from the University's Faculty of education, with the intention of extracting a particular component critical thinking as identified in the literature (Anderson and Krathwohl, 2001, Castle, 2006, Castle, 2009, Facione, 2011, Freeman and Lewis, 1998, McMullen and McMullen, 2009 and Peirce, 2006).
The authors are experienced academics in the field of radiography and health education. This ensured that the use of each vignette and its measurement were appropriate and applicable to a specific critical thinking component identified, and based on the theoretical and practical knowledge that the student had gained in order to answer the given vignette.
For each critical thinking component, a list of attributes (as shown in Fig. 1) was used as a guide to assess the participants' ability to answer each of the five vignettes. The researcher scored the students' ability to demonstrate a particular critical thinking component according to the attributes identified within each component using a Likert scale scoring from 1 (not at all) to 4 (to a large extent). Field notes were then generated and analysed qualitatively to identify themes and patterns based on the captured field notes.
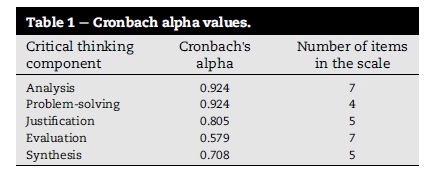
Statistical analysis of Cronbach's coefficient alpha was performed for each of the critical thinking components identified and measured in this study as an indication of the reliability and was found to be within an acceptable range according to the number of items within the scale (Pallant, 2007). As seen in Table 1, Cronbach alpha values range from 0 to 1, with higher values indicating greater reliability (Pallant, 2007).
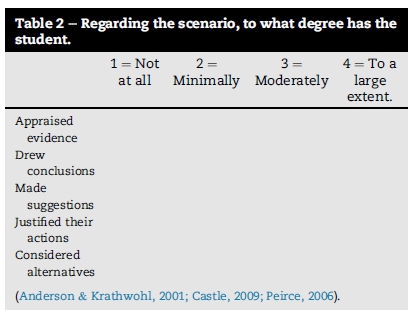
One vignette (in the form of a complex clinical scenario) was used per critical thinking component in order to extract the attributes identified to the specific critical thinking component. Each component was then assessed by identifying the degree to which the participant demonstrated the listed attributes identified for each component within their response, using the Likert scale as a guide (1 = not at all, 4 = to a large extent).
An example of a vignette used to extract the critical thinking component of justification is shown below.
3.2.1. Justification
An 11 year old patient who has been involved in a motor vehicle accident presents to the emergency department with severe trauma to the right leg. On examination, it is noted that there is no femoral pulse on the right side. What imaging modality/ies would be required in this situation, and justify your choice/s. The rubric used for this scenario is shown in Table 2 below:
3.3. Population and sample
The population for this study included all diagnostic radiography students registered for the Radiographic Practice III module (offered in the 3rd year of the National Diploma course) at the time of the study, at a comprehensive university in South Africa (N = 73). These students were purposely selected to determine their ability to demonstrate critical thinking skills as expected at this level of study. Being final year students, this group of students would be graduating and are required to possess critical thinking skills as set out by SAQA in order to work effectively within the healthcare team.
The sample for the study included voluntary participants within the population group. The total number of students who completed each critical thinking vignette varied due to their availability and willingness to participate. The total number of students participating in the study for each critical thinking skill can be seen in Table 3 below:
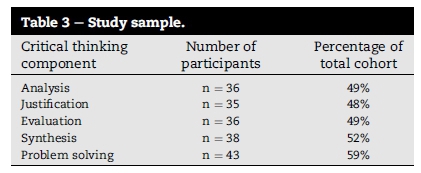
It should be noted that the sample size for each critical thinking component differs due to different dates of data collection set aside for the assessment of each critical thinking component, and varying availability of students.
3.4. Data collection procedure
The data in this study was collected in 2010, and to date, there has been no similar study or any new data obtained on critical thinking ability of radiography students at this particular university. This data will therefore form a baseline in order for further studies on critical thinking within radiography once teaching strategies to encourage critical thinking. Before the start of the study, each participant was given a letter explaining the significance of the study, and explaining their voluntary participation, including an explanation regarding their choice to participate. Each participant received a number, which remained his/her participant number throughout the study.
Each vignette was given to participants and they were instructed to respond in writing. Participants were reminded of their voluntary participation in the study, and responses to vignettes were collected by the class representative, and handed back to the primary author. Each specific vignette was only given to the participants once the primary author was assured that the participants had gained the theoretical knowledge, as well as attended the practical demonstration relating to the topics in each vignette. This was to ensure that participants had the knowledge to relate to each vignette, and could answer the vignette based on the knowledge they had gained throughout the course thus far. To ensure that participants did not discuss their answers, the vignettes were handed out in an assessment environment, where an invigilator was present to ensure assessment conditions.
Upon completion of the five vignettes, each vignette was assessed by the primary author using the scoring rubric (as shown in Fig. 1) to assign a score from 1 to 4 for each of the attributes per critical thinking component assessed. No feedback was given to the students, but students were invited to contact the researcher if they wanted feedback on the results of the study.
3.5. Data analysis
Each critical thinking component was assessed by the primary author, being an expert in the field of diagnostic radiography with tertiary education experience. The scoring rubric for each vignette was designed in consultation with an expert in higher education after an extensive literature search relating to critical thinking scoring rubrics. In addition the data was reviewed by an independent coder to reduce bias and increase reliability of the scoring. The numerical information from the Likert scale was used to generate the quantitative data which was then analysed statistically.
The qualitative data was analysed by the primary author as suggested by Creswell (2003) by coding the information captured in the field notes, generating themes from the codes and interpreting the meaning of the data. The qualitative data was further analysed independently by an independent coder to minimize bias and increase reliability and a consensus meeting held between the primary author and the independent coder before the generation of the final themes occurred.
The results of the quantitative data, therefore, were further supported by the qualitative data (Creswell, 2003).
3.6. Validity, reliability and trustworthiness
In order to ensure the validity of the vignettes, a field expert was consulted to verify the suitability of questions used prior to data collection. The self-designed measurement rubrics used in this study were also verified by a field expert once an extensive literature review, relating to critical thinking assessment rubrics, had been conducted. This ensured that the use of the vignettes and scoring rubric was appropriate and applicable to the critical thinking components identified, and based on the theoretical and practical knowledge that the student had gained in order to answer the vignette in the context of radiography.
An indication of the reliability of the rubric is the internal consistency of the tool. The most commonly used statistical measurement of internal consistency is Cronbach's coefficient alpha (Pallant, 2007). Statistical analysis of Cronbach's coefficient alpha was performed for each of the critical thinking skills identified and measured in this study. As indicated in Table 1 above, the lowest score for Cronbach's alpha was 0.579 and the highest 0.924. Taking into account that lower scores can be expected for scales with less than 10 items (Pallant, 2007) the Cronbach's alpha for this study proved to be acceptable.
Reliability was ensured for the purpose of this study through consultation with an independent coder who reviewed the scores allocated to each participant and the qualitative data collected. A consensus meeting between the primary author and the independent coder improved the reliability of the results of both the qualitative and the quantitative data.
The criteria used to establish trustworthiness in this study were identified by Lincoln & Guba's model of trustworthiness. These criteria are truth value, applicability, consistency and neutrality (De Vos, 2011 and Krefting, 1991). Truth value, in qualitative research, can be termed credibility (Babbie, 2010 and Krefting, 1991). The use of an independent coder ensured credibility within the current study, and minimized any bias (Babbie, 2010, Creswell, 2013 and Murphy and Yielder, 2010). Applicability is the extent to which findings of a study can be applied to other settings or groups, or to bigger populations. For this reason, both the vignettes and the scoring rubric used in the data collection procedure have been described to the reader. According to Lincoln & Guba's model of trustworthiness, applicability in qualitative research can be referred to as transferability. A sufficiently dense description of the setting and participants ensures transferability in this study (Creswell, 2013, Krefting, 1991 and Murphy and Yielder, 2010).
The use of an independent coder, also referred to as an external auditor, allows for an assessment of the qualitative data analysis or a code-recoding of results at the conclusion of the study in order to improve the trustworthiness of the study (Creswell, 2003 and De Vos, 2011).
3.7. Ethical considerations
Ethical clearance was given by the Ethics Committee of the Faculty of Health Sciences of the University concerned. Permission to conduct the study was obtained by the Head of the Department of Radiography at the university where the study was conducted. Participants were recruited once informed consent was obtained and confidentiality was ensured by assigning numbers to participants. Therefore confidentiality was ensured by refraining to refer to them by name during the data analysis process and data dissemination opportunities.
Right to equality, justice and protection from harm
All 3rd year radiography students were invited to participate in the study. Data collection procedures for this study did not involve any change to the assessment strategy of the 3rd year students.
Right to privacy, confidentiality and protection from harm
Special consideration was given to the participant's right to privacy and confidentiality. Research numbers were allocated to each participating student.
Right to freedom of choice
The participant's right to freedom of choice and expression was considered by allowing the participant the right to decide voluntarily whether to participate in the study and the right to withdraw at any time.
Informed consent
Signed informed consent was obtained from the participants following an explanation and purpose of the study. Permission from the HOD of Radiography to conduct the study was granted.
Due to the researcher's involvement as a lecturer in the Department of Radiography at this specific university, the researcher was not involved in the recruitment process of participants, nor in the collection of answers to vignettes.
4. Results
The quantitative data was generated by scoring the participants responses to the vignettes and analysed using the SPSS (version 15) programme to generate means and standard deviations for the scores achieved. The qualitative data was generated by extensive field notes written by the primary author as the vignettes were scored. Direct quotes by participants as well as the field notes produced will be used to inform the results.
4.1. Quantitative data
Table 4 indicates the total mean score for each critical thinking component identified in this study. The numbers of participants as well as the standard deviation are also displayed.
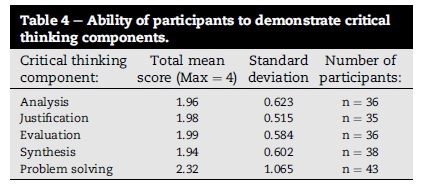
As shown in Table 4, the total mean for the critical thinking component of analysis is 1.96, indicating the minimal ability of participants to demonstrate this critical thinking component. The small standard deviation from the mean shows that the results tend to be clustered around the mean, indicating that in this study participants had minimal ability to demonstrate the critical thinking component of analysis.
The critical thinking component of justification, evaluation and synthesis yielded similar results, with a total mean score of 1.98 for the justification component, 1.99 for the evaluation component, and 1.94 for the synthesis component with a standard deviation of 0.515, 0.584 and 0.602 respectively.
The critical thinking component of problem solving demonstrates a similar situation with a total mean score of 2.32, but the standard deviation of 1.065 indicates that although the total mean score for participants to demonstrate the critical thinking component of problem solving showed minimal ability, some participants in this study achieved a moderate score, and some achieved a 'not at all' score, proving a greater degree of variable scoring for this particular critical thinking component.
4.2. Qualitative data
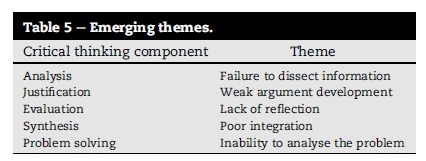
The quantitative data is further supported by the results of the qualitative data. Upon reflection of the field notes, the following themes were generated by the primary author (see Table 5). Each theme is briefly discussed in the section below:
4.2.1. Failure to dissect information
Participants were unable to dissect information and examine the information given in the vignette, in order to propose justifiable solutions. This theme became apparent when participants attempted to answer a vignette that called for participants to suggest, as an answer to the vignette posed, that the correct procedure to follow would be to start by referring the patient for basic imaging studies, to be followed by specialized studies, should the need arise. Instead, many participants were unable to link the patient history given in the vignette to justifiable imaging techniques.
Field notes generated by the primary author are shown below as well as verbatim quotes from participants.
Field Notes:
• Inability to identify area of concern therefore unable to suggest a reasonable course of action.
• Participant does not look at symptoms to indicate possible pathology and imaging necessary.
• Misses integral information given in the scenario.
Verbatim Quote:
"For the history of pyrexia, nausea and headaches a CT BRAIN pre- contrast may be performed. For pain in the right lower quadrant a CT ABDOMEN post contrast may be performed …"
Field Notes:
• Specialized techniques suggested without a first point of call for basic imaging.
• Holistic viewing of the patient not apparent.
• No specifics in procedures suggested, vague indirect answers.
• No justification of procedures relating to scenario.
Verbatim Quote:
"MRI and CT would be the modalities of choice. But ultrasound is the best modality due to the no need to use contrast media …"
Field Notes:
• Identification of area of concern whilst relating to scenario with possible imaging solutions suggested.
• Some justification of imaging suggested.
Verbatim Quote:
"Haematuria can due to glomerulonephritis. The mass can be tumor/cyst. The best imaging modalities are CT and MRI …"
4.2.2. Weak argument development
Participants were unable to develop an argument to justify a chosen answer. The vignette required the participants to justify their choice of imaging modality/ies given that the patient was a child, which necessitated adapting the chosen examinations accordingly. The answers given tended to state the image modalities, without being able to correctly justify the reason for each modality chosen. Field notes and verbatim quotes from participants are shown below.
Field Notes:
• Identification of correct procedures but no logic of thought and no justifications given for procedures.
• Non-specific answers given.
• No inclusion of what imaging choices may demonstrate.
• Listing of imaging modalities with no justification or argument development.
Verbatim Quote:
"Angio of the leg. Duplex Doppler. CT angio. (This was the complete answer.)"
Field Notes:
• Identifies possible impact of scenario and suggests imaging protocols.
• Does not justify imaging choice relating to scenario.
• Non-specific answers given.
Verbatim Quote:
"CT and MRI. This will demonstrate the involvement that the fracture has on the soft tissue and surrounding arteries and veins …"
4.2.3. Lack of reflection
Participants neglect to reflect upon and critique their own answers with regard to the vignette at hand. The vignette was developed to give participants an opportunity to equip a mining hospital with x-ray equipment. Students were required to justify the equipment chosen, evaluate the context, appraise, criticize and compare their choices. Participants were given the instruction to select either a CT or MRI unit as part of the equipment selected. Field notes and verbatim quotes from participants are shown below.
Field Notes:
• Failure to systematically answer the vignette in such a way as to ensure that each aspect is included.
• Failure to link answers to scenario given.
• Poor justification of choices relating to scenario.
Verbatim Quote:
"I will choose CT because its cheaper and does not take long …"
Field Notes:
• No reflection on answers given, in the context of the scenario and therefore failure to notice that the question is not answered correctly and in its entirety.
• Justifications not valid for the given scenario."
Verbatim Quote:
"MRI does not use radiation - CT - It is cheaper than MRI …"
4.2.4. Poor integration
The vignette called for the participants to suggest how radiographic techniques should be applied to ensure that good quality films are produced for a case involving imaging of a 12 week old baby with a history of clicking hips. Instead of adapting the radiographic technique, participants focused on patient positioning and did not consider measures such as limiting exposure, reducing time, and other methods of improving image quality. Field notes and verbatim quotes from participants are shown below.
Field Notes:
• Focus is on a narrow aspect of the question.
• Unable to link theory and adapt theory to the clinical scenario given.
• Unable to draw on theory and synthesize information to answer the question in its entirety. Limits response to positioning, neglecting to include technical factors required.
Verbatim Quote:
"AP - The baby will be laying supine on the bed - immobilized with strapping tape - Frog legs - 18 × 24 cm ffsc cassette."
Field Notes:
• Inability to integrate the entire scenario into their answer.
• Answers are limited due to main focus of answer on positioning rather than technical factors.
Verbatim Quote:
"Strap both legs with the belt for immobilization - Introduce myself to the pt. Reassure the patient …"
4.2.5. Inability to analyse the problem
The vignette called for the participants to demonstrate problem solving ability by determining that the lumbar spine examination requested did not correlate with the clinical symptoms of pins and needles in the arm, and by then suggesting that the correct examination would have been to x-ray the cervical spine. Compounding the problem was the fact that the patient was eight weeks pregnant. The field notes and verbatim quotes below support the generation of this theme.
Field Notes:
• Identification of problems that may exist in the vignette.
• Inabilityto identify solutions or solutions proposed are not feasible in the given scenario.
• Does not identify that the symptoms given are not related to the x-ray requested.
• Inability to tackle more than one clinical issue in a given scenario, so focuses on one aspect rather than the scenario as a whole.
Verbatim Quote:
"First I would advise her to go to another physician for second opinion, if she is willing I would do AP, lateral and oblique views for the lumbar spine, and a AP pelvis …"
Field Notes:
• A portion of the scenario attended to.
• Unable to identify a reasonable solution.
• Does not link the patient history to the clinical problem and therefore proposes an incorrect solution.
• Unable to link given history to correct imaging required to demonstrate the possible pathology.
Verbatim Quote:
Considering that I will never do the lumbar spine I will do only the right arm lateral to see if the pins are still aligned.
5. Discussion
Graduating radiography students are expected to display critical thinking skills in order to solve problems in the clinical environment, as well as to apply their knowledge gained within context in order to benefit the patient and the healthcare team. The minimal ability of students in the current study to think critically is supported by literature relating to critical thinking skills within the health care sector which have indicated that the ability of students and graduates to think critically is below the desired level (Castle, 2006, Castle, 2009, Fero et al., 2010, Agwu et al., 2007 and Tufekci et al., 2011). A Nigerian radiography study (Agwu et al., 2007) suggests that radiographers tend to learn 'over the shoulder' by watching other radiographers, instead of being given the chance to think for themselves. Thus they follow a rehearsed routine and are unable to critically analyse in clinical situations (Walsh & Seldomridge, 2006). Therefore, in clinical practice, it is common for students to undertake an examination, without thinking about the reason for the examination (Nisbet & Matthews, 2011) which, in the current study, could explain the participants poor application of critical thinking skills.
Sim and Radloff (2009) have also criticized radiographers as being followers rather than thinkers and blame the protocol-driven practices that are followed in radiography as contributing to this problem. Similarly, participants in the current study tend to rehearse what to do, instead of being encouraged to think for themselves and apply their knowledge to the clinical situation. The students' limited ability to synthesize information may be explained by the traditional lecture methods of teaching (Gqweta, 2012, Kowalczyk and Leggett, 2005, Mann, 2012, Raymond and Profetto-McGrath, 2005 and Wessel and Williams, 2004) used by the department in the institution concerned, where students become passive absorbers of knowledge instead of active participants in questioning, thinking and applying their knowledge in order to draw conclusions, propose alternatives and develop a plan. Fero et al. (2010) identify a clear link between weak critical thinking skills and ability to synthesize clinical information, which seems to also apply to the participants in the current study. It could be postulated that participants in the current study were placed in busy imaging departments for their practical clinical experience, with limited structured supervision and opportunity to make their own decisions and justify their actions further contributing to their limited critical thinking ability.
The current study further identified a minimal ability of participants to problem solve (Pieterse et al., 2014). Fero et al. (2010) yielded similar results to the current study, revealing that 75% of student nurses did not meet overall expectations relating to a given simulation designed to test for problem solving ability. Most student errors were associated with problem recognition and reporting findings to the referring doctor. In the current study participants could identify the problem but were unable to propose justifiable solutions. This minimal ability to problem solve could be due to students not being given the opportunity to think for themselves (Fero et al., 2010 and Mauro, 2009). In busy imaging departments, students tend to step aside when complications arise, and allow the qualified radiographer to take the lead. Very often students might continue with another patient, instead of following through with the initial patient and assisting the qualified radiographer, thereby inhibiting the development of a problem solving ability.
6. Conclusion
The results of this study indicate that the majority of the participants were unable to demonstrate critical thinking skills at the expected level in their responses to a vignette. This is in line with literature related to critical thinking skills within the health care sector, indicating that radiography, occupational therapy and nursing students' ability to think critically is below the desired level (Agwu et al., 2007, Castle, 2006, Castle, 2009, Fero et al., 2010, McMullen and McMullen, 2009, Raymond and Profetto-McGrath, 2005, Tufekci et al., 2011 and Velde et al., 2006). Literature reveals that critical thinking skills can be taught to students. It is therefore imperative that teaching methods be incorporated into the academic environment in order to address the critical thinking skills of students, and thereby improve clinical efficiency.
6.1. Limitations
A limiting factor was that data was collected at a single university rather than in multiple universities offering the radiography programme. In addition, it is possible that inter-rater reliability may have been compromised by the use of a single assessor.
6.2. Recommendations
Guidelines should be developed which could be implemented into the radiography curriculum in order to facilitate the development of critical thinking skills in radiography students. According to the literature, teaching strategies such as role play, simulation, case studies, concept mapping and problem based learning (Chabeli, 2010, Kowalczyk and Leggett, 2005, Popil, 2011, Ravert, 2008 and Wong et al., 2008) could all be used to improve critical thinking of students. These teaching strategies should be incorporated into the curriculum, with tasks and teaching methods designed in such a way as to encourage, support and extract these critical thinking skills.
Further research needs to include the implementation of teaching strategies for the development of critical thinking and the impact of the teaching strategies on critical thinking ability of radiography students. The study should be widened to include several universities across the country.
Acknowledgements
The results presented in this article form part of a study completed by the primary author as part of a Master's Degree in Radiography. Financial support was granted by the staff qualifications project of the university concerned.
References
Agwu, K. K., Ogbu, Soi., & Okpara, E. (2007). Evaluation of critical thinking application in medical ultrasound practice among sonographers in south-eastern Nigeria. Radiography, 13, 276e282. [ Links ]
Anderson, L. W., & Krathwohl, D. R. (2001). A taxonomy for learning, teaching and assessing: A revision of bloom's taxonomy of educational objectives. Boston: Allyn and Bacon. [ Links ]
Babbie, E. (2010). The practice of social research (12th ed.). Belmont: USA. [ Links ]
Bloom, B. (1984). A taxonomy of educational objectives. Bloom, B., (1984) (2nd ed.). New York: Addison Wesley. [ Links ]
Castle, A. (2006). Assessment of the critical thinking skills of student radiographers. Radiography, 12, 88e95. [ Links ]
Castle, A. (2009). Defining and assessing critical thinking skills for student radiographers. Radiography, 15, 70e76. [ Links ]
Castle, A. (2011a). Generation of a project proposal for an undergraduate literature review: One dimension of critical thinking. International Journal of Therapy and Rehabilitation, 18(4), 190e197. [ Links ]
Castle, A. (2011b). Evaluation of a radiographic technique: One dimension of critical thinking. International Journal of Therapy and Rehabilitation, 18(6), 311e317. [ Links ]
Chabeli, M. (2010). Concept-mapping as a teaching method to facilitate critical thinking in nursing education: A review of the literature. HealthSA Gesondheid, 15(1), 1e7. [ Links ]
Chee Choy, S., & San Oo, P. (2012). Reflective thinking and teaching practices: A precursor for incorporating critical thinking into the classroom? International Journal of Instruction, 5(1), 167e181. [ Links ]
Creswell, J. (2003). Research design: Quantitative, qualitative and mixed methods approaches (2nd ed.). London: Sage. [ Links ]
Creswell, J. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). Los Angeles: Sage. [ Links ]
De Vos, A. A. (2011). Research at grass roots: For the social sciences and human services professions (4th ed.). Pretoria: Van Schaik. [ Links ]
Facione, P. A. (1990). Critical thinking: A statement of expert consensus for purposes of educational assessment and instruction. The Delphi report. Millbrae: California Academic Press. [ Links ]
Facione, P. A. (2011). Critical thinking: What it is and why it counts. Millbrae: Measured Reasons and The California Academic Press. Retrieved from insight assessments www.insightassessments.com [Accessed on 22 August 2011]. [ Links ]
Facione, N. C., & Facione, P. A. (1996). Externalizing the critical thinking in knowledge development and clinical judgment. Nursing Outlook, 44, 129e136. [ Links ]
Fero, L. J., O'Donnell, J. M., Zullo, T. G., Devito Dabbs, A., Kitutu, J., Samosky, J. T., et al. (2010). Critical thinking skills in nursing students: Comparison of simulation-based performance with metrics. Journal of Advanced Nursing, 66(10), 2182e2193. [ Links ]
Forehand, M. (2012). Bloom's taxonomy. Emerging perspectives on learning, teaching and technology. Retrieved from the university of Georgia online www.coe.uga.edu [Accessed on 21 August 2012]. [ Links ]
Freeman, R., & Lewis, R. (1998). Planning and implementing assessment. London: Kogan Page. [ Links ]
Gqweta, N. (2012). Poor academic performance: A perspective of final year diagnostic radiography students. Radiography, 18, 212e217. [ Links ]
Jones, R. A. (2012). Instructional strategies that encourage critical thinking. The Science Teacher, 79(3), 66e70. [ Links ]
Kowalczyk, N., & Leggett, T. D. (2005). Teaching critical-thinking skills through group-based learning. Radiologic Technology, 77(1), 24e29. [ Links ]
Krefting, L. (1991). Rigor in qualitative research: The assessment of trustworthiness. The American Journal of Occupational Therapy, 45(3), 154e169. [ Links ]
Mann, J. (2012). Critical thinking and clinical judgment skill development in baccalaureate nursing students. The Kansas Nurse, 87(1), 26e30. [ Links ]
Mauro, A. M. P. (2009). Jumping on the simulation bandwagon: Getting started. Teaching and Learning in Nursing, 4(2), 30e33. [ Links ]
Mc Inerney, J., & Baird, M. (2016). Developing critical practitioners: A review of teaching methods in the bacheor of radiography and medical imaging. Radiography, 22, e40ee53. [ Links ]
McMullen, M. A., & McMullen, W. F. (2009). Examining patterns of change in the critical thinking skills of graduate nursing students. Journal of Nursing Education, 48(6), 310e319. [ Links ]
Murphy, F. J., & Yielder, J. (2010). Establishing rigour in qualitative radiography research. Radiography, 16, 62e67. [ Links ]
Ng, C. K. C., White, P., & McKay, J. C. (2008). Establishing a method to support academic and professional competence throughout an undergraduate radiography programme. Radiography, 14(3), 255e264. [ Links ]
Nisbet, H., & Matthews, S. (2011). The educational theory underpinning a clinical workbook for VERT. Radiography, 17, 72e75. [ Links ]
Pallant, J. (2007). SPSS survival manual (3rd ed.). Glascow: Bell and Bain. [ Links ]
Peirce, W. (2006). Designing rubrics for assessing higher order thinking. Retrieved from designing rubrics for assessing higher order thinking, online http://academic.pgcc.edu/~wpeirce/MCCCTR/Designingrubricsassessingthinking.html [Accessed on 19 August 2009]. [ Links ]
Pieterse, T. D., Lawrence, H., & Friedrich-Nel, H. (2014). Problemsolving abilities of radiography students at a South-African University. African Journal of Health Professions Education (AJHPE), 6(1), 33e36. [ Links ]
Popil, I. (2011). Promotion of critical thinking by using case studies as teaching method. Nurse Education Today, 31, 204e207. [ Links ]
Ravert, P. (2008). Patient simulator sessions and critical thinking. Journal of Nursing Education, 47(12), 557e562. [ Links ]
Raymond, C. L., & Profetto-McGrath, J. (2005). Nurse educators' critical thinking: Reflection and measurement. Nurse Education in Practice, 5(4), 209e217. [ Links ]
Sim, J., & Radloff, A. (2009). Profession and professionalization in medical radiation science as an emergent profession. Radiography, 15, 203e208. [ Links ]
South African Qualifications Authority [s. [ Links ]a.] Retrieved from SAQA online http://regqs.saqa.org.za/viewQualification.php?id=66949) [Accessed on 8 August 2012].
Spencer, C. (2008). Critical thinking in nursing: Teaching to diverse groups. Teaching and Learning in Nursing, 3, 87e89. [ Links ]
Tufekci, F. G., Kucokoglu, S., Bolubas, N., & Tezel, A. (2011). Critical thinking dispositions of nursing students and influencing factors in Turkey. Journal of Society for Development in New Net Environment in B & H, 5(4), 831e836. [ Links ]
Ugwu, A. C., Ukwueze, A. C., Erondu, O. F., & Nwokorie, E. (2010). Affective and cognitive learning outcomes of radiography students in a Nigerian university. The South African Radiographer, 48(2), 13e16. [ Links ]
Vacek, J. E. (2009). Using a conceptual approach with concept mapping to promote critical thinking. Journal of Nursing Education, 48(1), 45e48. [ Links ]
Velde, B. P., Wittman, P. P., & Vos, P. (2006). Development of critical thinking in occupational therapy students. Occupational Therapy International, 13(1), 49e60. [ Links ]
Walsh, C. M., & Seldomridge, L. A. (2006). Critical thinking: Back to square two. Journal of Nursing Education, 45(6), 212e219. [ Links ]
Wessel, J., & Williams, R. (2004). Critical thinking and learning styles of students in a problem-based, master's entry-level physical therapy program. Physiotherapy Theory and Practice, 20, 79e89. [ Links ]
Wong, F. K., Cheung, S., Chung, L., Chan, K., Chan, A., To, T., et al. (2008). Framework for adopting a problem-based learning approach in a simulated clinical setting. Journal of Nursing Education, 47(11), 508e514. [ Links ]
Yildirum, B., Ozkahraman, S., Korkmaz, M., & Ersoy, S. (2011). Examination of critical thinking disposition in nursing. HealthMED, 5(6), 1549e1557. [ Links ]
Received 19 June 2015
Accepted 5 July 2016
Available online 14 September 2016
Peer review under responsibility of Johannesburg University.
E-mail addresses: traceyp@uj.ac.za (T. Pieterse), heatherl@uj.ac.za (H. Lawrence), hfried@cut.ac.za (H. Friedrich-Nel).
* Corresponding author.


{kind=link}