










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.21 no.1 Cape Town 2016
http://dx.doi.org/10.1016/j.hsag.2015.11.006
HIV stigma experiences and stigmatisation before and after an intervention
H. Christa ChidrawiI; Minrie GreeffI, *; Q. Michael TemaneI; Colleen M. DoakII
IAfrica Unit for Transdisciplinary Health Research (AUTHeR), North-West University, Private Bag X6001, Potchefstroom, 2520, South Africa
IISection of Infectious Disease, Department of Health Sciences, Vrije University, Amsterdam, Netherlands
ABSTRACT
This study focuses on one aspect of a more extensive SANPAD-funded HIV stigma reduction research project. The study addresses not only the continuous burden of HIV stigma, but more specifically on the low rate of participation in healthcare opportunities and HIV stigma reduction interventions by people living with HIV (PLWH) This study tested both change-over-time in HIV stigma experiences of PLWH and change-over-time in the HIV stigmatisation behaviour of people living close to them (PLC) in an urban and rural setting in the North-West in South Africa. These aspects were measured before and after the comprehensive community-based HIV stigma reduction intervention. A quantitative single system research design, with a pre-test and four repetitive post-tests, and purposive voluntary and snowball sampling were used. Findings did not indicate significant differences between urban and rural settings, but demonstrated some significance in changeover-time in the HIV stigma experiences of PLWH as well as the HIV stigmatisation behaviour of PLC after the intervention. Recommendations include the continuation of this intervention, following the same guidelines that were implemented during the study.
Keywords: Change-over-time, Community-based intervention, HIV stigma experiences, HIV stigmatisation
1. Introduction
HIV infection remains a globally stigmatised condition (Greeff et al., 2008) and HIV stigma remains a complex concept (Mbonye et al., 2013) associated with blame, shame, disgrace and social unacceptability (Mandal, 2013). Fifty years ago Goffman (1963) described stigma as a deeply discrediting personal phenomenon and forty years later, Deacon and Stephney (2007) argued for an even stronger term to more accurately describe stigma. They suggested that a term similar to racism be found that would strongly portray public disapproval of discriminatory and stigmatising behaviour.
HIV stigma manifests as the assertion of a socially constructed "undesired differentness" through acts of ostracism, discrimination, social control, marginalisation and social domination (Herek, Saha, & Burack, 2013). Earlier authors have described it as a disempowerment of PLWH through labelling, stereotyping, separation, diminishing and discrimination (Link, Yang, Phelan, & Collins, 2004). Moreover, according to Kohi et al. (2006), stigma manifests in the violation of human rights which may take the form of refusing to care for PLWH within health facilities, verbal and physical abuse, food deprivation, denial of employment or income opportunities, denial of leadership positions and a so-called justified breach of confidentiality regarding the HIV status of PLWH. Further aspects of psychological distress experienced by stigmatised PLWH include increased physical distance, awkward social interaction, indifference, avoidance, blaming, exaggerated kindness, aggression, exclusion, excessive hygienic measures and being told to disclose or not (Stutterheim et al., 2009).
These complexities led to Holzemer et al. (2007) proposing a four-dimensional process model to facilitate a better understanding of HIV stigma in Africa. The model served as a basic framework for this study as it acknowledges that HIV stigma occurs within an interactive context where environment, the healthcare system as well as people all play a role in the everyday stigma reality. In this model there are four interactive processes of HIV stigma, namely triggers, behaviours, types and outcomes of HIV stigma. This suggests that an HIV test can trigger certain behaviour, lead to a specific type of stigma and result in a definable outcome of stigma for the PLWH.
The types and outcomes of HIV stigma are broadly covered in the literature and are summarised in Fig. 1 to enhance understanding. Internal stigma seems to refer to self-stigmatising (Holzemer et al., 2007) by PLWH or their insider view (Rensen, Bandyopadhyay, Gopal, & Van Brakel, 2011). Received stigma (Holzemer et al., 2007) relates to concepts like perceived/anticipated, outsider-view/external or felt stigma as mentioned by Mak et al. (2007), Weiss et al. (1992) and Herek et al., (2013) respectively, and as such experienced by PLWH as directed towards them. Lastly, associated stigma (Holzemer et al., 2007) or secondary stigma (Ogden & Nyblade, 2005) relates to stigma that stems from someone's association with PLWH and often includes PLC (people living close to PLWH). It is important to understand that stigma may in some instances also arise from PLC participating in stigmatising behaviour towards PLWH.
The experiences of PLWH with the above types of HIV stigma directed at them can be devastating with life-inhibiting emotional, psychological, relational or material outcomes. Repeated experiences of abuse and discouragement to participate in treatment programmes and attend care facilities could lead to diminished physical and mental health (Greeff et al., 2008). Isolation or decreased social participation of PLWH stems from living while fearing stigma and thus minimising their exposure to others (Gilbert & Walker, 2010) which in turn leads to poor participation in healthcare as well as in personal and employment relationships (Greeff et al., 2010). A further outcome of HIV stigma for PLWH relates to self-isolating behaviour to prevent HIV-transmission to others and to minimise secondary (associated) stigma directed at those living close to them (Salter et al., 2010). PLWH often experience personal and emotional frailty coupled with internalised self-stigmatisation, shame and a compromised self-efficacy (Naidoo et al., 2007). This leads to social avoidance, real or perceived loss of friends, perceived discomfort of those they are in contact with, symptoms of depression and feelings of anxiety, hopelessness and unattractiveness (Cahill & Valadez, 2013). All these aspects contribute to a decreased quality of life as an outcome of HIV stigma for PLWH and poor disclosure practices, poor sexual choices or quality-of-life decisions driven by a debilitating, internalised fear of losing significant relationships and losing their source of income/livelihood. Other fears include the fear of losing out on marriage, child-bearing, family care, hope, self-worth and reputation (Kasapoglu, Saillard, Kaya, & Turan, 2011; Rensen et al., 2011). However, HIV stigma could be turned around and lead to positive outcomes if PLWH become involved in actively reducing stigma, accept their HIV status, demonstrate a pleasant disposition, choose positive interpretations of social interactions, refuse the victim role and focus on health, resilience, strengths and capacity and thereby flourish in society (Shih, 2004).
However, the reality is that the South African Medical Research Council (Visser, 2007) some seven years ago found no evidence of HIV stigma reduction in sub-Saharan Africa. Mbonye et al. (2013) recently conducted a longitudinal study in which it was found that there was a decrease in HIV-associated stigma with commencement of anti-retro viral treatment. But the stigma increased again after 18-30 months on treatment and seemed to then persist in the long term. Even HIV status disclosure behaviour decreased as the visible HIV signs and symptoms of the illness decreased.
Furthermore, it is interesting to observe differences of HIV stigma and stigmatisation between urban PLWH and PLC and their rural counterparts. The literature points to complexity and even disagreement among researchers in this regard. This study did not find significant differences between the HIV stigma experiences of PLWH or stigmatisation behaviour within urban and rural communities. The complexities of continuous migration of community members between urban employment and rural homesteads were, however, noted. Voeten, Egesah, and Habbema (2004) suggest that this is one of the reasons why a full understanding of HIV and HIV stigma has been delayed in rural areas. Naidoo et al. (2007) found that urban PLWH faced more received stigma than their rural counterparts and that urban infrastructure facilitates higher reporting on HIV stigma. Heckman et al. (1998) found that urban and rural PLWH in the USA did not differ in age, education, employment, income or HIV symptomatology but that rural PLWH rated the severity of barriers to competent and compassionate care and care facilities higher than urban PLWH. These barriers included a shortage of competent health professionals, long distances to medical facilities, inadequate public transport and painful experiences of stig-matisation. Ankrah (1993) added a lack of privacy, anonymity and confidentiality as common aspects of HIV stigma in rural areas. According to Mswela (2009), unsympathetic and harsh treatment of sick relatives appears to be more common in rural areas.
This study tested an intervention for the reduction of stigma and stigmatising. According to a literature review, studies have been conducted and the outcomes have been reported of historic and recent community-based HIV stigma reduction interventions. During the first 25 years of the AIDS pandemic, the interventions have reported limited success in alleviating the effects of HIV stigma on community, national, and global levels. However by the end of the nineties, Corrigan (2000) implemented the attribution model which focused on replacing incorrect attributions/beliefs with correct ones. The operative elements of this model were protest against inaccurate information and myths, insurance of responsible HIV education, and facilitation of contact between stigmatised and stigmatising people (Corrigan, 2000).
Generally, interventions were based on intrapersonal, interpersonal, community, institutional and governmental strategic levels (Mahajan et al., 2008). The critical elements of such interventions were identified. Brown, Macintyre, and Trujillo (2003) mentioned a set of four elements. These were information to the public, personal contact with PLWH, coping skills for dealing with stigma and applied counselling.
Similarly, Uys et al. (2009) used three basic elements in their intervention, namely accurate information, personal contact with the stigmatised and skills to cope with stigma. Ongoing research started promoting multi-pronged approaches such as a combination of sharing information and building skills, or education and empowerment combined with personal contact (Brown et al., 2003; Holm-Hansen, 2009). An example of this approach is the Cross, Heijnders, Dalal, Sermrittirong, and Mak (2011) matrix which was used as a framework for situa-tional stigma interventions and strategic stigma reduction guidelines. This model was based on the intrapersonal, interpersonal, and organisational and community or governmental levels of stigma and cross-referencing components like labelling, stereotyping, separation, status loss and discrimination.
2. Problem statement and research objective
HIV stigma, HIV stigmatisation and the need for the reduction (and eradication) of both have become a growing international concern. Community-based change needs to reflect specific outcomes like a measurable decrease in the HIV stigma experiences of PLWH as well as in stigmatisation. Such change will ideally also reflect the empowerment of PLWH and the relational enhancement between PLWH and PLC. This study focused on a specific intervention that responded to three research questions. Firstly, is there a difference in the stigma reduction experiences between urban and rural PLWH and PLC following the comprehensive community-based HIV stigma reduction intervention? Secondly, will the comprehensive community-based HIV stigma reduction intervention reduce the stigma experiences of PLWH? Thirdly, will the comprehensive community-based HIV stigma reduction intervention reduce HIV stigmatisation by PLC?
The research objective for this article was thus to observe change-over-time in the HIV stigma experiences of PLWH and the stigmatisation by PLC in both urban and rural settings, following the comprehensive community-based HIV stigma reduction intervention.
3. Research design and methodology
A quantitative single system design (De Vos, Strydom, Fouche, & Delport, 2005) with a pre-test and four repetitive post-test measures (01 χ 02 03 04 05) was implemented. Both an urban and a rural setting were included.
3.1. Sample
The sample for this study comprised two groups representing their respective communities. These groups were representative of an urban and a rural community each, with each having PLWH and PLC groups. This study formed part of a SANPAD-funded study aimed at promoting a deeper understanding of HIV stigma and how people cope with the stigma related to HIV. The study thus also focused on the strengthening of relationships between PLWH and PLC as well as the activation of leadership by both the PLWH and PLC towards the reduction of HIV stigma. The therapeutic nature (Thorne, 2008) of the intervention limited the number of participants because meaningful interaction in small groups was required and non-probability sampling methods were thus used.
Mediators in already trusting relationships with PLWH from the identified urban and rural settings were sourced with the help of existing NGOs and healthcare clinics. These mediators helped the researcher find 18 PLWH by means of purposive sampling. This was followed by snowball sampling to identify PLC for the study.
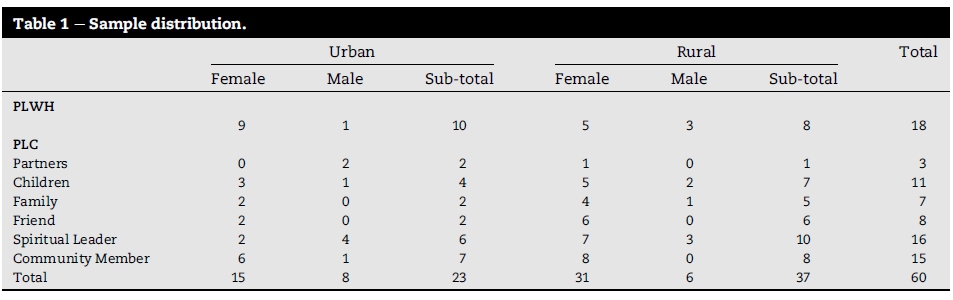
The inclusion criteria for PLWH were as follows: Participants had to be over 18 years old, conversant in either Afrikaans, English or Setswana, HIV-positive for a minimum of six months, and willing to give informed consent for participation and recording of discussions. PLWH participants were also required to openly share in HIV-status disclosure workshops with other PLWH. Furthermore, they were expected to be willing and able to nominate PLC for participation in various workshops of designated groups involving both PLC and PLWH. Eventually, 10 PLWH from the Potchefstroom urban district and eight PLWH from the rural Ganyesa district of the North-West volunteered (see Table 1). All the PLWH were black South Africans. Twelve finished school with Grade 10 or higher, seven held a post-school certificate and one a diploma. Ten persons had no post-school education.
The PLWH participated in snowball sampling for the next part of the study and could nominate six PLC, one from each of six designated categories - a spouse or partner, a child over 15 years of age, a family member, a close friend, a spiritual leader and a community member. Six designated groups were thus formed. The inclusion criteria for nominated PLC corresponded with that of PLWH, except that PLC did not have to be HIV-positive. Not all PLWH were able to nominate a suitable person for each designated group but a total of sixty (n = 60) PLC were identified (see Table 1). There were 23 urban and 37 rural Setswana-speaking participants from the same province. The PLC sample included 93.3% black, 4.8% coloured and 0.3% Indian participants. Of the 60 PLC, 83.3% had passed Grade 10 or higher, 55% had no post-school education, 41.7% had obtained a post-school certificate and 3.4% a diploma or degree.
3.2. The intervention
The intervention was adapted from the validated intervention manual of Uys et al. (2009) and was based on three tenets, namely the a) sharing of information on HIV stigma and coping with HIV stigma, b) the equalising of relationships between PLWH and PLC through increased interaction and contact among them by grouping them together, and c) the empowerment of members of both groups towards leadership in HIV stigma reduction through practical knowledge and experience of project planning regarding HIV stigma reduction and implementation in their communities.
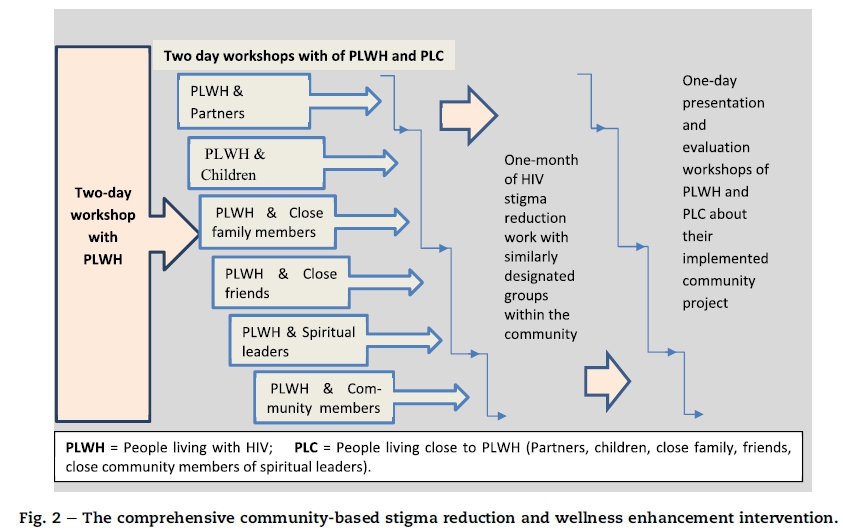
The comprehensive community-based HIV stigma reduction intervention primarily involved three processes (see Fig. 2) and ran over a five-month period in both the urban and rural settings. Firstly, there was a two-day presentation and activity-based workshop for PLWH only. It focused on their personal understanding of HIV stigma, identification of their personal strengths and teaching responsible disclosure management to prepare them for the rest of the workshops in the intervention. This workshop for PLWH was followed by a series of six three-day workshops for each group of PLC: first the group of spouses/partners, then the group of children over 15, then family members, friends, spiritual leaders and, lastly, neighbours or community members. The PLC workshops occurred two weeks apart and were led by two facilitators (one HIV-infected and one non-HIV infected person) for each group. These workshops were attended by all PLWH. The first day of these workshops focused on an understanding of and coping with HIV stigma and the relationship between PLWH and PLC. The second day focused on learning and practising the planning of an HIV stigma reduction project with a group similar to their specific designated group, e.g. partners with a community group of partners. Each of the 12 groups was given a month to implement their projects in their community while receiving support from the facilitators. In the third one-day workshop, the original designated group invited community members as guests and then presented feedback on their projects. Small prizes were awarded by the research team.
3.3. Data collection
The data collection process made use of two structured, valid and reliable measuring instruments, namely the Perceived AIDS Stigma Instrument PLWA (HASI-P) (Holzemer et al., 2007) and the AIDS-Related Stigma Measure for Community HIV Stigma (Maughan-Brown, 2004). A pre-test and four post-tests were conducted on a three-monthly basis over a one-year period for PLWH and PLC in urban and rural settings to test the change-over-time in the HIV stigma experience of PLWH and the stigmatisation by PLC.
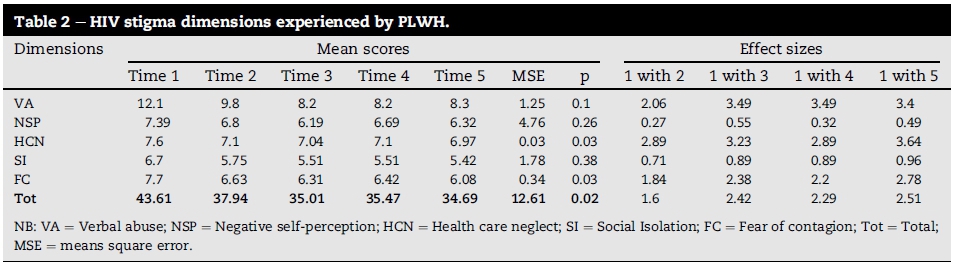
The HIV/AIDS Stigma Instrument PLWH (HASI-P) is a 33-item instrument developed by Holzemer et al. (2007) and measures six dimensions of HIV and AIDS-related stigma (verbal abuse, negative self-perception, healthcare neglect, social isolation, fear of contagion and workplace stigma) experienced by PLWH. It was validated with a sample of 1477 respondents from five African countries. Holzemer et al. (2007) reported a Cronbach reliability coefficient of 0.94 for the total scale. The Cronbach alpha value for subscales of the HIV/AIDS Stigma Instrument PLWA (HASI-P) for PLWH was 0.62 for healthcare neglect (HCN) and alpha values for the other four subscales ranged between 0.77 and 0.85. As the results on all subscales for the 18 PLWH were not statistically significant, effect sizes were compared to analyse potential Cohen devalues and determine practical significance. The community-based HIV stigma intervention was implemented after time one. Time-one scores (see Table 2) thus reflect pre-intervention scores on five different HIV stigma dimensions (subscales) for PLWH. In describing effect sizes, time-one scores are compared with scores on timelines two, three, four and five for each subscale. The 33 item four-point Likert scale used the following scores: 1 = no HIV stigma, 2 = some HIV stigma, 3 = definite HIV stigma, and 4 = high prevalence of HIV stigma.
The AIDS-related Stigma Measure for Community HIV Stigma is a 39-item instrument that measures AIDS-related stigma for community and was developed by Maughan-Brown (2004). With factor analysis, four indices, namely policy/resource-based stigma (PI), behaviour intention stigma (BI), symbolic stigma (SS) and instrumental stigma (IS), are measured on subscales and a combined score is then computed to yield a fifth index indicating general stigma (GS).
Maughan-Brown (2004) reported that initial reliability was established by factor analysis with an alpha coefficient of 0.76 for the factor relating to behaviour intention stigma, 0.59 for the factor relating to symbolic stigma, and 0.55 for the factor relating to instrumental stigma. These indexes tested reliable in this study with Cronbach alpha scores of 0.54, 0.69 and 0.53 respectively.
Symbolic stigma (SS) refers to a moralistic, value-based position or a prejudice-based position for what HIV symbolises for the PLC (Maughan-Brown, 2004). Instrumental stigma (IS) relates to the personally useful stigmatising thoughts or actions that the PLC use for self-protection. For instance, a personal fear of contagion may lead to a person to refuse to share cups or cutlery, to avoid touch or refrain from intimacy (Maughan-Brown, 2004). General stigma (GS) suggests improvement (change over time) in the general stigmatisation by PLC following the intervention. The third research question - whether the comprehensive community-based HIV stigma reduction intervention would reduce HIV stigmatisation by PLC - was thus confirmed.
Only three of the five indexes of this scale for stigmatisa-tion by PLC were used in the analysis because the Behavior Index (BI) refers to policy issues with regard to HIV stigma in the community and were removed from the personal experiences of participants in the particular intervention.
The comprehensive community-based HIV stigma reduction intervention was preceded by training to prepare the research assistants for their task. They were taught how to conduct the interviews, use the instruments and ensure accurate reporting of the process. As the names of the participants became available through the mediators, a research assistant made appointments with them and facilitated the administering of the relevant instruments. Participants were transported to and from the North-West University campus for data collection and workshops. They were also offered a light lunch during the workshops.
3.4. Data analysis
The data analysis for this quantitative data was computed with the Statistical Package for the Social Sciences (SPSS) (Version 21; IBM Corp., 2012). Descriptive statistics, namely mean, standard deviation, mean square error, p values and effect sizes, were calculated. Hierarchical linear modelling was used to estimate variability between urban-rural groups while taking into account the dependency on data collected from specific persons over time (McCoach, 2010).
4. Ethical considerations
Ethical approval was obtained from the School of Nursing Science as well as from the North-West University ethics committee (NWU-OOO 11-09-A1) (30/03/2009-29/03/2014). Permission was also obtained from the North-West Provincial Department of Health as well as the district health authorities. Proceedings were guided by basic ethical principles, like respect for human subjects and benevolence and justice as described by Botma, Greeff, Mulaudzi, and Wright (2010). Thus the participants were provided with information regarding the criteria for their inclusion on a voluntary basis; they were informed that their privacy and anonymity would be guaranteed by means of computer coding, and that their identities would not be linked to the collected data, analysis or study report. Partial confidentiality was ensured through a group contract with the group members. Participants were also informed that they were free to withdraw at any time. They then signed a consent form. The participants were also provided with knowledge and clarification about HIV stigma; they identified their personal strengths and PLWH were taught responsible disclosure management. Their best interests were pursued at all times by enhancing relationships between PLWH and PLC, educating them about HIV stigma reduction and how to cope coping with stigma, as well as providing them with basic skills for managing similar projects in the community. Fair treatment of participants was important and therefore possible risks to them were identified and managed. Counselling was made available to all of them should they need it.
5. Results and discussion
Hierarchical linear modelling was used to estimate variability between urban-rural groups while taking into account the dependency on data collected from specific persons over time (McCoach, 2010). The modelling indicated no statistical significance in the interaction effects of the urban and rural groups in any of the analyses, and no statistical significance was seen in the main effect of urban versus rural groups. The urban/rural results were therefore pooled and the answer to the first research question - whether there would be a difference between urban and rural PLWH and PLC following the comprehensive community-based HIV stigma reduction intervention - was thus no as no significant difference was found. The HIV stigma experiences of PLWH and the stigma-tisation by PLC in the pooled data demonstrated change over time.
5.1. Stigma experiences of PLWH
The comparison of scores reported over time did not give statistically significant results. But there were indications of practical significance when effect changes, Cohens'd' scores as such were reflected. Although not statistically significant (p = 0.10), the numeric value of the mean score on verbal abuse (VA) decreased from m = 12.1 at time one to m = 9.8 at time two and m = 8.3 at time five. This indicated a decreasing tendency by PLWH to experience verbal abuse. Moreover, the effect sizes between times one and two, one and three, one and four as well as one and five were all larger than 0.5. These d-values or effect sizes also indicated practical significance with regard to the change-over-time in the HIV stigma experiences of PLWH. The negative self-perception (NSP) scores of the PLWH were not statistically significant (p = 0.26), but the effect sizes of the decrease between times one and three and times one and five indicated practical significance with values of d = 0.55 and d = 0.49 respectively. The healthcare neglect (HCN) subscale indicated a statistical significant improvement in healthcare of PLWH with p = 0.03 while these were confirmed by the four effect sizes ranging between d = 2.89 and d = 3.64 and indicated practical significance as well. The subscale of social isolation (SI) did not show statistical significance but demonstrated practical significance with effect sizes between 0.71 and 0.96 (d > 0.5) on the four timeline comparisons to time one. This was an indication of improvement in how different social isolation linked to HIV stigma was experienced by PLWH after the intervention. Lastly, fear of contagion (FC) indicated clear statistical significance with p = 0.03 in change-over-time in the experiences of HIV stigma by PLWH. All five dimensions of HIV stigma on the HASI-P scale indicated improvement (change-over-time) in the HIV stigma experiences of PLWH after the intervention.
The summation of the scores of each of the timelines introduced the opportunity of a total stigma score for each (see Table 2). The score of p = 0.02 thus indicated statistical significance of change-over-time after the intervention on the total scores. The effect sizes for indication of practical significance on total HIV stigma experiences of PLWH indicated even stronger differences between times one and three of verbal abuse (VA), negative self-perception (NSP) and healthcare neglect (HCN). It also revealed large effect sizes between times one and five of the social isolation (SI) and fear of contagion (FC) scales. In terms of the second research question it was found that stigma experiences of PLWH were reduced following the community-based stigma reduction intervention.
5.2. Stigmatisation by PLC
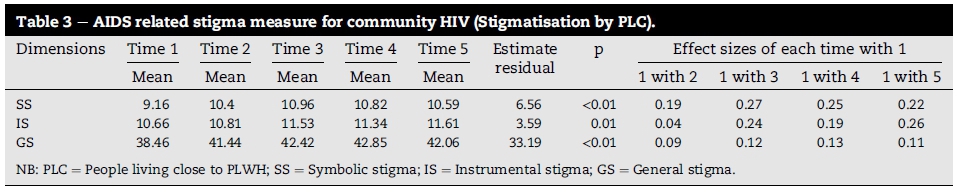
The AIDS-related stigma measure for community HIV scale was used to measure symbolic stigma (SS), instrumental stigma (IS) and general stigma (GS) of HIV stigmatisation in PLC. Results as seen in Table 3 showed statistically significant increases for all three mentioned subscales.
As symbolic stigma (SS) referred to an almost immovable moralistic, value-based position or a type of prejudice for what HIV symbolises in the mind of the PLC (Maughan-Brown, 2004), ideally PLC should have become capable of moving from their prejudice as a result of the intervention. The mean score for symbolic stigma (SS) at time one (m = 9.2) reflected the pre-intervention measure for PLC and increased to m = 10.6 at time five. This gave a statistically significant result (p < 0.01) and indicated change-over-time in the stigmatisation by PLC. In addition, effect sizes between the compared timelines on symbolic stigma (SS) demonstrated practical significance as the d-scores between times one and three and one and four were exceptionally large, measuring 0.70 and 0.65 respectively. There was thus a change-over-time in symbolic HIV stigma experiences and the potential shift in PLC prejudice was confirmed by practical significant results.
The scale for instrumental stigma (IS), similar to the above scale, needed to demonstrate meaningful shifts away from certain personally useful stigmatising thoughts or actions (instruments) used by PLC for self-protection. For instance, a personal fear of contagion could justify someone's refusal to share cups or cutlery, or avoidance to touch or refrain from intimacy (Maughan-Brown, 2004). The instrumental index (IS) at time one pre-intervention was m = 10.7, and increased to m = 11.6 at time five. The p vale of 0.01 indicated a statistical significant difference and the effect size of times one and five (d = 0.50) gave a practical significant result. This could possibly indicate that the tenets of the intervention (HIV knowledge sharing, relationship equalisation and personal empowerment) helped to replace older stigmatising patterns, thoughts and actions.
The general stigma (GS) index for PLC also offered a statistical significant result, with an increase at time one (m = 38.5) to m = 42.1 at time five and p < 0.01. Again, there were also an indication of practical significance as well, as all four effect sizes were larger than d = 0.50. These results suggested a change-over-time in the general stigmatisation behaviour by PLC following the intervention. It was thus found that the comprehensive community-based HIV stigma reduction intervention did indeed reduce HIV stigmatisation by PLC.
6. Conclusions
The urban and rural groups did not demonstrate significant differences over time. While not proven, this could have been due to the homogeneity and the inherent cultural similarities in the mainly Setswana-speaking population in both the urban and their rural counterparts. There was HIV stigma though. The PLWH responses on each first measure of the subscales confirmed the presence of HIV stigma which showed consistently on all five dimensions measured. The study offered an opportunity to measure and interpret data in terms of traditional statistical significant results as well as a method of demonstrating practical significant results where effect changes justified this. This methodology contributed to the inclusion of change-over-time in experiences and stig-matisation observed in interaction but not always measured in statistics. Results indicated the decline of HIV stigma experiences of PLWH on all the dimensions: verbal abuse, negative self-perception, healthcare neglect, social isolation by others and fear of contagion. The change-over-time in the overall stigma experiences of PLWH indicated by the total HIV stigma score showed a statistical significant result which thus indicates that the community-based stigma reduction intervention was successful. The third timeline measure, about three months after the intervention, revealed large effect size changes which could be indicative of personal benefits derived from the community-based HIV stigma reduction intervention. The linear correlation among the five HIV stigma dimensions indicates the tangency and even complexity of HIV stigma where variability between urban-rural groups is estimated while working with data collected from the specific people over time. As a result, a multi-dimensional approach was taken for the intervention and research.
Three of the five indices for stigmatisation by PLC indicated statistical significant change. Similar to the findings of the experiences of PLWH, large effect size scores featured at the third measure about three months after the intervention as PLC started to internalise the effects of the intervention. The symbolic enhancement is indicative of a change in the moralistic behaviour of PLC and fewer prejudices. PLC also realised that they probably did not need the symbolic behaviour to protect themselves from becoming infected. This could be due to the increased contact between PLWH and PLC. The type of prejudice-based HIV stigma intent measured by symbolic, instrumental and general stigma scales included the opinion that HIV was punishment for sleeping around, refusal to admit HIV-positive children to public schools and fear of touching someone with HIV. All these stigmatising thoughts and actions of the PLC showed reduced incidences. It can thus be concluded that stigmatisation by PLC was reduced through the intervention.
The change-over-time in the HIV stigma experiences of PLWH occurred concurrently with the change-over-time in the HIV stigmatisation behaviour by PLC. These changes in stigma experiences and stigmatisation were sustained over a one-year period after the intervention, showing that the impact on both PLWH and PLC relatively long lasting. The preparation of PLWH to understand HIV stigma, manage their disclosure responsibly and identify their strengths laid a foundation for the rest of the workshops with PLC. Using a team of infected and non-infected facilitators as well as bringing both PLWH and PLC together in the same workshop underlined the importance of equal relationships. In this way equality, acceptance and working together could be modelled practically. The fact that both the stigma experiences and stigmatisation changed, show that the approach of the intervention and its content were effective at bringing about changes. The interaction and contact between participants normalised the social interaction, offered opportunities to share experiences and activated support for each other. The projects that were undertaken by the PLWH and the PLC together as leaders in stigma reduction in their own community could have led to the reduction of fear of contagion. Both PLWH and PLC regained some control after HIV became a reality in their lives. If all PLC of PLWH could be included in such programmes as this one, more understanding of the stigmatisation process could be effected thus leading to a change in attitude in the entire community.
The intensity and time that the intervention required over a four-month period required much energy from the PLWH at times, but it did lead to positive results. There is no doubt that participants benefitted from the therapeutic nature of the intervention that provided skilled facilitators to a small number of participants within a structured environment. The community-based HIV stigma reduction intervention helped to bridge the gap in the quest for successful HIV reduction interventions. Mbonye et al. (2013), however, have warned that it is possible that HIV stigma and stigmatisation can return once PLWH reach the next level of seeking parity and equality in labour and reproductive issues.
7. Limitations of the study
The sample size of PLWH was small. It was deliberately kept small in order to accommodate the therapeutic nature of the intervention which required small group interaction and the building of personal relationships among PLWH and PLC. It also required pairs of well skilled facilitators of whom one had to be HIV-positive and the other not, so as to model a positive relationship between PLWH and PLC. The snowball sampling method in recruiting PLC was also limited as it was dependent on the PLWH. This resulted in some uncertainty regarding the eventual numbers of PLC since availability of potential participants for the six specified categories (spouses, children, family members, friends, spiritual leaders, neighbours/community members) could not be established beforehand.
8. Recommendations
The comprehensive community-based HIV stigma reduction intervention could serve as a useful tool in communities. In future interventions, the snowball sampling of PLC could be carried out without the restriction of designated categories. An aspect of culture sensitivity could be added to cater for diversity in communities. The basic tenets, methodology, participation, ethical considerations and programmatic expertise should, however, be retained. Groups should be kept small enough to ensure therapeutic benefit and PLWH should never be exposed to intervention content without being well prepared. A set of guidelines should be compiled for future implementation of the intervention. It would be helpful to have the intervention tested in a variety of cultures and locations with a view to building community-based networks and structures to eradicate HIV stigma and enhance wellness in the community at large. Such actions could perhaps also address the issues mentioned by Mbonye et al. (2013) whereby HIV stigma and stigmatisation could return after some time of initial decline. A booster type intervention at time three may also contribute to long-term sustainability of change-overtime in the reduction of HIV stigma experiences and stigma-tisation after a successful intervention.
Funding
The authors received research funds and student bursaries from SANPAD.
Acknowledgements
• SANPAD for the student bursary and financial support.
• Dr. Suria Ellis for statistical consult, direction and support.
• Poncho Molaudzi for research assistance, dedication and enthusiasm.
• Fieldworkers for their graceful contribution and human connection.
• The PLWH and PLC for their selfless sharing and honest participation.
REFERENCES
Ankrah, E. M. (1993). The impact of HIV/AIDS on the family and other significant relationships: the African clan revisited. AIDS Care. Psychological and Socio-Medical Aspects of HIV//Aids, 5(1), 5-22. [ Links ]
Botma, Y., Greeff, M., Mulaudzi, F. M., & Wright, S. C. D. (2010). Research in health science. Cape Town, South Africa: Pinelands. [ Links ]
Brown, L., Macintyre, K., & Trujillo, L. (2003). Interventions to reduce HIV/AIDS stigma: what have we learned? AIDS Education and Prevention, 15(1), 49-69. http://dx.doi.org/10.1521/aeap.15.1.49.23844. [ Links ]
Cahill, S., & Valadez, R. (2013). Growing older with HIV/AIDS: new public health challenges. American Journal of Public Health, 3(3), 7-15. http://dx.doi.org/10.2105/AJPH.2012.301161. [ Links ]
Corrigan, P. W. (2000). Mental health stigma as social attribution: implications for research methods and attitude change. Clinical Psychology: Science and Practice, 7(1), 48-67. http://dx.doi.org/10.1093/clipsy.7.1.48. [ Links ]
Cross, H., Heijnders, M., Dalal, A., Sermrittirong, S., & Mak, S. (2011). Interventions for stigma reduction - Part 1: theoretical considerations. Disability. CBR & Inclusive Development, 22(3), 62-70. http://dx.doi.org/10.5463/dcid.v22i3.70. [ Links ]
De Vos, A. S., Strydom, H., Fouche, C. B., & Delport, C. S. L. (2005). Research at grass roots: For the social sciences and human service professions (3rd ed.). Pretoria, South Africa: Van Schaik. [ Links ]
Deacon, H., & Stephney, I. (2007). HIV/AIDS, stigma and children. Cape Town: HSRC Press. [ Links ]
Gilbert, L., & Walker, L. (2010). My biggest fear was that people would reject me once they knew my status: stigma as experienced by patients in an HIV/AIDS clinic in Johannesburg, SA. Health and Social Care in the Community, 18(2), 139-146. http://dx.doi.org/10.1111/j.1365-2524.2009.00881.x. [ Links ]
Goffman, E. (1963). Stigma: Notes on the management ofspoilt identity. Englewood Cliffs, NJ: Prentice Hall. [ Links ]
Greeff, M., Uys, L. R., Holzemer, W. L., Makoae, L. N., Dlamini, P. S., Kohi, T. W., et al. (2008). Experiences of HIV/ AIDS stigma of persons living with HIV/AIDS and nurses involved in their care from five African countries. Africa Journal of Nursing and Midwifery, 10(1), 78-108. [ Links ]
Greeff, M., Uys, L. R., Wantland, D., Makoae, L., Chirwa, M., Dlamini, P., et al. (2010). Perceived HIV stigma and life satisfaction among persons living with HIV infection in five African countries: a longitudinal study. International Journal of Nursing Studies, 47(4), 475-486. http://dx.doi.org/10.1016/j.ijnurstu.2009.09.008. [ Links ]
Heckman, T. G., Somlai, A. M., Peters, J., Walker, J., Otto-Salaj, L., Galdabini, C. A., et al. (1998). Barriers to care among persons living with HIV/AIDS in urban and rural areas. AIDS Care: Psychological and Socio-medical Aspects ofHIV/AIDS, 10(3), 365-375. http://dx.doi.org/10.1111/j.1748-0361.1998.tb00615.x. [ Links ]
Herek, G. M., Saha, S., & Burack, J. (2013). Stigma and psychological distress in people with HIV/AIDS. Basic and Applied Social Psychology, 35(1), 41-54. http://dx.doi.org/10.1080/01973533.2012.746606. [ Links ]
Holm-Hansen, C. (2009). Stigma reduction: promoting greater understanding of mental health. Wilder Research Snapshot, 1-4. [ Links ]
Holzemer, W. L., Uys, L., Makoae, L., Stewart, A., Phetlhu, R., Dlamini, P. S., et al. (2007). A conceptual model of HIV/AIDS stigma from five African countries. Journal of Advanced Nursing, 58(6), 541-551. http://dx.doi.org/10.1111/j.1365-2648.2007.04244.x. [ Links ]
Kasapoglu, A., Saillard, E. K., Kaya, N., & Turan, F. (2011). AIDS related stigma in social relations: a qualitative study in Turkey. The Qualitative Report, 16(6), 1496-1516. [ Links ]
Kohi, T. W., Makoae, L., Chirwa, M., Holzemer, W. L., Phetlhu, D. R., Uys, L., et al. (2006). HIV and AIDS stigma violates human rights in five African countries. Nursing Ethics, 13(4), 405-414. http://dx.doi.org/10.1191/0969733006ne865oa. [ Links ]
Link, B. G., Yang, L. H., Phelan, J. C., & Collins, P. Y. (2004). Measuring mental illness stigma. Schizophrenia Bulletin, 30(3), 511-541. [ Links ]
Mahajan, A. P., Sayles, J. N., Patel, V. A., Remien, R. H., Ortiz, D., Szekeres, G., et al. (2008). Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS, 22(2), 67-79. http://dx.doi.org/10.1097/01.aids.0000327438.13291.62. [ Links ]
Mak, W. W. S., Cheung, R. Y. M., Law, R. W., Woo, J., Li, P. C. K., & Chung, R. W. Y. (2007). Examining the attribution model of self-stigma on social support and psychological well-being among people with HIV+/AIDS. Social Science & Medicine, 64(8), 1549-1559. http://dx.doi.org/10.1016/j.socscimed.2006.12.003. [ Links ]
Mandal, A. (2013). AIDS-stigma. News medical. Retrieved from http://www.news-medical.net/health/AIDS-Stigma.aspx. [ Links ]
Maughan-Brown, B. (2004). Measuring HIV/AIDS stigma: Working Paper No. 74. Cape Town: Centre for Social Science Research [CSSR], University of Cape Town. Retrieved from http://cssr.uct.ac.za/sites/cssr.uct.ac.za/files/pubs/wp74.pdf.
Mbonye, M., Nakamanya, S., King, R., Seeley, J., Birungi, J., & Jaffar, S. (2013). Stigma trajectories among people living with HIV (PLHIV) embarking on a life time journey with antiretroviral drugs in Jinja, Uganda. BMC Public Health, 13(1). http://dx.doi.org/10.1186/1471-2458-13-804. [ Links ]
McCoach, D. B. (2010). Hierarchical linear modelling. In G. R. Hancock, & R. O. Mueller (Eds.), The reviewer's guide to quantitative methods in the social sciences (pp. 123-140). New York, NY: Routledge. [ Links ]
Mswela, M. (2009). Cultural practices and HIV in South Africa: a legal perspective. Potchefstroom Electronic Law Journal, 12(4), 172-360. http://dx.doi.org/10.4314/pelj.v12i4.50053. [ Links ]
Naidoo, J., Uys, L., Greeff, M., Phetihu, R., Holzemer, W., Makoae, L., et al. (2007). Urban and rural differences in HIV/AIDS stigma in five African countries. African Journal of AIDS Research, 6(1), 17-23. http://dx.doi.org/10.2989/16085900709490395. [ Links ]
Ogden, J., & Nyblade, L. (2005). Common at its core: HIV-related stigma across context. Washington DC, WA: International Center for Research on Women (ICRW). Retrieved from http://www.icrw.org/files/publications/Common-at-its-Core-HIV-Related-Stigma-Across-Contexts.pdf. [ Links ]
Rensen, C., Bandyopadhyay, S., Gopal, P. K., & Van Brakel, W. H. (2011). Measuring leprosy-related stigma - a pilot study to validate a toolkit of instruments. Disability and Rehabilitation, 33(9), 711-719. http://dx.doi.org/10.3109/09638288.2010.506942. [ Links ]
Salter, M. L., Go, V. F., Le Minh, N., Gregowski, A., Ha, T. V., Rudolph, A., et al. (2010). Influence of perceived secondary stigma and family on the response to HIV infection among injection drug users in Vietnam. AIDS Education & Prevention, 22(6), 558-570. http://dx.doi.org/10.1521/aeap.2010.22.6.558. [ Links ]
Shih, M. (2004). Positive stigma: examining resilience and empowerment in overcoming stigma. The ANNALS of the American Academy of Political and Social Science, 591(1), 175-185. http://dx.doi.org/10.1177/0002716203260099. [ Links ]
Stutterheim, S. E., Pryor, J. B., Bos, A. E. R., Hoogendijk, R., Muris, P., & Schaalma, H. P. (2009). HIV-related stigma and psychological distress: the harmful effects of specific stigma manifestations in various social settings. AIDS, 23(17), 2353-2357. http://dx.doi.org/10.1097/QAD.0b013e3283320dce. [ Links ]
Thorne, S. (2008). Interpretive description. Left Coast, CA: WalnutCreek. [ Links ]
Uys, L. R., Chirwa, M. L., Kohi, T. W., Greeff, M., Naidoo, J. R., Makoae, L. N., et al. (2009). Evaluation of a health setting-based intervention. AIDS Patient Care and STDs, 23(12), 1059-1066. http://dx.doi.org/10.1089/apc.2009.0085. [ Links ]
Visser, P. (2007). HIV/AIDS and stigma. South African Medical Research Council [MRC]. [ Links ] Retrieved from http://www.afroaidsinfo.org/MRCWeb/portlets/AutonomyRetrieval/autosuggest.js p?username=e8e9e6e5f9e0 f8&threshold=20&numresult=10&defaultlogo=i_html.gif&display =774&url=22195&links=HIV,AID,STIGMA,VISSER&command=getoriginal.
Voeten, H. A. C. M., Egesah, O. B., & Habbema, J. D. F. (2004).Sexual behaviour is more risky in rural than in urban areasamong young women in Nyanza Province, Kenya. SexuallyTransmitted Diseases, 31(8), 481-487. [ Links ]
Weiss, M. G., Doongaji, D. R., Siddhartha, S., Wypij, D., Parhare, S., Bhatawdekar, M., et al. (1992). The explanatory model interview catalogue (EMIC): contribution to cross-cultural research methods from a study of leprosy and mental health. The British Journal of Psychiatry, 160, 819-830. http://dx.doi.org/10.1192/bjp.160.6.819. [ Links ]
Received 5 February 2015
Accepted 16 November 2015
* Corresponding author. Tel.: +27 18 299 2092; fax: +27 18 299 2088. E-mail addresses: Minrie.Greeff@nwu.ac.za (M. Greeff), c.m.doak@vu.nl (C.M. Doak).
Peer review under responsibility of Johannesburg University.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}