










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 n.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2016.01.004
FULL LENGTH ARTICLE
Short-term effects of simultaneous cardiovascular workout and personal music device use on the outer hair cell function of young adults
Bart Vinck1; Jessica Freeman*; Maggi Soer1
Department of Speech Language Pathology and Audiology, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Recreational noise exposure, including personal music device use (PMD), has become a growing public health concern, as it may potentially result in the development of hearing difficulties.
OBJECTIVES: The aim of the study was to determine the differential impact and short-term effects of simultaneous cardiovascular workout and PMD use on the outer hair cell (OHC) function of young adults.
METHOD: A quantitative research approach was followed. In this study a pre-test post-test approach was used and twelve subjects participated in three 1 h testing conditions with altered variables including: (i) exposure to PMD use in isolation, (ii) exposure to cardiovascular workout in isolation, and (iii) simultaneous exposure to the latter mentioned. Distortion product otoacoustic emissions (DPOAEs) were conducted pre- and post-exposure for each testing condition as primary indicator of cochlear responses. The process consisted of a cycling procedure through the preset stimulus frequency sequence, measuring the 2f₁-f₂ (75-70 dBSPL) and constructing a plot of DPOAE levels as a function of frequency.
RESULTS: Individual testing conditions did not result in statistically significant changes of the DPOAE response, however a significantly different profile in the DPOAE response level increase/decrease for the higher frequencies (6-8 kHz) was obtained when comparing the different sessions. Exposure to cardiovascular workout condition in isolation indicated a clear trend of an increased DPOAE response level between the pre-exposure and post-exposure testing from 2 kHz to 8 kHz with a maximum increase at 6 kHz. Both the music-only condition and the combined condition resulted in a clear trend of decreased DPOAE response amplitudes between the pre-exposure and post-exposure testing for the higher frequencies.
CONCLUSION: Findings support the notion of a clear effect of cardiovascular workout with and without music exposure on the OHC function at higher test frequencies, as measured by DPOAEs. Decreased DPOAE amplitudes between 2 kHz and 8 kHz were observed with music exposure and the opposite effect was observed for cardiovascular workout in isolation.
Keywords: Personal music device; Cardiovascular workout; Outer hair cell function; Otoacoustic emissions
ABSTRAK
AGTERGROND: Blootstelling aan geraas tydens ontspanningsaktiwiteite, soos die gebruik van persoonlike musiektoestelle (PMT), veroorsaak toenemende kommer met betrekking tot moontlike ontwikkeling van gehoorverlies.
DOELWITTE: Die doel van die navorsing was om die differensiële impak en korttermyn gevolge van gelyktydige kardiovaskulêre oefening en PMT gebruik op die buitenste haarselfunksionering van jong volwassenes te bepaal.
METODE: Tydens die studie is 'n kwantitatiewe pre-toets post-toets navorsingsbenadering gebruik waartydens twaalf deelnemers blootgestel is aan drie afsonderlike toetsomstandighede van een uur elk: (i) PMT gebruik in isolasie, (ii) kardiovaskulêre oefening in isolasie, en (iii) gelyktydige kardiovaskulêre oefening en PMT gebruik. Distorsieproduk oto-akoestiese emissies (DPOAE) is uitgevoer voor- en na blootstelling aan bogenoemde omstandighede as die primêre aanduiding van kogleêre response wat ontlok word deur 'n vasgestelde stimulus frekwensie patroon wat 2f₁ - f₂ (75-70 dBSPL) meet en voorstel as'n grafiek van DPOAE as 'n funksie van frekwensie.
RESULTATE: Die individuele toetsomstandighede het in isolasie geen statisties beduidende verskille in DPOAE amplitudes getoon nie. Statisties beduidende verskille in DPOAE amplitudes van die hoë frekwensies (6-8 kHz) is verkry tydens die vergelyking tussen die verskillende toetsomstandighede. Blootstelling aan kardiovaskulêre oefening alleenlik het 'n duidelike tendens van verhoogde DPOAE amplitudes tussen voor - en na blootstelling tussen 2 kHz en 8 kHz, met 'n maksimum by 6 kHz, getoon. Beide die musiek in isolasie en gekombineerde omstandighede het 'n duidelike afname in DPOAE amplitudes tussen voor - en na blootstelling getoon.
GEVOLGTREKKING: Hierdie bevindinge ondersteun die teorie dat kardiovaskulêre oefening 'n invloed op buitenste haarselfunksionering van hoë frekwensies kan hê, soos gemeet deur DPOAEs in die teenwoordigheid en afwesigheid van musiek. Verlaagde DPOAE amplitudes tussen 2 kHz en 8 kHz is geobserveer tydens musiektoestel blootstelling en die teenoorgestelde effek is waargeneem vir kardiovaskulêre oefening in isolasie.
1. Introduction
Over the past decade research has emphasized the growing risk of cochlear damage due to recreational noise exposure among young adults (Danhauer et al., 2009). Noise emitting devices such as personal music devices (PMDs) are now more compact and readily available (Danhauer et al., 2009, Haines et al., 2012, Hoover and Krishnamurti, 2010, Hodgetts et al., 2009, Punch et al., 2011, Sulaiman et al., 2014 and Shah et al., 2009). PMDs are manufactured to produce output levels up to 110 dBA (Bhagat and Davis, 2008, Keppler et al., 2010a and Kumar et al., 2009). Due to the availability, capacity and output levels of these devices research was conducted to assess possible effects on OHC functioning and hearing abilities. Keppler, Dhooge et al. (2010) concluded that temporary changes in outer hair cell (OHC) function, measured by otoacoustic emissions (OAEs) after 1 h listening time, indicated potential damaging effects of listening to a PMD. Kumar et al. (2009) reported a negative correlation between distortion product otoacoustic emission (DPOAE) measurements and music levels indicating that DPOAE amplitudes and signal to noise ratios (SNRs) were less significant in subjects who listened to high output music levels. Lastly, Bhagat and Davis (2008) found reduced DPOAE levels following high intensity music levels at 1.4 kHz-6.0 kHz. After a 30 min exposure time period the results indicated that reduced DPOAE levels may precede the progress of music-induced hearing threshold shifts.
Current legislation regarding noise exposure focuses mainly on occupational noise hazards. The allowable listening level is 85 dBA for an 8 h exposure time (National Institute for Occupational Safety and Health (NIOSH, 1998)). These recommendations state that as the sound level increases with 3 dBA, the listening time should be halved. The increase in the duration of listening time alone poses a great threat of OHC damage which can be measured accurately with OAEs (Attias et al., 2001 and Singh et al., 2009). Recent European standards for PMDs and mobile phones stipulate, however, that all PMDs sold after February 2013 should have a default set volume of 85 dB (http://www.hear-it.org/New-EU-standards-for-personal-music-players-and-mobile-phones).
Although PMDs can be used in several different listening environments, they are often used whilst doing cardiovascular workout. Cardiovascular workout increases blood flow and circulation to organs of the cochlea as well as oxygen saturation levels. Oxygen saturation refers to the amount of oxygen that is transported via the haemoglobin of red blood cells through the bloodstream as a percentage of the maximum it is able to transport (http://www.pulseox.info/pulseox/what2.htm).
There are also distinct physiological changes that take place in the inner ear after exposure to high intensity sound. Temporary threshold shift (TTS) includes a synaptic fatigue effect that is caused by the changes in metabolic processes of the OHCs and inner hair cells (IHCs) as well as changes in cochlear blood flow (Keppler et al., 2010b and Zhao et al., 2010). The repeated metabolic changes that occur during music exposure may lead to the generation of toxic metabolic byproducts such as reactive oxygen species (ROS) and free-oxygen radicals (FOR), which serve as triggers for cell damage and eventual necrosis and apoptosis (Zhao et al., 2010).
Cardiovascular fitness may positively influence hearing sensitivity through the effect of blood circulation to the organs and structures of the inner ear, especially the stria vascularis in the cochlea. Hutchinson, Alessio, and Baiduc (2010) mention existing evidence regarding hearing preservation and protection by cardiovascular workout. The latter study indicated that cells under stress from noise generate proteins to protect surviving cells. According to Hutchinson et al. (2010) metabolism and blood flow are directly related to the vascular structure of the cochlea. Variations in cochlear blood flow may consequently affect the availability of oxygen and glucose which is more rapidly metabolized during sound stimulation (Alessio, Hutchinson, Price, Reinhart, & Sautman, 2002). Vittitow, Windmill, Yates, and Cunningham (1994) concluded that a greater TTS is observed during simultaneous cardiovascular workout and noise exposure in comparison to these testing conditions in isolation. Krishnamurti, Sridhar, Grandjean and Peter (2003) found no evidence of auditory changes after short-term exposure to exercise and loud music. Although conflicting information exists on the effect of simultaneous cardiovascular workout and PMD use, the simultaneous metabolic changes including increased blood flow and oxygen saturation could decrease the risk for permanent music induced hearing loss (MIHL) (Hull & Kerschen, 2010).
Despite the lack of evidence on the simultaneous use of PMDs and cardiovascular workout, observable metabolic changes occur during both cardiovascular workout and PMD use in isolation, and it is feasible that these effects are magnified when combining the two activities (Hutchinson et al., 2010).
The main aim of this study was thus to determine whether there is a differential impact and potential short-term effects on OHC function in the presence of simultaneous cardiovascular workout and listening to music as measured by DPOAEs.
2. Method
2.1. Research design
A quantitative research approach was followed. In this study a pre-test post-test approach was used and subjects participated in three testing conditions with altered variables including (i) 1 h PMD use in a resting state, (ii) 1 h cardiovascular workout on a Cateye ergociser EC-3200 with inserted ear plugs to rule out potential external noise, and (iii) 1 h simultaneous PMD use and cardiovascular workout on a Cateye ergociser EC-3200. The testing conditions were completed on three separate days, each following a 72 h non-exposure time period. Each subject listened to identical pop-rock music samples on identical iPod Shuffle PMDs during the first and final testing conditions. Audiological testing was conducted in a quiet office. The pre-exposure session included an otoscopic examination, tympanometry and DPOAE testing (see Fig. 1). The exposure phase then commenced, directly followed by DPOAE testing.
2.2. Subject description
Twelve subjects (7 female, 5 male) were selected through convenience sampling and included in the study. All subjects presented with normal pure-tone averages (PTAs) (PTA ≤ 15 dB HL) (Vinck, De Vel, Xu, & Van Cauwenberge, 1996) as well as normal middle ear functioning. Middle ear pathology was ruled out by immittance testing, which included tympanometry (pressure: −50- 50 daPa, compliance: 0.3-1.75 ml, volume: 1-1.4 ml) and ipsilateral acoustic reflex testing (acoustic reflex present at 1000 Hz from 70 to 90 dB HL above the accepted normal pure tone threshold) (Martin and Clark, 2006 and Vinck et al., 1996). No previous or current ototoxic exposure, family history of hereditary hearing impairment or noise exposure 72 h prior to testing was recorded. Absent DPOAEs [signal to noise ratio (SNR) < 6 dB] and transient evoked otoacoustic emissions (TEOAEs) (SNR < 3 dB) excluded participation in the study. Subjects' ages ranged between 18 and 25 years with a mean age of 23 years [standard deviation (SD) = 0.95]. The mean female age was 22.71 years (SD = 0.95) and the mean male age was calculated at 23.4 years (SD = 0.89).
2.3. Equipment
An otoscopic examination was conducted with a Heine Mini 3000 otoscope in order to rule out structural abnormalities within the external meatus. Pure tone audiometric testing was performed in a standard audiometric soundproof booth by means of a recently calibrated GSI 61 audiometer to determine the pure-tone hearing thresholds. DPOAEs [signal to noise ratio (SNR) > 6 dB] and TEOAEs (SNR > 3 dB) were obtained by means of the ILO92 Otodynamics Analyser (calibrated on each day of testing). Immittance testing was conducted with a GSI Tympstar tympanometer. Finally a Cateye ergociser EC-3200 exercise bicycle was used during two of the three testing conditions in order to obtain data.
2.4. Ethical considerations
Prior to commencement of research ethical clearance was obtained as required by the ethical committee of the University of Pretoria Humanities Department. Subjects signed informed consent letters providing detailed information regarding testing procedures. A pilot study rendered testing procedures to be accurately repeatable to ensure that results are valid and reliable. Subjects were instructed to adjust the PMD to the loudest comfortable listening level instead of using a uniform loudness level. The latter is due to ethical considerations regarding the known fact that PMDs are able to produce intensities above the recommended allowable listening levels. In order to avoid harm to subjects this aspect of the study was variable in nature. Other variables possibly affecting the reliability of the testing procedures is the cardiovascular workout. Although all subjects engaged in cardiovascular workout for the exact same time period, possible differing fitness levels were not taken into consideration. Equipment used to assess possible short-term effects of testing conditions were deemed valid as DPOAEs directly assessed the OHC functioning. The equipment was calibrated on each day of testing. The equipment functions according to predetermined algorithms ensuring accuracy and repeatability of the tests. Therefore results can be deemed valid and reliable.
3. Procedures
3.1. Pre-exposure experimental testing
3.1.1. Outer and middle ear examination
The external ear canal was examined to rule out structural or foreign abnormalities. The subjects' middle ear functioning was evaluated through immittance measurements. A baseline tympanogram with a probe tone of 220 Hz and ipsilateral reflexes at 1000 Hz was performed prior to each of three testing conditions. Tympanometry testing and response parameters were calculated and interpreted as follows: tympanometric peak pressure (TPP) expressed in daPa, compliance, and the estimated ear canal volume.
3.1.2. Pre- and post-exposure experimental testing measured by DPOAEs
DPOAEs were performed prior to and following each exposure. The noise levels in the environment were minimized. Two simultaneous pure tones at the primary frequencies of f₁ and f₂ were generated by the ILO92 Otodynamics Analyser. The two stimuli were varied acoustically and delivered to a probe that was sealed with a foam tip into the external ear canal. The adequate positioning of the measurement probe in the external ear canal was monitored by using the 250 Hz tone 'checkfit' procedure prior to each session after which the test ear was presented with a click stimulus and the real time in-the-ear sound spectrum was shown on the screen (Vinck et al., 1996).
In order to rule out artifacts, the probe was manipulated to obtain a spectrum as uniform as possible with a realistic ear canal volume for each subject. The DP-grams were recorded using eight points/octave delivered from 75 to 70 dB SPL. The test frequencies that were used were automatically selected by the ILO92 software, based upon the resolution (point/octave) that was pre-selected by the user. The DP-gram collection process consisted of a cycling procedure through the preset stimulus frequency sequence, measuring the 2f₁-f₂ (75-70 dB SPL) DPOAE and constructing a plot of DPOAE levels as a function of frequency. Each point of the DP-gram was recorded using a summation-averaging algorithm. Data were collected in short sections, in each of which the noise level was assessed. The clean data were sub-averaged before being added to the main pool average. Each particular frequency pair was examined, and the new data were added to the pooled data for that frequency pair, thus continuously increasing the SNR. Target sound levels and noise contamination areas were calculated and displayed on the screen (Vinck et al., 1996).
4. Statistical analysis of data
The observed differences in the mean DPOAE amplitude response levels (dBSPL) of the 2f₁ - f₂ levels between the pre- and post-exposure measurements of each session were statistically analysed by means of a repeated measures ANOVA using a commercially available statistical software package (IBM SPSS version 21). Tukey HSD post hoc analysis was carried out to reveal significant differences among the different experimental sessions. Normal distributivity of the data, a requirement for ANOVA, was evaluated by means of the Kolgomorov-Smirnov test. A level of p < .05 was used as the level of significance for this study.
5. Results
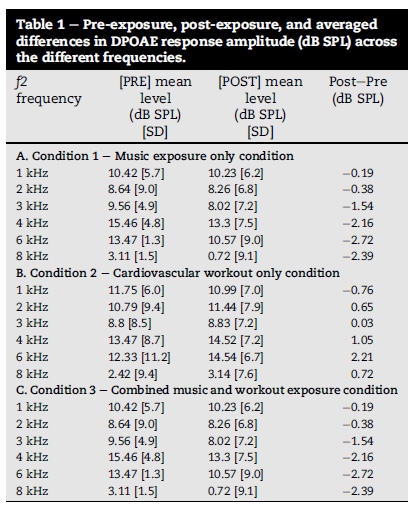
The results obtained following all three testing conditions collected data are presented in Table 1.
5.1. Influence of "music exposure only" condition on DPOAE response
Results obtained from both sets of DPOAE amplitudes across frequencies before and after the 1 h exposure to the music sample via the PMD indicated a minor increase of 0.18 dB SPL in response amplitude, except for 1 kHz. A decrease of the DPOAE response level was observed for all half octave frequency bands between 2 kHz and 8 kHz (Table 1).
Repeated measures one-way ANOVA was carried out to compare the pre-exposure and post-exposure 2f₁ - f₂ response measurements. Although there is a clear trend in decrease of the DPOAE response amplitude over the frequency range 2-8 kHz in the study population, no statistically significant effect (p > .05) was obtained. Thus, no significant effect of listening to the 1 h music sample could be demonstrated on the OHC function.
5.2. Influence of "cardio exposure only" condition on DPOAE response
Results obtained from both sets of DPOAE amplitudes across frequencies before and after the 1 h cardiovascular workout indicated a minor decrease of 0.76 dB SPL in response amplitude, except for 1 kHz. An increase of the DPOAE response level was observed for all half octave frequency bands between 2 kHz and 8 kHz, with a maximum of 2.21 dB SPL at 6 kHz (Table 1).
Repeated measures one-way ANOVA was carried out to compare the 2f₁ - f₂ response measurements between the pre-workout and post-workout session. Although an increase in the DPOAE response amplitude over the frequency range 2-8 kHz in the study population was obtained, no statistically significant effect (p > .05) was obtained. Thus, no significant effect of a 1 h cardiovascular workout on the DPOAE response amplitude could be demonstrated.
5.3. Influence of "combined cardio and music exposure" condition on DPOAE response
Results obtained from both sets of DPOAE amplitudes across frequencies before and after the 1 h combined cardiovascular workout and music exposure indicated a clear trend of decrease in response amplitude for all frequencies. This decrease in DPOAE response level was observed for all half octave frequency bands with a maximum of 2.72 dB SPL at 6 kHz (Table 1).
Repeated measures one-way ANOVA was carried out to compare the 2f₁ - f₂ response measurements between the pre-combined workout and music and post-combined workout and music session. Although a trend of decrease in the DPOAE response amplitudes over the high frequency range in the study population was obtained, no statistically significant effect (p > .05) was obtained. Thus, no significant effect of the combined 1 h cardiovascular workout on the DPOAE response amplitude could be demonstrated.
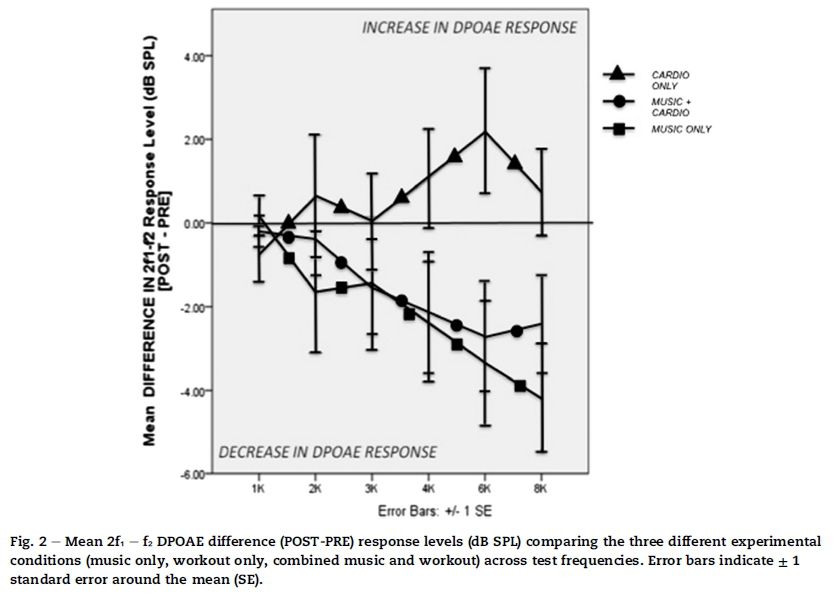
An additional two-way repro (pre-versus post-) x session (music only, cardio only, and music and cardio) interaction analysis was carried out. Fig. 2 shows the graphic output of this response.
Fig. 2 illustrates the difference in profiles of DPOAE amplitudes across frequencies before and after the three experimental sessions (music only, cardiovascular workout only and the combined exposure to music and workout). For the higher frequencies, 4 kHz and higher, a clearly different trend in profile between the different experimental sessions is shown.
The multivariate ANOVA analysis, with Tukey HSD post-hoc testing, showed highly significant differences for the DPOAE test frequencies 6 kHz (F = 4.508, df = 2, p = .014), and 8 kHz (F = 4.448, p = .015). The statistical analysis strongly demonstrates an increase in DPOAE response amplitude for the higher frequencies after performing cardiovascular workout, whereas a significant decrease in DPOAE response amplitude is observed for both of the other conditions (music only and the combination of music and cardiovascular workout).
6. Discussion
During the first condition the effects of PMD use for a time period of 1 h were measured by DPOAEs. Several previous studies focused on determining whether PMD use places young adults at risk for potential hearing damage. Zhao et al. (2010) acknowledge the controversy regarding this topic and further state that music exposure may possibly lead to the development of MIHL. These statements are based on mechanical and physiological changes that occur in the cochlea whilst listening to high intensity music levels. These may include detachment of OHCs from the basilar membrane due to excessive vibration as well as increased levels of glutamate between the IHCs and auditory nerve causing possible ototoxic effects (Zhao et al., 2010). The latter is however relative to the intensity and duration of music exposure (Zhao et al., 2010). Results obtained from a study conducted by Bhagat and Davis (2008) indicated that short-term changes in OAEs may precede the development of a MIHL. Following high intensity music exposure symptomatic effects including TTS can be recorded as measured by DPOAEs supporting the notion of possible early detection of MIHL before evident on the audiogram (Bhagat & Davis, 2008). In accordance with these results a related study indicated that the DPOAE amplitudes were decreased in individuals who were exposed to high intensity output levels (Kumar et al., 2009). Keppler, Dhooge et al. (2010), in a similar study to determine short-term effects of PMD use on the auditory system, did not record significant post-exposure changes and found that the effects were temporary of nature. These temporary changes may however be indicative of potential long term effects of listening to a PMD (Keppler, Dhooge et al., 2010). Fligor (2009) states that the minimal short-term changes are not clinically significant. Most of these studies' outcomes were prompted by the high output levels, listening duration, and general availability of PMDs. This study recorded decreased DPOAE amplitudes between 2 and 8 kHz but cannot be deemed statistically significant. This may be due to the fact that subjects' PMD intensities were not pre-set at a uniform intensity due to ethical recommendations. In spite of this a clear trend of decreased DPOAE amplitudes was observed.
Previous research has also indicated that damage due to noise is usually first evident as a notch in the higher frequencies (Attias et al., 2001, Bhagat and Davis, 2008, Keppler et al., 2010a and Santos et al., 2007). The latter was again observed during this study.
The second testing condition aimed to determine the short-term effects of cardiovascular workout on OHC function in isolation. Limited research pertaining to cardiovascular workout and OHC function is available. Engdahl (1996) concluded that cardiovascular workout significantly increased the noise induced TTS and the effect of noise on DPOAE response amplitudes. According to Hutchinson et al. (2010), cardiovascular workout and fitness may play a protective role in hearing conservation. Cells that are under stress from noise or other damaging agents generate proteins that have positive pharmacological effects protecting the cochlea from damage (Hutchinson et al., 2010). These results correlate with the results obtained in this study, as a clear trend of increased DPOAE amplitudes was recorded between 2 kHz and 8 kHz during cardiovascular workout in isolation.
With regard to the third experimental condition, Vittitow et al. (1994) concluded that a greater TTS is observed during simultaneous cardiovascular workout and noise exposure in comparison to these testing conditions in isolation. In contrast to these results Krishnamurti et al. (2003) found no evidence of auditory changes after short-term exposure to exercise and loud music. A related study indicated that although a TTS occurred following simultaneous exposure, a more significant TTS was observed during noise exposure in isolation (Hutchinson et al., 2010). During the current study's final testing condition of combined PMD use and cardiovascular workout, no statistically significant different results were obtained between the DPOAE response amplitude levels (post - pre) of the music only and combined cardiovascular workout and PMD use. A clear trend of decreased DPOAE response levels after simultaneous cardiovascular workout and PMD use was observed between 2 kHz and 8 kHz. Results obtained from analysis of the difference between post-exposure and pre-exposure of all three experimental testing conditions indicated an increase in DPOAE response amplitude for the higher frequencies after performing cardiovascular exercise, whereas a significant decrease in DPOAE response amplitude was observed for both other conditions (music only and the combination of music and cardiovascular workout) at 6 kHz and 8 kHz.
7. Conclusion
In spite of controversial opinions evident in previous research results, evidence from the current study has indicated that exposure to high levels of music exposure for 1 h through PMD use does not have a significant short-term effect on OHC function, although a clear trend of decreased DPOAE response amplitudes was observed. It is also evident from the results of this study that cardiovascular workout in isolation does lead to a visible increase of DPOAE amplitudes, although not of statistical significance. The simultaneous exposure to cardiovascular workout and PMD use temporarily induces decreased DPOAE response amplitudes although the decrease is not of statistical significance. Pre-exposure and post-exposure results of the three different testing conditions indicated increased DPOAE response amplitudes for the higher frequencies after performing cardiovascular exercise, whereas a significant decrease in DPOAE response amplitude is observed for both other conditions. Thus it can be deducted that PMD use in isolation is indicative of a clear decrease in DPOAE amplitudes in contrast to cardiovascular workout in isolation that indicates an increase in DPOAE amplitudes. The simultaneous use of PMDs and cardiovascular workout displays a similar trend as PMD use in isolation. The latter emphasizes a trend of decreased OHC functioning at 6-8 kHz for PMD use in isolation as well as in the combined condition. In turn, a trend of increased OHC functioning at 6-8 kHz is observed for cardiovascular workout in isolation.
Certain limitations were identified. Comfortable loudness levels may differ between individuals and consequently may affect the severity of the short term and long term effects of PMD use. This could have caused variations across the participant sample. Although a decrease in DPOAE amplitudes were observed after 1 h's PMD use, no statistical differences were obtained. The latter may be due to the variable of differing output levels used by the participants. These intensity levels were not calculated individually and could have influenced the obtained data. This study was conducted in the absence of external auditory stimuli and consequently the effects may differ when a participant is listening to a PMD in a noisy environment such as in a gymnasium with background music. When taking into account the cardiovascular aspect of the study, physiological systems may influence the outcomes of the study. Susceptibility could also contribute to certain responses. In addition to these limitations, the sample size should be increased to ensure a more representative sample.
Future research should attempt to evaluate the long-term effects of cardiovascular workout on OHC function as well as the effects of PMD use over an extended time period. More in-depth assessments of these short-term effects on high frequency (>8 kHz) pure tone audiometry in comparison to DPOAEs could be useful in early identification of potential MIHL. If these short-term effects, as recorded by this study, are not detected by the pure tone audiometry, further research could aim to prove that DPOAEs are more sensitive measures for early identification and diagnosis of MIHL.
References
Alessio, H. M., Hutchinson, K. M., Price, A. L., Reinhart, L., & Sautman, M. J. (2002). Study finds higher cardiovascular fitness associated with greater hearing acuity. The Hearing Journal, 55(8), 32e40. [ Links ]
Attias, J., Horovitz, G., El-Hatib, N., & Nageris, B. (2001). Detection and clinical diagnosis of noise-induced hearing loss by otoacoustic emissions. Noise & Health, 3(12), 19e31. [ Links ]
Bhagat, S. P., & Davis, A. M. (2008). Modification of otoacoustic emissions following ear-level exposure to MP3 player music. International Journal of Audiology, 47, 751e760. [ Links ]
Danhauer, J. L., Johnson, C. E., Byrd, A., DeGood, L., Meuel, C., Pecile, A., et al. (2009). Survey of college students on iPod use and hearing health. Journal of American Academic Audiology, 20, 5e27. [ Links ]
Engdahl, B. (1996). Effects of noise and exercise on distortion product otoacoustic emissions. Hearing Research, 93, 72e82. [ Links ]
Fligor, B. (2009). Personal listening devices and hearing loss: seeking evidence of a long term problem through successful short-term investigation. Noise & Health, 11(44), 129e133. [ Links ]
Haines, N. C., Hodgetts, W. E., Ostevik, A. V., & Rieger, J. M. (2012). Listening levels of teenage iPod users: does measurement approach matter? Audiology Research, 2(6), 25e29. [ Links ]
Hodgetts, W. E., Szarko, R. A., & Rieger, J. M. (2009). What is the influence of background noise and exercise on the listening levels of iPod users? International Journal of Audiology, 48, 825e832. [ Links ]
Hoover, A., & Krishnamurti, S. (2010). Survey of college students' MP3 listening: habits, safety, issues, attitudes, and education. American Journal of Audiology, 19, 73e83. [ Links ]
Hull, R. H., & Kerschen, S. R. (2010). The influence of cardiovascular health on peripheral and central auditory function in adults: a research review. American Journal of Audiology, 19, 9e16. [ Links ]
Hutchinson, K. M., Alessio, H., & Baiduc, R. R. (2010). Association between cardiovascular health and hearing function: puretone and distortion product otoacoustic emission measures. American Journal of Audiology, 19, 26e35. [ Links ]
Keppler, H., Dhooge, I., Maes, L., D'haenens, W., Bockstael, A., Philips, B., et al. (2010). Short-term auditory effects of listening to an MP3 player. Archives of Otolaryngology e Head and Neck Surgery, 136(6), 538e548. [ Links ]
Keppler, H., Vinck, B., & Dhooge, I. (2010). Noise-induced hearing loss in youth caused by leisure noise. New York: Nova Science Publishers, Inc. [ Links ]
Krishnamurti, Sridhar, Grandjean, & Peter, W. (2003). Effects of simultaneous exercise and loud music on hearing acuity and auditory function. National Strength and Conditioning Association, 17(2), 213e416. [ Links ]
Kumar, A., Mathew, K., Alexander, S., & Kiran, C. (2009). Output sound and pressure levels of personal music systems and their effect on hearing. Noise & Health, 11(4), 133e142. [ Links ]
Martin, F. N., & Clark, J. G. (2006). Audiology (9th ed.). USA: Pearson. [ Links ]
NIOSH. (1988). Recommendations for occupational safety and health standards. [ Links ]
Punch, J. L., Elfenbein, J. L., & James, R. R. (2011). Targeting hearing health messages for users of personal listening devices. American Journal of Audiology, 20, 69e82. [ Links ]
Santos, L., Morata, T. C., Jacob, L. C., Albizu, E., Marques, J. M., & Paini, M. (2007). Music exposure and audiological findings in brazilian disc jockeys. International Journal of Audiology, 46, 223e231. [ Links ]
Shah, S., Gopal, B., Reis, J., & Novak, M. (2009). Hear today, gone tomorrow: an assessment of portable entertainment players use and hearing acuity in a community sample. Journal of American Board of Family Medicine, 22(1), 17e23. [ Links ]
Singh, R., Saxena, R. K., & Varshney, S. (2009). Early detection of noise induced hearing loss by using ultra high frequency audiometry. The International Journal of Otorhinolaryngology, 10(2), 1e4. [ Links ]
Sulaiman, A. H., Husain, R., & Seluakumaran, K. (2014). Evaluation of early hearing damage in personal listening device users extended high-frequency audiometry and otoacoustic emissions. European Archives of Otorhinolaryngology, 271, 1463e1470. [ Links ]
Vinck, B. M., De Vel, E., Xu, Z. M., & Van Cauwenberge, P. B. (1996). Distortion product oto-acoustic emissions: a normative study. Audiology, 35, 231e245. [ Links ]
Vittitow, M., Windmill, I. M., Yates, J. W., & Cunningham, D. R. (1994). Effects of simultaneous exercise and noise exposure (music on hearing). Journal of American Academic Audiology, 5, 343e348. [ Links ]
Zhao, F., Manchaiah, V. K. C., French, D., & Price, S. M. (2010). Music exposure and hearing disorders: an overview. International Journal of Audiology, 49, 54e64. [ Links ]
Received 17 June 2015
Accepted 28 January 2016
Available online 31 August 2016
Peer review under responsibility of Johannesburg University.
* Corresponding author. 119 Pendoring Avenue, Wonderboom, Pretoria, 0182, South Africa. Tel.: +27 079 885 1027.
1 Tel.: +27 012 420 2355.


{kind=link}
{kind=link}