










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 no.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.07.004
FULL LENGTH ARTICLE
Maximum potential cost-savings attributable to generic substitution of antipsychotics 2008 to 2013
D. HusselmannI; R. JoubertII, *; J.R. BurgerI; M.S. LubbeI; M. CockeranI
IMedicine Usage in South Africa, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIPharmacy Practice, School of Pharmacy, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
ABSTRACT
BACKGROUND: Schizophrenia is a costly illness to treat, especially during a time of escalating medicine inflation costs, putting a large economic strain on patients, their families and the community. Treatment, however, can become more affordable through generic substitution.
OBJECTIVE: To determine the maximum potential cost-saving through generic substitution for both originator and more expensive generic items while observing the prescribing patterns of antipsychotics.
METHOD: Antipsychotic medicine usage was analysed retrospectively during the study period 2008 to 2013 using data obtained from a nationally representative Pharmaceutical Benefit Management Company. The study population consisted of 4410 patients with ICD-10 codes (F20-F20.9) who had paid claims for an antipsychotic reimbursed from their prescribed minimum benefits. Active ingredients were identified using the MIMS classification system. Maximum potential cost savings were determined by substituting all originator and more expensive generic antipsychotic items with the cost of the least expensive generic antipsychotic item available.
RESULTS: Through generic substitution, a total potential cost-saving of ZAR4 642 685.45 could be possible from 2008 to 2013. Average cost per items increased from ZAR600.53 ± ZAR435.00 (median ZAR 539.82) in 2008 to ZAR1 196.59 ± ZAR 942.16 (median ZAR 940.72) in 2013 and had a significant effect on patients' contribution, which increased with 726.94% from 2005 to 2008. Psychiatrists prescribed the majority of antipsychotics. Although generic items claimed increased by 60.31% during the study period, psychiatrists still favoured non-generic prescribing (40.63%).
CONCLUSIONS: Potential economic benefits can be generated with generic substitution.
Keywords: Generic substitution; Potential cost-saving; Originator; Generic; Non-generic; Antipsychotics; South Africa
1. Introduction
Neuropsychiatric conditions are ranked third in their contribution to the burden of disease in South Africa, after HIV/AIDS and other infectious diseases (Bradshaw, Norman, & Schneider, 2007;Lund et al., 2008). A study conducted by Williams et al. (2008) revealed that 16.5% of all South Africans suffer from common mental disorders, including, inter alia, depression, anxiety and somatoform disorders. This figure, however, did not include schizophrenia and bipolar mood disorder ( Williams et al., 2008). When costs of treatment for psychiatric illnesses are compared, schizophrenia is the most costly illness to treat (Emsley & Booysen, 2004). Without healthcare coverage, treatment for schizophrenia can become unaffordable, even if generic medicines are used (Lehman et al. 2004). A rapid increase was observed in the percentage of medical expenditures in association with prescription drugs (Fischer & Avorn, 2003). In 2011, $12.6 billion was spent on 54 million prescriptions issued for antipsychotics in the United States of America (Leonhauser, 2012). Irrespective of its economic strain on patients themselves, this disease also puts a large economic burden on families, societies and healthcare systems (Emsley & Booysen, 2004). For example, according to Emsley and Booysen (2004), it could cost a family of a schizophrenic patient approximately ZAR 498 771.00 per year to take care of such an individual, while spending approximately 15 h a week taking care of these members.
South Africa spends 8.9% of its gross domestic product (GDP) on health, which is relatively high compared to the 5% recommended by the World Health Organization (WHO) (World Health Organization, 2016 and South Africa. Department of Health, 2011). According to the South African National Treasury (2015), a total of ZAR 121 billion was spent on health for 2012/2013 (Department of Health, 2011). Regardless of this rather high expenditure, health outcomes compared to more or less the same middle-income countries, remain poor (Department of Health, 2011).
In order to control healthcare costs in the private sector of South Africa, a number of regulations, policies and pricing interventions were put in place by the South African Government, inter alia, the National Drug Policy (NDP), the Medicines and Related Substances Control Amendment Act (No 90 of 1997), Good Pharmacy Practice (GPP) and Good Marketing Practice (GMP) rules, a transparent pricing structure and certain pricing interventions such as mandatory generic substitution, the establishment of the Single Exit Price (SEP) for all medicine, and the Prescribed Minimum Benefits (PMBs) and Chronic Disease List. The goal of the National Drug Policy, published in 1996, was to "ensure an adequate and reliable supply of safe, cost-effective drugs of acceptable quality to all citizens of South Africa, and the rational use of drugs by prescribers, dispensers and consumers" (South Africa, 1996). The Medicines and Related Substances Control Amendment Act No 90 of 1997, tabled in Parliament in May 1997, was designed for the provision of more affordable medicines ( Deroukakis, 2007 and South Africa, 1997). In Section 22F of this act, which was implemented on 2 May 2003, generic substitution was promulgated and states that a pharmacist is required to dispense the generic alternative of a prescribed medicine, unless the patient or the prescribing doctor explicitly refuses the substitution, or if the price of the generic product is higher than that of the branded or originator product (Black, 2013; Deroukakis, 2007 and South Africa, 1997). The Medicines and Related Substances Act, Good Pharmacy Practice (GPP) and Good Marketing Practice (GMP) rules furthermore ensure that medicines are of good quality, that medicines are safe and effective, that marketing takes place according to a code of marketing and that medicine prices are transparent and in accordance with single exit price (SEP) regulations (Black, 2013). The Prescribed Minimum Benefit (PMB) conditions listed by Council of Medical Schemes (CMS) (CMS, 2009) is a set of well-defined benefits to make sure that all medical scheme members have access to certain minimum health services, regardless of the benefit option they have selected, in order to be provided with continuous care, to improve the health and well-being of a patient, to make healthcare more affordable and to prevent restriction of access to health insurance for high-risk individuals (CMS, 2010). Medical aid schemes are obligated to cover diagnosis, medical costs as well as cost of care of patients registered on the chronic disease list of the PMB, provided that the prescribed therapeutic algorithm is followed ( Council for Medical Schemes, 2009 and South Africa. Department of Health, 2003). Schizophrenia is listed as one of these 27 chronic disease disorders in South Africa.
The single exit price in South Africa is set according to benchmark prices of other international countries that follow pricing systems closest to the system that is used in South Africa. Department of Health (2015). New Zealand, Australia, Canada and Spain were chosen as benchmarking countries (Department of Health, 2015). The SEP may be applied to products that are priced below the international benchmark and may be increased up to the international benchmark, but the SEP may not exceed the price of the benchmark (Department of Health, 2015). The annual increase of SEP for 2008 was 6.5%; in 2009 SEP increased with 13.2%; and in 2010 SEP increased with 7.4% (Council for Medical Schemes, 2014). In 2011, there was no increase in SEP (South Africa, 2011). An annual adjustment was made in 2012 for the SEP of medicines and scheduled substances where the South African Minister of Health stated that SEP may only be applied to a maximum of 2.14% as last stated on 9 December 2011 (South Africa, 2012). In 2013, a maximum of 5.8% was applied as last stated in 23 December 2012 (South Africa, 2013). In 2013, medicine expenditure increased by 2% for cost per item from 2011 (Mediscor, 2013). A total of 42.2% of manufacturers that represent approximately 83.3% of products sold in South Africa took a 4% increase in SEP for January to May in 2013 (Mediscor, 2013). This increase in cost puts a large economic strain on patients during a time of spiralling medication inflation (Mediscor, 2013).
According to the WHO (2010), a generic drug is a pharmaceutical product or medicine item that is manufactured without a licence from the innovator company and marketed after the patent right of the specific drug has expired. These generic medicines should be of the same formula (including, inter alia, the same amount of active ingredient and the same route of administration) while giving the same therapeutic effectiveness than that of the originator medicine ( Borgherini, 2003). Originator products have a higher cost than their generic versions, which produce the same therapeutic effect (Fischer & Avorn, 2003). Costs of originator drugs, especially in low and middle-income countries, are substantially higher than their generic alternatives (WHO, 2010). Typically, generic substitutions are 20-90% cheaper than those of originator medicines (Dunne, Shannon, Dunne, & Cullen, 2013). In 2013, 20% of overall medicine product costs were for original items for which patents had already expired (Mediscor, 2013). This raised concern, as average generic equivalents for all medicine items were only ZAR96 per item, compared to the average cost of all original items with expired patents at ZAR131 (Mediscor, 2013).
In this study, we aimed to determine the maximum potential cost saving by substituting the average medicine cost of more expensive generic and originator antipsychotic items with that of the least expensive generic antipsychotic items available on the database during the study period, while observing the prescribing patterns of antipsychotics (including, inter alia, prescriber speciality). Generic substitution poses the advantage of reducing treatment expenditure for patients while maintaining the same quality of care ( Hamann, Mendel, Kissling, & Leucht, 2013).
2. Method
2.1. Data source and study population
Medicine usage of antipsychotics for the treatment of schizophrenia was analysed retrospectively using repeated cross-sectional analysis, for the study period 1 January 2008 to 31 December 2013. Data were obtained from a Pharmaceutical Benefit Management Company (PBM). A total of 8.78 million individuals in South Africa were registered as members of medical schemes in 2013 (Council for Medical Schemes, 2014), of whom 1.7 million individuals were members of this nationally representative PBM. All of South Africa's pharmacies and 98% of all dispensing doctors are on this service provider database.
Data fields used from the database included date of treatment, active ingredients, direct medicine cost (total cost, SEP, medical scheme contribution and patient contribution), trade names of active ingredients and quantities.
All patients with ICD-10 codes F20-F20.9 (classification for different types of schizophrenic diagnosis) with a claim reimbursed from their prescribed minimum benefit for active ingredients included in the MIMS classification system for schizophrenia (N = 4410) were included in the study (Snyman, 2014). Antipsychotics were categorised according to four pharmacological groups: phenothiazines, butyrophenones, atypical antipsychotics and others (Snyman, 2014).
2.2. Measurements
Schizophrenia prevalence was determined as percentage of the total patient population of the database. Total costs of antipsychotics were determined as a percentage of the total cost of medicine products of the database. Thereafter, the average cost per item per patient was compared, in terms of the medical scheme contribution and patient contribution as well as the influence of the single exit price on the average cost per item. Average costs per generic status (i.e. generic, non-generic or originator) were compared, while observing the medical scheme contribution and patient contributions. Prevalence of antipsychotics prescribed based on generic status and prescriber speciality was determined. The percentage change in the number of items and mean cost were calculated by dividing the difference between the 2013 and 2008 values by the 2008 value and then multiplying it with 100. For example: the percentage increase in mean cost = [(Mean cost 2013 − mean cost 2008)/mean cost 2008] × 100 = [(43.09 − 24.26)/24.26] × 100 = 77.62%.
The primary outcome of this study was to determine the maximum potential cost saving in direct medicine costs for patients per year by substituting all originator and more expensive generic antipsychotic medicine items with the mean cost of the least expensive generic antipsychotic medicine item during the year while observing the prescribing patterns of antipsychotics (including, inter alia, prescriber speciality). The differences in actual and substituted costs per year were then summed to calculate the total potential cost saving for the study period.
2.3. Statistical analysis
The SAS program version 9.3 (SAS Institute, Cary, NC, 2008-2013) was used for statistical analyses. Descriptive statistics included frequencies, means, standard deviations (SD), medians and interquartile ranges, and 95% confidence intervals (95% CI). Inferential statistics included analysis of variance (ANOVA) with Tukey's HSD post-hoc test, which was used to compare mean values between more than two independent groups. Cohen's d-value was used to determine effect sizes and was taken as practically significant if d ≥ 0.8. This was only considered if there was a practical significance p ≤ 0.001. Chi-square distribution models were used to test the distribution of the statistics of the population. Practical significance was then determined by Cramer's V and values ≥ 0.1 were regarded as a small effect, ≥0.3 as a moderate effect and ≥0.5 as large effects.
2.4. Ethical considerations
This study was approved by the board of directors of the PBM company, as well as the Health Research Ethics Committee of the North-West University (NWU-00179-14-A1).
3. Results
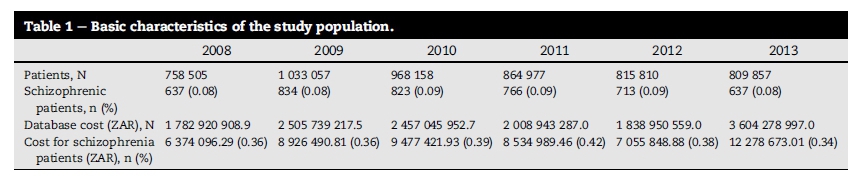
Table 1 describes the basic characteristics of the study population. During the study period (2008-2013), the prevalence of schizophrenia varied between 0.08% and 0.09% of the total population on the database. The total direct cost for the treatment of schizophrenia with antipsychotics ranged from ZAR 6 374 096.29 in 2008 to ZAR 12 278 673.01 in 2013.
The majority of antipsychotics were prescribed by psychiatrists (Table 2). Antipsychotic prescribing by general medical practitioners decreased by 5.43% during the study period, whereas that by neurologists and psychiatrists increased with 0.52% and 4.80%, respectively. For the purpose of this study, a non-generic item was defined as an originator product of which the patent has not yet expired and therefore no generic equivalent product was available. A general breakdown of the prescribing patterns of antipsychotics by generic status shows that the prescribing of non-generic items decreased by 35.21% overall, whereas that of originator and generic items increased with 8.08% and 27.12%, respectively, during the study period. Prescribing of generic antipsychotics by general medical practitioners, neurologists and psychiatrists increased by 30.58%, 41.52% and 25.23%, respectively, from 2008 to 2013 (Table 2). The prescribing of non-generic items by all prescribers decreased during the study period; however, psychiatrists still slightly favoured prescribing of non-generic items during 2013 (40.63%). The majority of prescriptions by general medical practitioners, neurologists and all other prescribers were for non-generic items.
The cost per antipsychotic medicine item consists of a drug's SEP, scheme contribution and patient contribution. These, as well as a breakdown of mean costs stratified by generic status are presented in Table 3. The mean cost per item increased by 99.26% from ZAR 600.53 ± ZAR 435.00 (95% CI 566.68-634.38) in 2008 to ZAR 1196.59 ± ZAR 942.16 (95% CI 1123.29-1269.90) in 2013 (p < 0.001; Cohen's d-value = 1.01) ( Table 3). The mean SEP per item increased with 77.62% from ZAR24.26 ± ZAR 67.84 (95% CI 18.98-29.53) in 2008 to ZAR 43.09 ± ZAR165.44 (95% CI 555.89 ± 555.89) in 2013. Although the mean cost covered by medical schemes stayed more or less the same, a practically significant increase of 726.94% occurred in the co-payment of patients from ZAR 77.48 ± ZAR 123.76 (95% CI 67.86-87.11) in 2008 to ZAR 640.71 ± ZAR 518.19 (95% CI 600.39-681.02) in 2013 (p < 0.001; Cohen's d-value = 2.28).
Stratification of the mean cost per antipsychotic medicine item by generic status showed that the mean cost of generics increased with 219.52% from 2008 to 2013 (Cohen's d-value = 1.02), whereas that of originator and non-generic items increased by 136.69% (Cohen's d-value = 0.77) and 106.45% (Cohen's d-value = 0.56), respectively ( Table 3). Mean patient co-payments for non-generic and generic drugs increased by 784.17% and 798.78%, respectively, over the study period (Cohen's d-value > 0.8), whereas that of originator drugs increased by 444.93% (Cohen's d-value = 1.1). The SEP increased with 163.35% for non-generic items (Cohen's d-value = 0.18) and 105.66% for generic items (Cohen's d-value = 0.89). Scheme contributions for non-generics remained relatively the same (Cohen's d-value = 0.08), while increasing by 36.51% for originators (Cohen's d-value = 0.35) and 91.84% for generics (Cohen's d-value = 0.70).
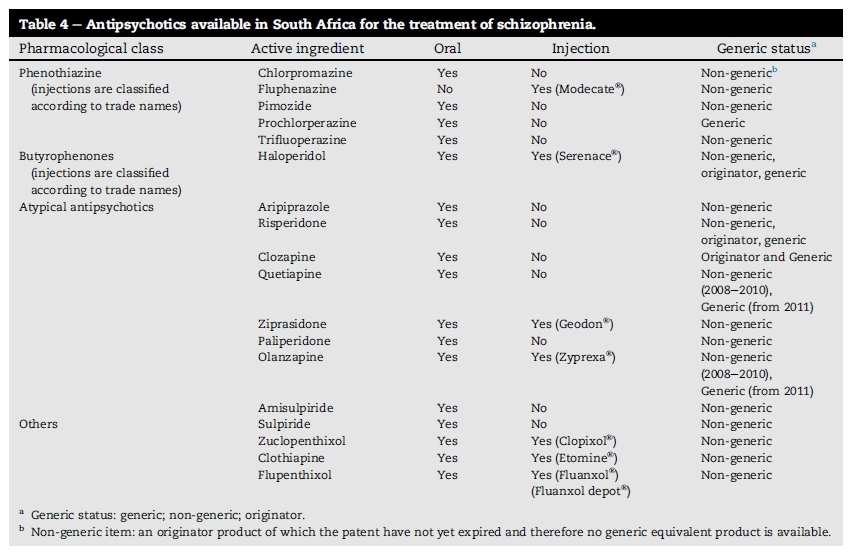
Availability of generic alternatives increased within the study period; however, from the 18 antipsychotics currently available in the South African market (listed in Table 4), only five had generic alternatives on the database during the study period. These included; clozapine, haloperidol, olanzapine, quetiapine and risperidone. The total costs for originator and generic items in 2008 accrued to ZAR 281 946.66 (Table 5). If all originator and more expensive generic items were substituted with the mean cost of the least expensive generic item available, a potential cost saving of ZAR 106 855.59 (37.90%) could have been generated during 2008. Similarly, potential annual cost-savings of 25.72%, 33.64%, 47.80%, 41.47% and 39.29%, respectively, would have been possible from 2009 to 2013. A total of ZAR 4 642 685.00 could potentially have been saved over the six-year study period if all originator and more expensive antipsychotic generic items were substituted with the least expensive generic antipsychotic item available on the database for each year.
4. Discussion
Treatment for schizophrenia is extremely costly (Emsley & Booysen, 2004), and therefore patients' health expenditures can be reduced by developing a cost-saving plan through generic substitution (Hamann et al., 2013). By using generic medication, at a lower cost and assured quality of their originator equivalent, health outcomes for both patients and health systems can be achieved at a lower cost.
For our study, atypical antipsychotics had more generic equivalents (clozapine, olanzapine, quetiapine, risperidone) as opposed to typical antipsychotics (haloperidol), supporting studies from the literature that atypical antipsychotics are leading the market (Leonhauser, 2012). However, no generic equivalents were available for the phenothiazines and 'others' (e.g. sulpiride, zuclopenthixol decanoate, flupenthixol and clothiapine) group on the dataset during the study period. The low number of generic alternatives for quetiapine and olanzapine could be due to patent protection during our study period. These expired in 2011 for olanzapine (Zyprexa®) and in 2012 for quetiapine (Seroquel®) (De Ruiter & Holston, 2012).
Based on the Mediscor annual report of 2013/2014, 20% of medicine items in total claimed during 2013 were originator products (Mediscor, 2013). Medical aid schemes make use of reference drugs for each therapeutic class to determine the maximum price that may be reimbursed (McLeod & Ramjee, 2006). If the cost of the drug dispensed is higher than the price of the reference drug, then the patient has to pay the difference in price (McLeod & Ramjee, 2006). Antipsychotics claimed during 2013 were the most expensive, even with generic substitutions (Table 4). The national single exit price increased initially with 6.5% annually from 2008, then 13.2% (2009), 7.4% (2010), 0% (2011), 2.14% (2012) and 5.8% (2013), respectively, affecting the dispensing fee that directly influenced the median cost per item (Council for Medical Schemes, 2014, South Africa, 2011, South Africa, 2012, South Africa, 2013 and Mediscor, 2013). A 5.8% increase in the SEP was allowed in 2013, causing an overall 2% increase in the median cost per items, explaining the large increase in total costs for 2013 (Mediscor, 2013).
Patient contribution for all antipsychotics (generics, non-generics and originators alike) increased significantly from 2008 to 2013 compared to both the average household inflation in South Africa, as well as the increase in earning power of the households (Statistics South Africa, 2016). This could be due to changes in medical scheme benefit packages and formularies, medical inflation, possible use of non-designated service providers, as well as additional costs charged by the provider that were in disagreement with the medical scheme rate or dispensing fee for the year (Mediscor, 2013). Research has, however, shown that co-payments have an immediate and persistent deterrent effect on the use of psychotherapeutic drugs, increasing the likelihood that patients will choose not to pay and to stop taking prescribed drugs (Reeder and Nelson, 1985 and Treur et al., 2009), resulting in increases in patient visits to community mental health centres, use of emergency mental health services and partial hospitalisation (Hynd et al., 2008 and Soumerai et al., 1994).
According to Fischer and Avorn (2003), a potential annual cost-saving of a quarter to half a billion dollars is possible when all originator prescription drugs are substituted with generic brands. This observation was confirmed in our study where it was found that approximately ZAR 4.6 million could have been saved over the six-year period if antipsychotic drugs for the treatment of schizophrenia were generically substituted. Psychiatrists, however, are not always willing to consider that medication may be substituted with their generic equivalents (Hamann et al., 2013). Reasons stated against generic substitution includes that physicians have been found to believe that originator medicine items are more effective and have a higher standard of manufacturing than their generic versions (Fischer and Avorn, 2003 and Shrank et al., 2011), vague attitudes towards properties of generics and branded drugs as well as by 'non-evidence based' factors such as uncertainty in tolerance (Hamann et al., 2013). Furthermore, patients themselves are not always willing to use generic equivalents. For example, Roman (2009) found that 73% of patients treated with oral antipsychotics would refuse generic substitution when given the option by a pharmacist. Schizophrenic patients, in particular, are often reluctant to change and may become suspicious, paranoid, delusional or even hostile when changing their medicine to a generic version (Treur et al., 2009). Reasons stated against the use of generics in general include that generic items appear differently (different colours, odd shapes etc.) than the originator items, confusing patients, especially the elderly (Dunne et al., 2013) Therefore, it is encouraged that generic products have the same appearance than their originators (Posner & Griffin, 2011).
5. Conclusion
This study confirmed the potential economic benefits of using generics. It can be concluded that if only 45% of medicine items were dispensed using generic substitution, which, according to Mediscor, is the actual rate for generic substitution in South Africa, then a total of ZAR 2 089 208.20 could still have been saved during the study period. Due to patent protection on drugs, there is the probability that the number of generic alternatives will increase for antipsychotics in the future. However, with the rather large increase in patient contribution towards antipsychotics, it is clear that even generic drugs may soon be unaffordable for patients, which can also affect patients' adherence. It is therefore necessary that alternative and innovative cost-saving methods be investigated.
6. Limitations
When patients used varying providers, all the necessary claims were not captured (e.g. 'out-of-pocket' payments, hospitalisation etc.) as these claims data were lost to the database and therefore not available for analyses. External validity was also limited as only one database was used for analyses and was therefore not representative of the South African market as a whole.
Funding
The National Research Foundation (NRF) contributed to the funding of the first author. The NRF, however, had no involvement in the writing, study design, collection, and interpretation of the data and in the decision of submitting the article for publication.
Acknowledgements
We would like to thank Cecile van Zyl for proofreading this article as well as Anne-Marie Bekker for assisting in the data analyses. A special thanks also to the Pharmaceutical Benefit Management Company for providing their data in order to conduct this study.
References
Black, G. (2013). Generic substitution and the Consumer Protection Act: a pharmacist's perspective. South African Pharmaceutical Journal, 80(8), 35e38. [ Links ]
Borgherini, G. (2003). The bioequivalence and therapeutic efficacy of generic versus brand-name psychoactive drugs. Clinical Therapeutics, 25(6), 1578e1592. http://dx.doi.org/10.1016/S0149-2918(03)80157-1. [ Links ]
Bradshaw, D., Norman, R., & Schneider, M. (2007). A clarion call for action based on refined DALY estimates for South Africa. South African Medical Journal, 97(6), 438e439. [ Links ]
Council for Medical Schemes. (2009). PBM review consultation document: Third draft. Retrieved from http://www.medicalschemes.com/files/PMB%20Review/3rd_Draft_PMB_ 20090325.pdf. [ Links ]
Council for Medical Schemes. (2010). Definition what are PMBs?. Retrieved from https://www.medicalschemes.com/medical_schemes_pmb/. [ Links ]
Council for Medical Schemes. (2014). Annual report 2013/2014. Pretoria, SA: Author. [ Links ]
De Ruiter, J., & Holston, P. L. (2012). Drug patent expirations and the "patent cliff". U.S Pharmacist, 37(6), 12e20. [ Links ]
Deroukakis, M. (2007). Mandatory substitution successful. South African Medical Journal, 97(1), 63e64. [ Links ]
Dunne, S., Shannon, B., Dunne, C., & Cullen, W. (2013). A review of the differences and similarities between generic drugs and their originator counterparts, including economic benefits associated with usage of generic medicines, using Ireland as a case study. Biomedical Central Pharmacology and Toxicology, 14(1), 1e19. http://dx.doi.org/10.1186/2050-6511-14-1. [ Links ]
Emsley, R., & Booysen, F. (2004). Cost-effectiveness of an atypical conventional antipsychotic in South Africa: An economic evaluation of quetiapine versus haloperidol in the treatment of patients partially responsive to previous antipsychotics. South African Journal of Psychiatry, 10(3), 58e66. [ Links ]
Fischer, M. A., & Avorn, J. (2003). Economic consequences of underuse of generic drugs: Evidence from Medicaid and implications for prescription drug benefit plans. Health Services Research, 38(4), 1051e1063. http://dx.doi.org/10.1111/1475-6773.00162. [ Links ]
Hamann, J., Mendel, R., Kissling, W., & Leucht, S. (2013). Psychiatrists' decision making between branded and generic drugs. European Neuropsychopharmacology, 23(7), 686e690. http://dx.doi.org/10.1016/j.euroneuro.2012.08.007. [ Links ]
Hynd, A., Roughead, E. E., Preen, D. B., Glover, J., Bulsara, M., & Semmens, J. (2008). The impact of co-payment increases on dispensings of government-subsidised medicines in Australia. Pharmacoepidemiology and Drug Safety, 17(1), 1091e1099. http://dx.doi.org/10.1002/pds.1670. [ Links ]
Lehman, A. F., Lieberman, J. A., Dixon, L. B., McGlashan, T. H., Miller, A. L., Perkins, D. O., et al. (2004). Practice guideline for the treatment of patients with schizophrenia, second edition. American Journal of Psychiatry, 161(2 Suppl.), 1e56. i-iv. [ Links ]
Leonhauser, M. (2012). Antipsychotics: Multiple indications help drive growth. Retrieved from https://www.imshealth.com/ims/Global/Content/Corporate/Press%20Room/ IMS%20in%20the% 20News/Documents/PM360_IMS_Antipsychotics_0112.pdf. [ Links ]
Lund, C., Kleintjes, S., Campbell-Hall, V., Mjadu, S., Petersen, I., Bhana,A., et al. (2008).Mental health&poverty project.Mental health policy development and implementation in South Africa: A situation analysis. Phase 1. Country report. Retrieved from http://www.who. int/mental_health/policy/development/SA%20Country% 20Report%20-%20Final%20Draft%20Jan%202008.pdf. [ Links ]
McLeod, H., & Ramjee, S. (2006). Medical schemes. Retrieved from http://www.hst.org.za/uploads/files/chap4_07.pdf. [ Links ]
Mediscor. (2013). Mediscor medicines review 2013. Retrieved from http://www.mediscor.net/MMR/Mediscor%20Medicines%20Review%202013.pdf. [ Links ]
National Treasury Republic of South Africa. (2015). Budget review 2015. Retrieved from http://www.treasury.gov.za/documents/national%20budget/2015/review/FullReview.pdf. [ Links ]
Posner, J., & Griffin, J. P. (2011). Generic substitution. British Journal of Clinical Pharmacology, 72(5), 731e732. http://dx.doi.org/10.1111/j.1365-2125.2011.03920.x. [ Links ]
Reeder, C. E., & Nelson, A. A. (1985). The differential impact of copayment on drug use in a Medicaid population. Inquiry, 22(4), 396e403. [ Links ]
Roman, B. (2009). Patients' attitudes towards generic substitution of oral atypical antipsychotics: A questionnaire-based survey in a hypothetical pharmacy setting. CNS Drugs, 23(8), 693e701. http://dx.doi.org/10.2165/00023210-200923080-00006. [ Links ]
Shrank, W. H., Liberman, J. N., Fischer, M. A., Girdish, C., Brennan, T. A., & Choudhry, N. K. (2011). Physician perceptions about generic drugs. Annals of Pharmacotherapy, 45(1), 31e38. http://dx.doi.org/10.1345/aph.1P389. [ Links ]
Snyman, J. R. (Ed.). (2014). MIMS monthly index of medical specialities (p. 525). Pretoria: MIMS. [ Links ]
Soumerai, S. B., McLaughlin, T. J., Ross-Deghan, D., Casteris, C. S., & Bollini, P. (1994). Effects of limiting Medicaid drugreimbursement benefits on the use of psychotropic agents and acute mental health services by patients with schizophrenia. The New England Journal of Medicine, 33(10), 650e655. [ Links ]
South Africa. (1997). Medicines and related substances act control amendment act (Act 90 of 1997) (1997, Dec 12). Government gazette, 18505. Retrieved from http://www.gov.za/sites/www.gov.za/files/a90-97.pdf. [ Links ]
South Africa. Department of Health. (1996). National drug policy. Retrieved from http://www.gov.za/sites/www.gov.za/files/drugpol_0.pdf. [ Links ]
South Africa. Department of Health. (2003). Medical Schemes Act, 1998 (Act No. 131 of 1998). Regulations made in terms of the Medical Schemes Act, 1998-amendment. Therapeutic algorithms for chronic conditions. Government Gazette, 25537(3), 6 Oct. Retrieved from http://www.gov.za/sites/www.gov.za/files/25537b_0.pdf. [ Links ]
South Africa. Department of Health. (2011). National health insurance in South Africa. Retrieved from http://www.hst.org.za/sites/default/files/2bcce61d2d1b8d972af41ab0e2c8a4ab.pdf. [ Links ]
South Africa. Department of Health. (2015). Announcement of the new dispensing fee for medicine. Retrieved from http://www.hst.org.za/news/announcement-new-dispensing-fee-medicine. [ Links ]
South Africa. Medicines and related substances act (Act 101 of 1965). (2013, Jan 22). Regulations relating to a transparent pricing system for medicines and scheduled substances: Amendment (single exit price adjustment for the year 2013) (Notice no. R35) Government Gazette, 36087. [ Links ]
South Africa. Medicines and related substances act (Act 101 of 1965). (2011, Jan 19). Regulations relating to a transparent pricing system for medicines and scheduled substances: Amendment (single exit price adjustment for the year 2011) (Notice no. R30) Government Gazette, 33961. [ Links ]
South Africa. Medicines and related substances act (Act 101 of 1965). (2012, Jan 19). Regulations relating to a transparent pricing system for medicines and scheduled substances: Amendment (single exit price adjustment for the year 2012) (Notice no. R47) Government Gazette, 34959. [ Links ]
Statistics South Africa. (2016). CPI history. Retrieved from http:// www.statssa.gov.za/. [ Links ]
Treur, M., Heeg, B., Möller, H., Schmeding, A., & Van Hout, B. (2009). A pharmaco-economic analysis of patients with schizophrenia switching to generic risperidone involving a possible compliance loss. Biomedical Central Health Services Research, 9(32), 1e9. http://dx.doi.org/10.1186/1472-6963-9-32. [ Links ]
Williams, D. R., Herman, A., Stein, D. J., Heeringa, S. G., Jackson, P. B., Moomal, H., et al. (2008). Twelve-month mental disorders in South Africa: Prevalence, service use and demographic correlates in the population-based South African stress and health survey. Psychological Medicine, 38, 211e220. http://dx.doi.org/10.1017/S0033291707001420. [ Links ]
World Health Organization. (2010). Cost savings of switching private sector consumption from originator brand medicines to generic equivalents. Health systems financing: the path to universal coverage. World Health Report (2010) background paper, no 35. Retrieved from http://www.who.int/healthsystems/topics/financing/healthreport/35Medicine CostSavings.pdf. [ Links ]
World Health Organization. (2016). Countries. Retrieved from http://www.who.int/countries/zaf/en/. [ Links ]
Received 6 October 2015
Accepted 6 July 2016
Available online 13 September 2016
Abbreviations: GDP, gross domestic products; PMB, Prescribed Minimum Benefits; NDP, National Drug Policy; WHO, World Health Organization; MIMS, monthly index of medicines speciality; SEP, single exit price; NRF, National Research Foundation
Peer review under responsibility of Johannesburg University.
* Corresponding author. E-mail address: rianda.joubert@nwu.ac.za (R. Joubert).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}