










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkHealth SA Gesondheid (Online)
On-line version ISSN 2071-9736
Print version ISSN 1025-9848
Health SA Gesondheid (Online) vol.19 n.1 Cape Town Jan. 2014
http://dx.doi.org/10.4102/HSAG.V19I1.809
ORIGINAL RESEARCH
Nurses' knowledge of chronic disease management
Saloshni NaidooI; Ozayr H. MahomedII; Shaidah AsmallIII; Myra TaylorII
IOccupational and Environmental Health, School of Nursing and Public Health, University of KwaZulu-Natal, South Africa
IIPublic Health Medicine, School of Nursing and Public Health, University of KwaZulu-Natal, South Africa
IIISenior Technical Advisor, South African National Department of Health: PACTSA, South Africa
ABSTRACT
BACKGROUND: Chronic diseases of lifestyle are detrimentally affecting South Africans. National Health Insurance, which is intended to improve care, requires capacity building for nurses at primary care clinics to ensure appropriate service provision
OBJECTIVE: This study's objective was to evaluate the impact of the 'Primary Care 101' chronic disease management guideline and training on nurses' knowledge of chronic diseases management
METHOD: A population-based, unblinded, stratified cluster randomised controlled trial with intervention (n = 20) and control clinics (n = 10) in three South African districts was conducted over six months in 2012. Nurses in the clinics participated in surveying knowledge on management of tuberculosis, human immunodeficiency virus infection, mental health, epilepsy, diabetes, hypertension and asthma and chronic obstructive pulmonary disease (COPD). All nurses were surveyed at baseline and six months later. Intervention clinic nurses were also surveyed immediately after training and three months post-training. Data were analysed using SPSS version 19 (SPSS Inc., Chicago, IL).Total mean knowledge percentage scores were calculated for each chronic disease. Mean knowledge percentage score changes between baseline and six months amongst all nurses and between intervention and control clinic nurses were compared using the paired samples t-test and independent samples t-test respectively
RESULTS: There were significant improvements in nurses' knowledge of hypertension and diabetes management over six months. Knowledge about asthma and COPD management decreased in all districts and nurse categories
CONCLUSION: The improvements in nurses' knowledge can ensure improved patient management, but attention to asthma and COPD management is required
OPSOMMING
AGTERGROND: Chroniese lewenstylsiektes beïnvloed Suid-Afrikaners nadelig. Die nasionale gesondheidsversekering, wat ten doel het om sorg te verbeter, vereis kapasiteitsbou vir verpleegsters by primêre-sorg-klinieke om sodoende toepaslike dienslewering te verseker
DOELWITTE: Hierdie studie se doel was te evalueer wat die impak van die 'Primary Care 101' chroniese siekte bestuursriglyn, asook opleiding is op verpleegsters se kennis van hoe om chroniese siektes te bestuur
METODE: 'n Bevolkingsgebaseerde, onverblinde, ewekansige gekontroleerde trossteekproef met ingrypings- (n = 20) en kontrole-klinieke (n = 10) is oor 'n tydperk van ses maande in 2012 in drie Suid-Afrikaanse distrikte uitgevoer. Verpleegsters in hierdie klinieke het deelgeneem aan 'n opname oor hul kennis oor die bestuur van tuberkulose, menslike immuniteitsgebreksvirus-infeksie, geestesgesondheid, epilepsie, diabetes, hoë bloeddruk, asook asma en chroniese obstruktiewe longsiekte (COPD). Alle verpleegsters is by die basislyn ondervra en ses maande later. Intervensie kliniekverpleegsters is ook ondervra onmiddellik na die opleiding en drie maande post-opleiding. Data is ontleed met behulp van SPSS, weergawe 19 (SPSS Inc, Chicago, IL). Totale gemiddelde kennis persentasietellings is vir elke chroniese siekte bereken. Veranderinge in die gemiddelde kennis persentasietellings tussen die basislyn en ses maande later is onder alle verpleegsters, asook tussen ingrypings- en kontrole-kliniekverpleegsters vergelyk met behulp van die gepaarde steekproef t-toets en die onafhanklike steekproef t-toets onderskeidelik
RESULTATE: Daar was 'n aansienlike verbetering in verpleegsters se kennis oor die bestuur van hoë bloeddruk en diabetes na ses maande. Kennis oor die bestuur van asma en COPD het in alle distrikte en verpleegster-kategorieë afgeneem
GEVOLTREKKING: Die verbetering in die verpleegsters se kennis kan verbeterde pasiëntbestuur verseker, maar die bestuur van asma en COPD vereis verdere aandag
Introduction
South Africa's population is experiencing a multiple burden of disease. Human immunodeficiency virus infection and/or acquired immune deficiency syndrome (HIV/AIDS) and tuberculosis (TB) (Harrison 2009) still account for the major part of the disease burden. However, the prevalence of non-communicable diseases (NCDs) such as diabetes and hypertension are on the increase (Mayosi et al. 2009; Peer et al. 2012; Phaswana-Mafuya et al. 2013; Peer et al. 2013). HIV and/or AIDS and TB infections, injury due to personal violence and accidents, cardiac diseases, diarrhoeal diseases, lower respiratory tract infections and poverty-related disease such as protein-energy malnutrition are estimated to account for approximately 90% of the premature mortality in South Africa (Harrison 2009).
Chronic diseases of lifestyle are affecting all population groups in South Africa. Research in the urban black population of the Western Cape Province reported the prevalence of hypertension and diabetes to be 35.6% and 12.5% respectively (Peer et al. 2012; Peer et al. 2013). A population-based survey of self-reported NCDs found the prevalence of all NCDs to be 51.8%, with approximately 22.5% of respondents having two or more NCDs. Being of mixed race (OR 1.50, 95% CI 1.05-2.15) or Indian race (OR 1.59, 95% CI 1.08-2.34) was significantly associated with having an NCD (Peer et al. 2012; Peer et al. 2013).
With the improved treatment and care for people diagnosed with HIV, the life expectancy of the South African population has been increasing. In KwaZulu-Natal between 2003 and 2011 the life expectancy of a population cohort increased from 49.2 years prior to implementation of anti-retroviral treatment to 60.5 years with availability of antiretrovirals (Bor et al. 2013). This increased life expectancy allows for the development and an increasing burden of NCDs as the population ages.
This increase in the burden of NCDs has implications for the health system and service provision in the country. In 1994 the National Health Plan for South Africa was developed based on the delivery of health care through a District Health System utilising a district-based primary healthcare approach (Kautzky & Tollman 2008). This would ensure access to health care for all, with the first point of entry into the health system being via the primary health clinic, and the first contact being with a primary health clinic nurse. However, access to health care for all has not been achieved. Instead, both public and private health systems have persisted with an almost equal distribution of expenditure between the two systems, even though the public sector caters for the majority of the South African population (Naidoo 2012).
In 2011 the South African National Department of Health (NDoH) published a Green Paper on their policy for National Health Insurance (NHI) as a means of transforming the health system to achieve the earlier intentions of access to quality healthcare services for all (Matsoso & Fryatt 2013). In order to achieve this, the current public health system will have to be overhauled and strengthened to provide a comprehensive package of care at a primary healthcare level. This would mean that nurses will be responsible for service provision including chronic disease management. They will be supported by general medical practitioners contracted to provide services at primary health clinics with a view to eventually expanding to accredit existing private medical practices (Matsoso & Fryatt 2013).
This will require appropriate capacity building for nurses at primary health clinic level to ensure that they are able to contribute appropriately to the provision of services. Currently there are efforts under way to ensure that service providers are appropriately equipped to provide quality services. The Practical Approach to Lung Health in South Africa (PALSA) was developed by the Knowledge and Translation Unit affiliated to the University of Cape Town. This programme trained nurse trainers who in turn trained primary health clinic nurses to use evidence-based management guidelines to improve management of patients with TB, obstructive lung diseases and lower and upper respiratory tract infections. The guideline has an algorithmic format which uses a syndromic approach to patient management (Fairall et al. 2005; Bheekie et al. 2006). Use of PALSA by primary health clinic nurses in the Free State Province of South Africa showed an improvement in TB case detection and treatment of asthma (Fairall et al. 2005).
The PALSA training initiative has been developed further to include the management of patients with HIV and/or AIDS and those on antiretroviral treatment, commonly referred to as PALSA-PLUS (Stein et al. 2008). In addition, on-site training of nurses by nurse trainers was incorporated into the training initiative. Nurses trained in the PALSA-PLUS programme appreciated the simplicity of the approach and found the on-site training to be more relevant (Stein et al. 2008). These successes resulted in the NDoH contracting the Knowledge and Translation Unit to develop an expansion of the PALSA-PLUS programme to include all priority chronic diseases. The PALSA-PLUS guideline has been expanded to address 40 common presenting symptoms and 17 chronic conditions in adults within one 101-page compendium known as 'Primary Care 101' or 'PC 101'. This guideline retains many aspects of the original PALSA guideline, including the symptom-based algorithmic approach (South African NDoH 2011).
Problem statement
The NDoH has also adopted an Integrated Chronic Disease Management model for the management of all chronic diseases. This model has its origin in public health principles focusing on the reorganisation of primary health clinics to improve service delivery. This involves providing support for the clinical management of patients with outreach teams supporting, managing and empowering patients to take responsibility for their chronic disease treatment (Asmall & Mahomed 2011). The Integrated Chronic Disease Management model will be beneficial in the NHI programme by improving the management of patients with chronic diseases. However, it requires appropriate capacity building for primary health clinic nurses to manage patients with chronic diseases of lifestyle.
As part of the Integrated Chronic Disease Management model implementation, PC 101 was used to train primary health clinic nurses in the management of chronic diseases. The NDoH requested that an independent evaluation be conducted by an academic institution to assess whether the PC 101 guideline and training programme achieved the expected outcomes in imparting knowledge and competencies, to assess the quality of care provided, and the impact on management of patients with chronic diseases. This evaluation was undertaken before and after the training and implementation of the PC 101 guideline.
Research objective
In this study we sought to establish if there had been changes in primary health clinic nurses' knowledge of the management of chronic diseases, from baseline to six months after completing the PC 101 training.
Research methods and design
Study design
This was a population-based, unblinded, stratified cluster randomised controlled trial evaluating the impact of the PC 101 intervention conducted over a six-month period in 2012 in three health districts in three provinces in South Africa. The primary health clinics were the cluster. In the health districts a complete list of primary health clinics was obtained, and clinics were randomly chosen to receive the intervention. Control clinics were matched to the intervention clinics. Participating staff and the study team were aware of which primary health clinics were receiving the intervention.
Population and sampling
The primary health clinic was selected as the unit of randomisation. The 20 intervention primary health clinics are sites in which the Integrated Chronic Disease Management model was being implemented. Twenty primary health clinics received the intervention (cases) and 10 primary health clinics did not receive the intervention (controls). All nurses working in the 30 selected primary health clinics were invited to participate in the study.
The intervention
The study intervention comprised a training programme developed to train nurses in primary health clinics on managing patients with chronic diseases. There were two parts to the training programme. The first part was the training material, which made use of the PC 101 guideline, and the second was the training process and method of training. The PC 101 guideline and training material provide a stepwise approach to managing patients with chronic conditions including hypertension, diabetes, cardiovascular disorders, TB, HIV, sexually transmitted infections, asthma, chronic obstructive pulmonary disease (COPD), depression, anxiety, psychoses, substance abuse, dementia, musculoskeletal conditions, epilepsy, skin conditions and women's health.
For evaluation of the training intervention used in this study we focused on hypertension, diabetes, epilepsy, depression, TB, HIV and/or AIDS, asthma and COPD. The training content was focused on recognising symptoms, diagnosing and managing patients with the above chronic diseases. There was information on when to refer patients to hospital and advice to give patients presenting with each chronic disease. Nurses were trained to follow an algorithm in diagnosis and managing each of the chronic diseases.
The training method used for the intervention was based on the 'train the trainer' principle. In May 2012 staff from the Knowledge and Translation Unit at the University of Cape Town trained master and facility trainers and professional nurses on using the PC 101 guideline and training manual. The master and facility trainers had to conduct eight training sessions at each intervention primary health clinic over a six-month period on the use of the PC 101 guideline. The eight training sessions in each of the intervention primary health clinics was used as a method of reinforcing the initial training the nurses had received in May 2012.
Measurement instrument
A knowledge assessment questionnaire was developed by the research team. The questions and expected answers relating to the chronic conditions were based on the content in the PC 101 training manual which was used to train the nurses. This questionnaire consisted of 150 closed- ended questions requiring 'yes' or 'no' answers with 10 to 35 questions on the chosen chronic diseases. The final questionnaire was approved by representatives from the Mental Health and Substance Abuse and Human Resources Directorates in the South African NDoH and a Senior Technical Advisor to the South African NDoH at a meeting with the research team. Minor corrections to the questionnaire were made to ensure clarity and ease of understanding.
The questionnaire was piloted amongst nurses who worked in primary health clinics prior to use in the study. Amendments were made to questions which were found to be ambiguous and questions which could have multiple answers were refined to ensure that only one correct answer was possible. The questionnaire focused on the symptom presentation and management of the following chronic diseases: (1) TB (20 questions); (2) HIV (30 questions); (3) mental health (20 questions); (4) epilepsy (10 questions); (5) hypertension (20 questions); (6) diabetes (35 questions); and (7) asthma and COPD (15 questions). The self-administered questionnaire was distributed to participating nurses, each of which took an average of 30 minutes to complete due to the categorical nature of the questions.
Data collection
Data were collected at four stages during the study. During all stages of the study the questionnaires were distributed to the nurses and collected by the research team. In stages one (T1) and four (T4) nurses from the intervention and control clinics completed questionnaires. In stages two (T2) and three (T3) only nurses from the intervention clinics completed questionnaires. At stage one all participating nurses (intervention and control clinics) were given the self-administered questionnaire to complete, and nurses from the control clinics completed the questionnaire at their primary health clinic whilst nurses from the intervention clinics completed it prior to the start of their PC 101 training at the training venue. In stage two nurses from the intervention clinics were asked to complete the questionnaire immediately after they had finished their PC 101 training at the training venue. In stage three nurses from the intervention clinics completed the questionnaire at their respective primary health clinics, three months after their PC 101training had been completed. Stage four of the study occurred six months after completion of the PC 101 training for nurses from the intervention clinics. In stage four nurses from the control and intervention clinics completed the questions at their respective primary health clinics. All participants were given a unique study number which was used throughout the study period.
Data analysis
Data were analysed using IBM SPSS version 19 (SPSS Inc., Chicago, IL). Descriptive statistics were presented for the demographic data. Each of the 150 questions was scored one for a correct answer and zero for an incorrect answer, with a total score of 150 achievable. Failure to answer a question was scored as zero. A total score above 80% indicated having adequate knowledge, since this is generally accepted as having a good level of knowledge. All test scores were converted from points to percentages for the analysis. Total mean percentages and subsection mean percentages for the different diseases were calculated for knowledge about each chronic disease and categorised by nursing job category, subdistrict and intervention group T1 and T2. Changes in the knowledge score percentages between T1 and T2, T1 and T3, T1 and T4 amongst the nurses were compared using the paired samples t-test. Standard deviations for the mean change of score percentages were reported. The mean differences in knowledge between nurses from the intervention and control groups were compared using the independent samples t-test at T1 and at T4. The accepted level of statistical significance was α = 0.05.
Results
The participation rates of nurses in each phase of the study varied considerably (T1 [n = 171]; T2 [n = 53]; T3 [n = 99]; T4 [n = 109]). Only 2 nurses participated in all 4 phases of the study. Of the 171 nurses who participated at T1, 49 nurses participated in T2, 44 nurses participated in T3 and 70 nurses participated in T4. Nurses from the control clinics did not participate in the second and third phases of the study. The results presented in this article focus on T1 and T4.
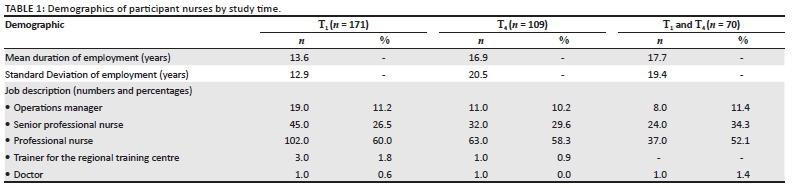
Demographic profile of participating nurses
The duration of employment of participating nurses ranged from a mean of 13.6 years (SD 12.9 years) to a mean of 17.7 years (SD 19.4). The majority of participants in each phase were professional nurses (Table 1). There were no significant differences in duration of employment as a nurse between the 70 nurses who participated in both T1 and T4 and those who participated only in T1 (n = 101) (p = 0.4). Similarly, there were no significant differences in duration of employment as a nurse between the 70 nurses who participated in both T1 and T4and those who participated only in T4 (n = 39) (p = 0.6).
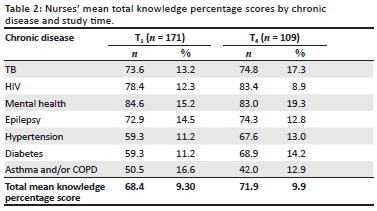
Mean total knowledge percentage scores at each phase of the study amongst all nurses
Nurses' mean total knowledge percentage scores were highest for mental health patient management in all phases of the study, ranging between 84.6% (SD 15.2) and 83.0% (SD 19.3). Mean total knowledge percentage scores were above 70% for TB and HIV patient management in all phases of the study. Mean total knowledge percentage scores remained persistently low for asthma and/or COPD patient management through all phases of the study, ranging between 50.5% (SD 9.3) and 42.0% (SD 12.9) (Table 2).
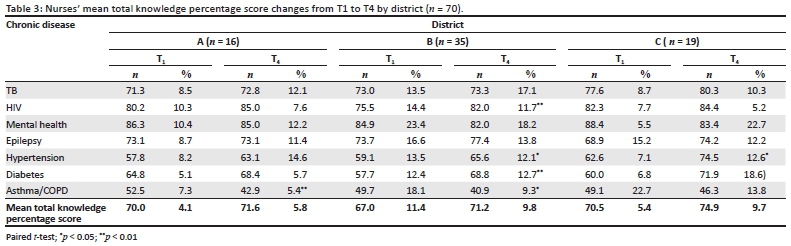
Mean total knowledge percentage score changes from T1 to T4 by district
Mean total knowledge percentage scores improved in all districts from T1 to T4. The mean total knowledge percentage scores for hypertension and diabetes management increased significantly in district B from T1 to T4 (hypertension: p < 0.05; diabetes: p < 0.01) and district C (p < 0.05). The mean total knowledge percentage score for HIV management significantly improved in district B from T1 to T4 (p < 0.01). There were significant decreases in mean total knowledge percentage scores for asthma and/or COPD management in districts A (p < 0.01) and B (p < 0.05) from T1 to T4. Whilst not statistically significant, there was a decrease in mental health mean total knowledge percentage scores in all districts from T1 to T4 (Table 3).
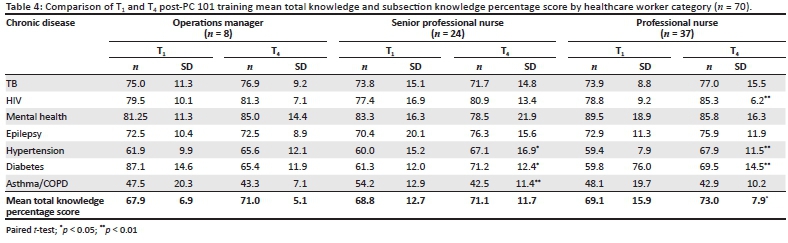
Mean total knowledge percentage score changes from T1 to T4 by nurse category
The mean total knowledge percentage scores of professional nurses increased significantly from 69.1% at T1 to 73.4% at T4 (p = 0.02). There was no significant change in mean total knowledge percentage scores amongst the operations managers and senior professional nurses from T1 to T4. There were significant improvements in mean total knowledge percentage scores for hypertension and diabetes from T1 to T4 amongst the professional nurses (p < 0.01) and senior professional nurses (hypertension: p = 0.03; diabetes: p = 0.01). Asthma and/or COPD mean total knowledge percentage scores decreased amongst all categories of nurses. There was a significant decrease in mean total knowledge percentage scores for asthma and/or COPD management from T1 to T4 amongst the senior professional nurses (p < 0.01) (Table 4).
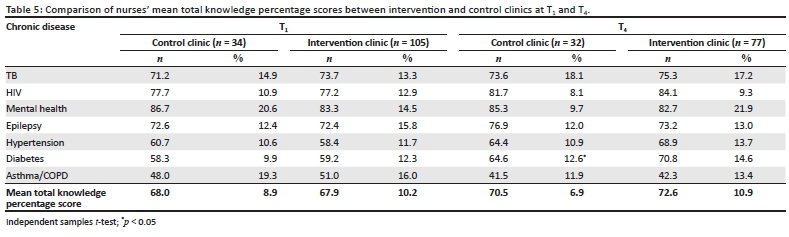
Mean total knowledge percentage scores differences between nurses working in intervention and control clinics at T1 and T4
The mean total knowledge percentage scores amongst nurses from the intervention and control clinics were compared at T1 and T4. The mean knowledge percentage scores of the nurses in the control and intervention clinics reflected that of the entire group of nurses at T1 and T4, with their knowledge being consistently high with regard to the management of mental health patients and consistently poor with regard to management of asthma/COPD. There was no difference in mean knowledge percentages scores between intervention and control clinic nurses at T1,but at T4 there was a significant difference with regard to mean diabetes management knowledge percentage scores (p = 0.04) between intervention and control clinic nurses. At T4nurses from the control clinics displayed better knowledge on mental health and epilepsy than nurses from the intervention clinics, although this was not statistically significant (Table 5).
Ethical considerations
The protocol was approved by the Biomedical Research Ethics Committee at the University of KwaZulu-Natal (UKZN (BE 006/12). Permission to undertake the project was obtained from the South African NDoH. All nurses employed in the selected primary health clinics were invited to participate in the study. Written informed consent was obtained from the participants prior to the interviews and execution of the data collection tool. Participation was voluntary. Nurses were provided with a written information sheet detailing the study objectives, and informed of their right to withdraw from the study at any time.
All participants were given a unique study number for use in each phase of the study, and no names were used. The questionnaires are kept under lock and key in the Discipline of Public Health Medicine, University of KwaZulu-Natal. Only the principal investigator has access to the questionnaires.
Validity and reliability
Reliability
The questionnaire used in this study was piloted prior to use in the field. It was piloted amongst nurses of a similar training background as those who participated in this study. The Cronbach alpha for the questions ranged from 0.42 for questions on epilepsy to 0.91 for questions on mental health, indicating good reliability of the questionnaire.
Validity
The questions relating to each chronic disease and expected correct answers were based on the training content in PC 101. This was verified by a panel of members including representatives from the NDoH, which ensured content validity of the questionnaire. Participants' responses to questions relating to each chronic disease were analysed to check for a sequence of responses which confirmed good construct validity.
Discussion
The findings of this study confirm that training with the PC 101 guideline does improve nurses' knowledge on the management of chronic diseases, but also highlighted problems which need to be addressed. The knowledge improvements were seen after training using the PC 101 guideline, whether categorised by district or category of nurse. This supports the findings of previous studies (Fairall et al. 2005; Stein et al. 2008) which evaluated the PALSA and PALSA-PLUS training programmes which gave rise to the PC 101 guideline.
The high knowledge percentage scores seen with respect to TB, HIV and mental health chronic patient management is reflective of the diseases on which the majority of training initiatives in South Africa have concentrated. Programmes such as Nurse Initiated Management of Antiretroviral Treatment (Nyasulu et al. 2012), PALSA and PALSA-PLUS have focused on the management of patients with HIV infection and TB (Fairall et al. 2005; Stein et al. 2008). Mental health has been an integrated service provided by nurses at a primary level, and they have been involved in prescribing medication for patients with chronic mental illnesses (Lund et al. 2012).
The improvements in mean knowledge percentage scores for the management of hypertension and diabetes seen in this study are very promising. With the high prevalence of hypertension and diabetes that is now being reported in South Africa (Peer et al. 2012; Peer et al. 2013), the need for nurses in primary health clinics to have correct knowledge on management of patients with these chronic diseases is important. Previous intervention work focusing on diabetes in Soweto has also shown that nurses receiving training on management of patients with diabetes had better knowledge than nurses who had not received the training (Katz et al. 2009).
Asthma and COPD contribute significantly to the burden of chronic respiratory diseases in South Africa (Mayosi et al. 2009). Patients with respiratory diseases do present at primary health clinics for management by nurses, making knowledge about disease management a necessity. In all of the study districts the asthma and/or COPD mean knowledge percentage scores were the poorest compared to those for other diseases and decreased by T4. Comparing T1 asthma and/or COPD mean knowledge percentage scores to T4 knowledge levels, there was a significant decrease overall (p < 0.01, result not shown) and also in districts A (p < 0.01) and B (p = 0.01).
Research previously showed that training with PALSA positively impacted on the prescriptions for obstructive lung diseases (Fairall et al. 2005). Clearly, despite the training in our study there were no improvements with regard to knowledge about these specific chronic conditions. In attempting to address this, two aspects need to be considered. The essential information which primary health clinic nurses should know about managing the diseases and what is currently provided in the guideline must be reviewed. Whilst not researched in this study, the training methods on asthma/COPD should be examined to ensure that there is no confusion concerning the information being provided to nurses.
A serious concern in the study was failure to retain the nurses for the duration of the study, and to ensure that the same nurses from the intervention clinics participated at all four stages of the study. Similarly, we were unable to ensure that the nurses from the control clinics who participated at T1 also participated at T4. At T4 109 nurses participated in the survey compared to 171 nurses who were involved at T1. An estimated 50% (n = 70) of the nurses who participated in the survey at T1 participated at T4. Furthermore, amongst the nurses from the intervention clinics only two nurses participated in all four phases of the study. During site visits it was established that nurses were being rotated through clinics in the district. A number of nurses who completed the survey at T1 were community service nurses, and once they finished their community service they were moved to other primary health clinics. As a result, nurses who had participated in the survey at T1 were not always present at a facility to participate in follow-up surveys.
The repeated training sessions at the primary health clinics were meant to reinforce the training that nurses received at T1. However, if the nurses had moved from the facility it meant that their initial training was not reinforced and the intervention had been undermined. Whilst one would like to target all nurses during the training sessions in order for the intervention to succeed, trained senior nurses should have been retained at the facility. Furthermore, to ensure the methodological integrity of the study training had to continue at the intervention clinics and could not be moved as nurses moved from one primary health clinic to another. Katz et al. (2009) reported that staff allocated to management of patients were rotated, and this affected patient management. Staff turnover because of heavy workloads can also influence implementation of chronic disease management programmes (Katz et al. 2009; Parker et al. 2012).
Interestingly there were no differences in knowledge between the nurses from the intervention and control clinics at T4. The potential for cross-over bias that may occur in a randomised controlled trial did exist in this study. There were nurses who had been trained at T1 from the intervention who may have been rotated to control clinics, and the researchers had no control over this. These nurses could have shared information with nurses at the control clinics. Stein et al. (2008), reporting on a process evaluation of PALSA-PLUS nurse training, described a nurse from a control clinic making copies of the guideline for use in her clinic.
The sustainability of programmes such as PC 101 is dependent on nurses remaining at a primary health clinic to benefit from refresher training sessions. Nurses rotating through primary health clinics are unavailable for refresher sessions, negatively impacting on the sustainability of training programmes. Furthermore, training initiatives were given considerable financial support by the NDoH, and efforts should be made to ensure that they are successful. If primary health clinics are to provide the package of services for NHI then closer attention has to be paid to such training initiatives to ensure that capacity is built amongst nurses.
Limitations of the study
Although due diligence was exercised in maintaining the scientific integrity of the study, the main limitation was the loss to follow-up or non-participation of nurses. At T1 171 nurses participated in the questionnaire survey, whilst at T4 109 nurses participated, of whom only 70 had participated at baseline. Furthermore, at T3 and T4 the nurses filled out the questionnaire at the facility level. Despite communicating with nurses there was no way to ensure that all nurses completed the questionnaire, as this was dependent on voluntary participation.
The burden of chronic diseases in the South African population is increasing, requiring appropriate healthcare management. In addition, the South African Government is rolling out the NHI system, which will be implemented through primary health clinics. This study identified gaps in primary health clinic nurses' knowledge about chronic disease management which need to be addressed to improve the implementation of NHI.
Recommendations
The recommendations outlined below are based on the study findings.
Staff retention and training at clinics
Staff rotation should be minimal so that the PC 101 training can be properly implemented. Continuous training of nurses at the clinics is required. In-facility training should take place monthly. District-level training should be scheduled at least six-monthly to minimise service disruption at the primary health clinics. These refresher training sessions are needed to ensure that knowledge is reinforced.
Staff participation
All nurses responsible for chronic patient management should be targeted for training. In addition, nurses who received initial training and who moved on to other clinics should be included in facility training efforts. This will ensure that their initial knowledge is built upon and not lost.
Training programme content
The current discipline-specific experts involved in the development of PC 101 should review the training material currently being used for training nurses responsible for chronic disease patient management in primary health clinics. Decisions must be made on the exact content which nurses at primary health clinics need to know for chronic disease patient management. Furthermore, content on asthma/COPD patient management in the training guideline for nurses together with the training methods on this topic must be reviewed to ensure that nurses are receiving appropriate and explicit information. Innovative practical methods have to be developed and implemented to ensure that nurses understand and implement the core elements of asthma/COPD chronic patient management.
Conclusion
This study found an improvement in nurses' knowledge from T1 to T4. There were significant improvements in knowledge in certain districts with respect to hypertension and diabetes patient management. However, knowledge about asthma and/or COPD patient management decreased in all districts and amongst all categories of nurses between T1 and T4. There were no differences in knowledge levels amongst nurses from the intervention and control clinics. Greater attention has to be paid to staff retention in primary health clinics and the content being used for training nurses on the management of patients with chronic diseases, to ensure successful patient management. This in turn is likely to contribute to the successful functioning of the NHI system through primary health clinics in South Africa.
Acknowledgements
The research was funded by the United States Agency for International Development (USAID) through the Rapid Response Mechanism for HIV and AIDS via Pact Prime Award No. 647-A-00-08-00001.
The authors would like to acknowledge the assistance provided to them by officials from the South African NDoH, North West Provincial Department of Health, Gauteng Department of Health, Mpumalanga Department of Health, the district management teams and staff from the participating clinics in the three districts.
Competing interests
The authors declare that they have no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
Authors' contributions
O.H.M. (University of KwaZulu-Natal) developed the proposal for the main project with contributions by S.N. (University of KwaZulu-Natal) and M.T. (University of KwaZulu-Natal) S.A. (South African National Department of Health) reviewed the proposal and participated in implementation of the study. S.N. analysed the data for knowledge evaluation and drafted the manuscript with editorial and technical input to the article by O.H.M. and M.T.
References
Asmall, S. & Mahomed, O.H., 2011, Controlling non communicable disease through health system strengthening, Concept Paper for discussion at NCD Summit-2011, South African National Department of Health, viewed 03 December 2013, from http://www.doh.gov.za/docs/misc/2011/through_systControllingNonCommunicable Disease through Health System Strengtheningem_streng.pdf. [ Links ]
Bheekie, A., Buskens, I., Allen, S., English, R., Mayers, P., Fairall, L., Majara, B., Bateman, E.D., Zwarenstein, M. & Bachmann M., 2006, 'The practical approach to lung health in South Africa (PALSA) intervention: Respiratory guideline implementation for nurse trainers', International Nursing Review 53(4), 261-268. [ Links ]
Bor, J., Herbst, A.J., Newell, M.L. & Bärnighausen, T., 2013, 'Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment', Science 22, 961−965. [ Links ]
Fairall, L.R., Zwarenstein, M., Bateman, E.D., Bachmann, M., Lombard, C., Majara, B.P., Joubert, G., English, R.G., Bheekie, A., Van Rensburg, D., Mayers, P., Peters, A.C. & Chapman, R.D., 2005, 'Effect of educational outreach to nurses on tuberculosis case detection and primary care of respiratory illness: Pragmatic cluster randomised controlled trial', British Medical Journal 331(7519), 750-754. [ Links ]
Harrison, D., 2009, An overview of health and health care on South African 1994-2010: Priorities, progress and prospects for new gains, discussion document commissioned by the Henry J. [ Links ]
Kaiser Family Foundation to help inform the National Health Leaders' Retreat, Muldersdrift, 24-26 January 2010, viewed 02 December 2013, fromhttp://www.doh.gov.za/docs/reports/2010/overview1994-2010.pdf [ Links ]
Katz, I., Schneider, H., Shezi, Z., Mdleleni, G., Gerntholtz, T., Butler, O., Manderson L. & Naicker, S.,2009, 'Managing type 2 diabetes in Soweto - The South African Chronic Disease Outreach Program experience', Primary Care Diabetes 3(3),157-164. [ Links ]
Kautzky, K. & Tollman, S.M., 2008, 'A perspective on primary health care in South Africa', in P. Barron & J. Roma-Reardon (eds.), South African Health Review 2008, Health Systems Trust, Durban, viewed 10 November 2013, from http://www.hst.org.za/publications/841 [ Links ]
Lund, C., Petersen, I., Kleintjes, S. & Bhana, A., 2012, 'Mental health services in South Africa: Taking stock', African Journal of Psychiatry 15(6), 402-405. [ Links ]
Matsoso, M.P. & Fryatt, R., 'National Health Insurance: The first 18 months', in A. Padarath & R. English (eds.), South African Health Review 2012/13, Health Systems Trust, Durban; 2013, viewed 20 November 2013, from http://www.hst.org.za/publications/south-african-health-review-2012/13 [ Links ]
Mayosi, B.M., Flisher, A.J., Lalloo, U.G., Sitas, F., Tollman, S.M. & Bradshaw, D., 2009, 'The burden of non-communicable diseases in South Africa', The Lancet 374(9693), 934-947. [ Links ]
Naidoo S., 2012. 'The South African national health insurance: A revolution in health-care delivery!', Journal of Public Health 34(1),149-150. [ Links ]
Nyasulu, J.C., Muchiri, E., Mazwi, S.L. & Ratshefola, M., 2012, 'NIMART rollout to primary healthcare clinics increases access to antiretrovirals in Johannesburg: An interrupted time series analysis', South African Medical Journal 103(4), 232-236. [ Links ]
Parker, W.A., Steyn, N.P., Levitt, N.S. & Lombard, C.J., 2012, 'Health promotion services for patients having non-communicable diseases: Feedback from patients and health care providers in Cape Town, South Africa', BioMed Central Public Health 12, 503. [ Links ]
Peer, N., Steyn, K., Lombard, C., Lambert, E.V., Vythilingum, B. & Levitt, N.S., 2012, 'Rising diabetes prevalence among urban-dwelling black South Africans', PLoS One 7(9), e43336. [ Links ]
Peer, N., Steyn, K., Lombard, C., Gwebushe, N. & Levitt N., 2013, 'A high burden of hypertension in the urban Black population of Cape Town: The Cardiovascular Risk in Black South Africans (CRIBSA) Study', PLoS One 8(11):e78567. [ Links ]
Phaswana-Mafuya, N., Peltzer, K., Chirinda, W., Musekiwa, A., Kose, Z., Hoosain, E., Davids, A. & Ramlagan, S., 2013, 'Self-reported prevalence of chronic non-communicable diseases and associated factors among older adults in South Africa', Global Health Action 6, 20936. [ Links ]
South African National Department of Health, Primary Care 101 Integrated Guideline, Pretoria, South African National Department of Health; 2011/2012. [ Links ]
Stein, J., Lewin, S., Fairall, L., Mayers, P., English, R., Bheekie, A., Bateman, E. & Zwarenstein, M., 2008, 'Building capacity for antiretroviral delivery in South Africa: A qualitative evaluation of the PALSA PLUS nurse training programme', BioMed Central Health Services Research 18(8), 240. [ Links ]
 Correspondence:
Correspondence:
Saloshni Naidoo
3rd Floor, George Campbell Building
Howard Campus, Science Drive, Durban 4001
South Africa
naidoos71@ukzn.ac.za
Received: 24 Dec. 2013
Accepted: 12 June 2014
Published: 21 Nov. 2014


{kind=link}
{kind=link}
{kind=link}
{kind=link}