










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.19 no.1 Cape Town ene. 2014
http://dx.doi.org/10.4102/hsag.v19i1.776
ORIGINAL RESEARCH
Child and youth care workers: profile, nutrition knowledge and food safety and hygiene practices
Hendrina H. Grobbelaar; Carin E. Napier
Department of Food and Nutrition Consumer Sciences, Durban University of Technology, South Africa
ABSTRACT
BACKGROUND: Facilities concerned with children 'in need of care' should not only be considered as a last resort for a child's care, but also as an intervention that requires more than addressing a child's basic physical needs. The nutritional needs of children are particularly important to consider as they are a fundamental part of the care provided.
OBJECTIVES: The purpose of this descriptive quantitative study was to investigate the profile, nutrition knowledge, food safety and hygiene practices of child and youth care workers (CCWs) in residential care settings in order to guide the development of a food preparation and nutrition manual.
METHOD: The residential care settings included in this study were three that were selected randomly in Durban. CCWs (N = 40) employed permanently or part-time were included. Convenience purposive sampling of the CCWs was undertaken. A structured self-administered questionnaire, developed and tested for this purpose, was used to gather information on the profile, nutrition knowledge, food safety and hygiene practices. The data were analysed for descriptive statistics (means and frequencies).
RESULTS: The majority of CCWs were women aged 18-34 years. Very few had completed a relevant tertiary qualification. The results indicated that the respondents' knowledge was fair on general nutrition guidelines, but there were areas of concern. Specifically, knowledge on recommended fruit and vegetable intake, correct serving sizes and importance of a variety in the diet were lacking. Some knowledge about food safety and hygiene practices was demonstrated, but not in totality.
CONCLUSION: The overall findings supported the development of a comprehensive food preparation and nutrition manual for child residential care facilities.
ABSTRAKTE
AGTERGROND: Fasiliteite gemoeid met kinders 'in die behoefte van sorg' nie net beskou moet word as 'n laaste uitweg vir 'n kind se sorg nie, maar ook as 'n intervensie wat meer as net die basiese en fisiese behoeftes van kinders aanspreek. Die voedingsbehoeftes van kinders is veral belangrik om te oorweeg as 'n fundamentele element van versorging.
DOELWIT: Die doel van hierdie beskrywende kwantitatiewe studie was om die profiel, voeding kennis en voedsel- veiligheid en higikne van kinder-en jeugsorgwerkers te ondersoek in residensikle sorg instellings met die doel om 'n voedsel voorbereiding en voedings handleiding te ontwikkel.
METODE: Die residensikle sorg instellings het bestaan uit drie ewekansig gekiesde kinderhuise in Durban. Die studie het bestaan uit kinder-en jeugsorgwerkers (N = 40) in permanente of deeltydse poste. 'n Doelgerigte steekproef van die kinder-en jeugsorgwerkers is onderneem. 'n Gestruktureerde self-geadministreerde vraelys, ontwikkel en getoets vir hierdie doel, is gebruik om inligting oor die profiel, voeding kennis, voedselveiligheid en higikniese praktyke van die kinder- en jeugsorgwerkers in te samel. Die data is ontleed vir beskrywende statistieke.
RESULTATE: Die meerderheid van die kinder- en jeugsorgwerkers was vroulik, tussen die ouderdomme van 18-34 jaar. Min het 'n toepaslike tersijre kwalifikasie gehad. Dit blyk uit die resultate dat die respondente se algemene voeding riglyne was aanvaarbaar. Die resultate het gedui op 'n gebrek aan kennis oor die aanbevole vrugte en groente inname, korrekte porsiegroottes en die belangrikheid van 'n verskeidenheid in die dieet. Die respondente het tot 'n mindere mate kennis oor voedselveiligheid en higikne gehad.
GEVOLGTREKKING: Die algemene bevindinge ondersteun die ontwikkeling van 'n omvattende voedsel voorbereiding en voedings handleiding vir kinder residensikle sorg instellings.
Introduction
Background
In sub-Saharan Africa it was estimated that, in 2005, 12% of children aged 0-17 years were orphans, which amounted to 48 300 000 children (United Nations Children's Fund [UNICEF] 2009). In 2007, an estimated 47.5 million children in sub-Saharan Africa had lost one or both parents to Acquired Immunodeficiency Syndrome (AIDS) or other causes (UNICEF 2009). In addition, the General Household Survey indicated that there were approximately 3.4 million orphans in South Africa in 2005. It was verified in this survey that almost half of all the orphans lived in two provinces, namely KwaZulu-Natal (23%; n = 864 643 children) and the Eastern Cape (25%; n = 796 525 children). The survey also indicated that the number of double orphans (children whose parents had both died) living in KwaZulu-Natal in 2005 was estimated to be 199 623 (Meintjies, Leatt & Berry 2006). No current statistical data are available to indicate how many of these orphans are living in residential care settings.
The Children's Amendment Act 41 of 2007 (South Africa 2007) emphasises that Child and Youth Care Centres should provide therapeutic programmes appropriate to children's developmental and other needs. Above all, the legislation also highlights that residential care should not only be considered as a last resort for a child's care, but also as an intervention that requires more than merely addressing children's basic physical needs. The majority of these centres in South Africa are run by welfare organisations; only a handful countrywide are managed entirely by the government (Meintjies et al. 2007).
Child and youth care workers (CCWs) in these centres are encouraged to register with the National Association of Child and Youth Care Workers (NACCW). In order to improve the quality of care of at-risk children, this association allows for interaction with a network of colleagues and access to continuous professional development opportunities. The association offers both non-accredited and South African Qualifications Authority-accredited training. The accredited training provided is linked to 14 unit standards of the Further Education and Training certificate in Child and Youth Care work (NACCW 2011). Basic care of children requires an understanding of the key aspects of developmental, therapeutic and health care and encompasses physical, social and emotional care and support (Nahikian-Nelms 1997).
Childhood is a critical phase in physical growth and physiological development; for this reason, the nutritional needs of children are particularly important to consider, as they are a fundamental part of healthcare. Adequate nutrients provide what is needed for maintenance of health, growth and prevention of diseases (Wenhold, Kruger & Muehlhof 2008). Micronutrient malnutrition, in particular, results in reduced resistance to infections, as well as delayed or impaired physical and psychomotor development (World Health Organization [WHO] 2002).
The World Health Report of 2002 confirmed that iodine, iron, vitamin A and zinc deficiencies were identified as being the most serious health risk factors worldwide (WHO 2002). Manary and Solomons (2004) pointed out that deficiencies in vitamin D, calcium, zinc, vitamin B12 and riboflavin are also emerging as a public concern. Micronutrient malnutrition is a concern, not just because such a large number of individuals are affected, but also because it can contribute to high rates of morbidity and mortality (WHO 2002).
The National Food Consumption Survey of 2005 indicated that in South Africa, two out of three children had a poor vitamin A status, one out seven had a poor iron status and four and a half out of 10 had a poor zinc status (Labadarios et al. 2008).
The recent South African National Health and Nutrition Examination Survey (SANHANES-01) indicated a prevalence of anaemia in 10.7% of children younger than five years. In the same age groups, 43.6% of the children were vitamin A deficient. Overweight and obesity levels in children in South Africa are alarming, with the SANHANES 2013 study reporting that 16.5% and 17.1% of girls aged 2-14 years were either overweight or obese, respectively. The boys reflected overweight and obesity levels of 11.5% and 4.7%, respectively (Human Sciences Research Council [HSRC] 2013). On the other hand, wasting, stunting and underweight are also indicators of poor nutrition and, combined with deficiencies in vitamin A and zinc, contribute to more than one third of all child deaths worldwide (WHO 2013). In South Africa, 9.4% of children aged 7-9 years are stunted, 1.9% are wasted and 6.6% are underweight (HSRC 2013).
The causes of malnutrition in children are a combination of many contributing factors and can be categorised as either basic, underlying or immediate (Ganyaza-Twalo & Viviers 2012). The immediate causes of malnutrition are associated with dietary intake, stress, trauma and disease (Matji 2008:840). Vorster (2009:4) confirms that immediate causes also include health status, social structures, dietary practices and personal choice. Immediate causes of malnutrition are influenced by the underlying causes of malnutrition. Household food security, maternal and child care practices, inadequate caring capacity of vulnerable groups, education, the availability and access to health services, as well as environmental influences, are underlying causes of malnutrition (Matji 2008:841). Furthermore, the size of the family, family composition and rules of food distribution in the family further contribute to underlying causes (Vorster 2009:5). In turn, the underlying causes are affected by the basic causes of malnutrition. Basic causes are the availability and control of resources, as well as the socio-political, cultural and economic factors that affect the availability and control of these resources (Matji 2008:840).
Various strategies have been implemented in South Africa to prevent malnutrition. Firstly, to address the high prevalence of micronutrient deficiencies, the Department of Health (DoH) implemented a compulsory food fortification programme (Witten et al. 2003). Salt was fortified with iodine in 1995 and in October 2003, it became legally applicable to fortify maize and wheat flours with eight micronutrients, namely, vitamin A, thiamin, riboflavin, niacin, folic acid, pyridoxine, iron and zinc. Secondly, promoting diversity of food intake is seen as being the most sustainable way of addressing micronutrient malnutrition as it can address several micronutrient deficiencies concurrently (WHO & FAO 2006). Thirdly, micronutrient supplementation is part of the Health-Facility based Nutrition Programme of the Integrated Nutrition Programme (INP) and, finally, nutrition education is aimed at changing behaviours that may contribute to poor food choices (DoH 1998).
Many factors influence children's eating behaviour and, consequently, their dietary intake. Story, Neumark-Sztainer & French (2002) identified lifestyle, biological and psychological factors as being some of these influences. Because of changes in their lifestyle, development, social activities and sometimes the environment, dietary quality declines from childhood to adolescence, resulting in a higher intake of soft drinks and fast food and a decrease in fruit and vegetable intake. Poor dietary practices can have long-term implications on health and result in malnutrition, as indicated earlier. Malnutrition can affect growth and sexual development; and results in iron deficiency, obesity, underweight, poor bone health and dental caries (Wenhold et al. 2008:443). Menus in residential care settings provide the framework for nutritious meals that are essential to child health and growth as well as to the development of healthy eating habits (Romaine et al. 2007). Eating behaviour is also influenced in a social setting through reinforcement, modelling, social support and perceived norms (Story et al. 2002). In a residential care setting, various steps can be implemented in order to make mealtimes a positive experience for children and adolescents, thus encouraging the learning of healthy eating habits. Firstly, children learn from good examples, so CCWs should demonstrate good habits; secondly, children who feel stressed, unsafe or anxious do not eat well, so mealtimes should be kept relaxed; and thirdly, it is recommended that children should be involved in menu planning, preparation and serving where possible as this contributes to the development of good habits (Harrison & Crocker 2011:7).
Problem statement
According to the WHO (2013), child nutrition, particularly for vulnerable populations, must be given higher priority in national development, as the unsatisfactory progress from 1990 to 2011 is inadequate for the purposes of meeting the 2015 Millennium Development Goals target. This situation will deteriorate further because the current global economic turmoil has resulted in higher food prices (WHO 2013). Improving nutrition requires an integrated approach to healthcare. Nutrition education and the transfer of relevant knowledge and skills to individuals involved in caring for at-risk children, using appropriate communication strategies, will greatly enhance the quality of life of these children (Egal & Valstar 2007). In order to achieve excellent health and an optimal nutritional status, individuals need sufficient knowledge and skills which would enable them to grow, purchase, process, prepare and eat a variety of foods in the right quantities and combinations (WHO and FAO 2006).
However, before planning a successful nutrition intervention programme to address nutrition problems, it is critical to assess the extent of the existing nutrition problems in a population (Matji 2008:841). A recent study in similar residential care settings established that the large portion sizes of certain food items and the low nutritional quality and inadequacy of the menus need to be addressed. The study found that the average portion sizes of starchy foods were three times larger than recommended (334.70 g per day) and the average portion sizes of fruit and vegetables were small (40 g per day) when compared with the WHO recommendation of > 400 g per day (Grobbelaar, Napier & Oldewage-Theron 2013:35). As already stated, nutrition education material exists and training is provided for CCWs, however it was reported by the management of the various establishments that it is not compulsory for the CCWs to attend these training courses. The effectiveness of the training was not tested for the purpose of this study as only a few CCWs had attended these courses thus far. For this reason, it is evident that exceptional measures are needed in order to ensure the sufficient development of these social service professionals to allow them to respond effectively to the needs of the children in their care.
Aim and objectives of the study
The purpose of this study was to investigate the profile, nutrition knowledge, food safety and hygiene practices of child and youth care workers in residential care settings in Durban in order to guide the development of a food preparation and nutrition manual. The specific objectives were to: (1) determine the demographic profile of the CCWs; (2) establish the current nutrition knowledge; (3) determine the current food safety and hygiene practices; and (4) make recommendations for inclusion in a manual.
The results reported in this article form part of a larger study investigating the food safety and hygiene practices of CCWs in residential care settings
Significance of the study
The information generated will contribute to a better understanding of the factors to be considered in the nutritional management of children in residential care. Moreover, it will provide insight into the issues that need to be addressed in a food preparation and nutrition manual that is developed specifically for CCWs in residential care and other similar settings.
Definition of key concepts
Child and youth care workers: Social service professionals working with and caring for children at risk.
Residential care: Facilities concerned with children who are 'in need of care'.
Adolescents and children: 'Adolescents' are defined as persons aged 10-19 (WHO 2008) and 'children' are, according to the United Nations Convention on the Rights of the Child of 1989 (UNICEF 1989), defined as all individuals below 18 years of age.
Research method and design
Design
A descriptive quantitative design was used. Descriptive studies are useful in that they provide evidence to guide the development of appropriate services, allocate resources and decide on priorities for certain populations (Morroni & Myer 2008:78).
Setting
All the residential care settings (n = 3) managed by a welfare organisation in Durban were included in this study. These homes are officially registered with the Department of Social Development as children's homes in terms of the Child Care Act 74 of 1983 (South Africa 1983). The study population included all the CCWs employed on a permanent or part-time basis.
Each children's home consists of several houses in which up to 15 children can reside. Child and youth care workers are assigned to the houses and they work shifts to ensure that one official is on duty at a time per house. The duties of the CCWs include supervising homework and social activities, as well as preparation and service of meals according to a cycle menu. Children are assigned tasks requiring them to assist in the day-to-day running of each house, including the preparation of meals.
Sampling
Convenience purposive sampling of the CCWs was undertaken. All the CCWs employed during the study period were invited to participate, but participation was voluntary. The CCWs were approached in a group setting during a weekly meeting by the principle investigator. The study was explained and time was given for questioning after which they were requested to participate in the study. Each CCW signed a letter of consent regarding their participation. Forty CCWs agreed to participate and were thus included in the study.
Data collection methods
Data collection was done during 2009. A structured self-administered questionnaire, developed and tested for this purpose, was used to gather the information. The decision to develop rather than use an existing questionnaire was based on factors such as the knowledge of the child care workers, the length of the test (i.e. the test should not be too time consuming to complete) and the familiarity of the food items included (e.g. the use of pilchards on the menu). Some questions were taken from existing questionnaires, for example, from the nutrition knowledge questionnaire validated by the Medical Research Council (Whati et al. 2005) and a nutrition knowledge questionnaire validated in the United Kingdom (Parmenter & Wardle 1999). Questions were also formulated after studying the menus, observing practices in the children's homes and a study of the literature. The questionnaire was reviewed by a dietician for content and face validity. It was also administered to a sample group in order to evaluate the internal consistency by establishing Cronbach's α values. The test-retest reliability was determined by administering the questionnaire to both a knowledgeable and a non-knowledgeable group and establishing Pearson's correlation coefficient.
The questionnaire was divided into two main sections: namely, section A: demographic data of the CCWs; and section B: the awareness of the South African Food Based Dietary Guidelines (SAFBDGs) and knowledge of food sources relating to these guidelines and food safety and hygiene practices. Forty CCWs from the three facilities completed the questionnaires.
General practices during meal preparation and service were observed but not recorded.
Data analysis
The data on the completed questionnaires were captured on a Microsoft® Excel 2010 spreadsheet by the researcher. The data were then analysed with the assistance of a statistician for descriptive statistics (frequencies) using the Statistical Package for Social Sciences (SPSS) version 17.0 (2008; IBM Software). Tables were drawn representing the percentages of the variables included on the questionnaire.
Results
Demographic description of the study group
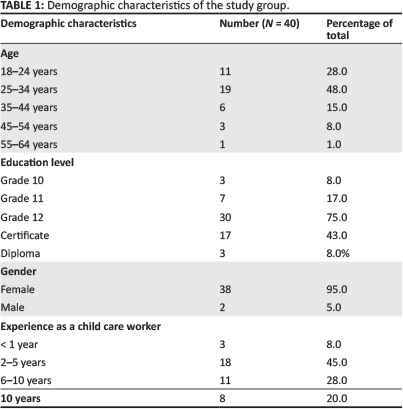
A total of 40 CCWs participated in the study and 95% (n = 38) were women. The majority (n = 30; 76%) were aged between 18 and 34 years. Very few (n = 3; 8%) had completed a Diploma in Child and Residential Care, whilst 43% (n = 17) had completed short courses offered by the NACCW during their employment at the children's homes. Of the 40 CCWs, 75% (n = 30) had completed Grade 12, 17% (n = 7) Grade 11 and 8% (n = 3) Grade 10. The years of experience working as a child and youth care worker ranged from < 1 year (n = 3; 8%) to > 10 years (n = 8; 20%). A large percentage of the respondents (n = 18; 45%) had experience of two to five years and 28% (n = 11) had worked as a child and youth care worker for 6-10 years (Table 1).
Nutrition knowledge of the child and youth care workers
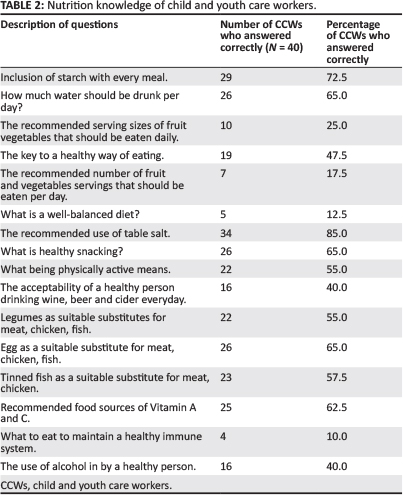
Table 2 presents the summary of results pertaining to the knowledge of the CCWs with regard to the SAFBDGs. The majority of the respondents (n = 29; 72.5%) knew that starchy foods should form part of every meal and could identify correctly the main sources of carbohydrates. Sixty-five percent (n = 26) were aware of how many glasses of water should be drunk per day. A minority of the respondents (n = 10; 25%) could identify the correct serving size for vegetables and very few (n = 7; 17.5%) knew how many portions of fruit and vegetables should be eaten daily. The concept of a well-balanced diet was only known by 12.5% (n = 5), whereas 47.5% (n = 19) knew that a variety of foods should be included in the diet. Fifty-five percent (n = 22; 55%) of the respondents were aware of the importance of physical activity and how it fits into a healthy lifestyle. A minority (n = 16; 40%) knew about the guidelines on the use of alcohol by a healthy person. Only 10% (n = 4) of the respondents could answer the question, 'what should you eat for a healthy immune system?' correctly. Only half of the respondents knew about legumes (n = 22; 55%) and tinned fish (n = 23; 57.5%) as being protein food sources which are suitable substitutes for meat, chicken, fish and poultry.
Food safety and hygiene practices
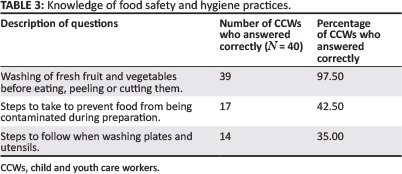
The majority of the respondents were aware of acceptable practices as 97.5% (n = 39) indicated that fruit and vegetables should be washed prior to being eaten, peeled or cut. Nevertheless, only 42.5% (n = 17) knew the steps to be taken to prevent cross-contamination during food preparation and only 35% (n = 14) could identify the correct procedures for washing crockery and cutlery (Table 3).
Ethical considerations
This study was approved as a level 1 ethical impact study by the Faculty of Applied Sciences research committee of the Durban University of Technology. Participants in this study included all the CCWs from the randomly-selected residential care facilities. Participation was voluntary and anonymous; no names were requested on the questionnaire and written consent was obtained from the participants. Written permission was obtained from the Senior Manager: Residential Services of the particular establishments.
Validity and reliability
The final questionnaire was self-administered during a meeting called by the researcher as the respondents (N=40) could read and write and were familiar with answering questions. Care was taken during the implementation of the questionnaire in order to prevent the respondents from influencing each other. This was done by instructing the respondents not to speak to each other, as well as positioning chairs and tables some distance away from each other, all facing the same direction as if writing a test. The researcher was present throughout the questionnaire completion session.
Discussion
This study aimed to investigate the profile, nutrition knowledge, food safety and hygiene practices of child and youth care workers in residential care settings in order to guide the development of a food preparation and nutrition manual. The study highlighted various areas for improvement and the results provided useful information for inclusion into a manual that will be specifically customised to the CCWs in order to respond to the needs of the children.
Very few of the CCWs had a tertiary or any other qualification. Employment periods at the children's homes ranged from < 1 to > 1 0 years, during which time some of the CCWs attended short courses offered by the NACCW. Theory on basic nutritional concepts and menu planning are included in one unit standard of these courses, but no practical application of the theory is done. The duration of this unit standard is four to six hours and it includes other basic caring skills for children and youth at risk. Most of the CCWs rely on the training provided by the children's homes and experience gained during employment to care for the children.
Various studies from Canada and the United States of America indicate that even though CCWs seem to be well educated, with 60% - 70% having a post-secondary school education, 16% - 36% community college training, 14% -22% university qualifications and 9% - 18% with Childhood Development diplomas (Burden et al. 2000; Lero et al. 1999; Nahikian-Nelms 1997)
Only 50% of menu planners in a sample of 101 child care facilities in the United States (USA) indicated that they received training in menu planning and at least 50% of these reported that this had occurred more than six years before the date of the study (Romaine et al. 2007). The American Dietetic Association recommends that CCWs should receive child nutrition training on an annual basis (Briley & Roberts-Gray 1999).
Research has confirmed that nutrition knowledge is an important indicator of dietary intakes and adequate nutrition knowledge is imperative with regard to the improvement of dietary intake habits (Hendrie, Cox & Coveney 2008). Above all, the CCWs are tasked with the healthcare of at-risk children. The purpose of healthcare is to assist children to live a healthy and good life and nutrition plays a very important part (Food and Nutrition Technical Assistance [FANTA] 2008). In addition, the accredited training provided by NACCW includes approximately four hours of basic nutrition education and no practical training (NACCW 2011).
Although it is evident from the results that the respondents' knowledge was fair on general nutrition guidelines, there are areas for improvement. Firstly, knowledge on the importance of a variety in the diet is lacking. Secondly, the results indicate a very poor knowledge of the recommended number of fruit and vegetable portions per day, as well as correct serving sizes. Thirdly, a very poor knowledge exists regarding the role of healthy eating in maintaining and supporting the immune system; and finally, the respondents lacked knowledge in the area of the use of alcohol by healthy individuals. In a study in the USA investigating the nutrition knowledge and attitudes amongst caregivers in 24 child care programmes, it was found that the group's overall nutrition knowledge was low as less than 50% answered 10 of the 20 questions correctly. Many were also unable to identify the best sources of protein (Nahikian-Nelms 1997:506). These results are consistent with the results of this study as only 45% of the CCWs scored 50% or more in the questionnaire. Many of the caregivers in the USA study were also unable to identify the best sources of protein, which compares with the results of this study. Just over half of the CCWs knew that tinned fish (57%) and legumes (55%) can be used in place of meat.
In a study by Grobbelaar et al. (2011), investigating the dietary intake of the children in the same residential care settings, it was found that the average portion sizes of starch served (established through a plate-waste study) were large (250 g -350 g), resulting in the children consuming three times more carbohydrates per day than the recommended intake. This investigation also highlighted the small portions of vegetables served to the children during meal times (an average serving size of 40 g) and the absence of adequate fruit and vegetables on the menu for breakfast and lunch. Although the children's energy intake was adequate, none of the age groups met the Dietary Recommended Intakes (DRIs) for fibre, calcium and iodine. Micronutrient inadequacies were more prevalent in the dietary intake of age groups 9-13 and 14-18 years in both girls and boys (Grobbelaar et al. 2013:35). This could be because of the lack of nutrition knowledge in the CCWs as reflected in this article.
A limited knowledge regarding correct hygiene practices was noted. Although the data indicated that the majority of the CCWs were aware of the correct handling of fruit and vegetables, this was not, however, the case in practice. The researcher observed that fresh fruit and vegetables were not always washed prior to use. The results also showed that the CCWs lacked knowledge on steps to prevent food contamination and had a very poor knowledge on the correct procedures for washing plates and utensils. Access to appropriate cleaning materials was limited. These results are consistent with the findings of a study in the North Eastern USA indicating that only 55% of managers in residential care settings met the proficiency standards of food safety practices for cooked and/or prepared food (Pivarnik et al. 2012:296). It is known that poor hygiene practices can result in unsafe food that can result in diarrhoea and, ultimately, contribute to malnutrition as a result of food-borne diseases (Egal & Valstar 2007; FANTA 2008).
Limitations of the study
The small convenient sample is not representative of the total population, which may limit the generalisation of the results. Informal observation on its own did not measure food safety and hygiene practices adequately and it is recommended that structured interviews be combined with informal observation in order to yield more detailed results. As a result of a paucity of recent literature and studies in residential care facilities, specifically in South Africa, limited comparisons could be drawn to the results of this article.
Conclusion and recommendations
The significance of this study is that it is one of the first studies that reports on the nutrition knowledge and food safety and hygiene practices of child and youth care workers in residential care settings in South Africa.
The overall findings support the development of a comprehensive food preparation and nutrition manual. The manual should address relevant nutrition education including meal and menu planning, food safety and hygiene practices and practical food preparation skills. The manual should increase self-efficacy of the CCWs for planning and preparing healthy menus and meals for the children in their care.
Investing in the development of the ability to plan and prepare nutritious meals of those working directly with at-risk children, will vastly improve the quality of services provided.
A further study on food safety and hygiene practices in these establishments is recommended in order to gain a better understanding of these practices and to develop a manual that also includes safety and hygiene.
Acknowledgements
We thank all the child and youth care workers who participated in the study and the residential care facilities for allowing us to conduct the study. In addition, we would like to acknowledge Professor Wilna Oldewage-Theron for her co-supervision of the research.
Competing interests
The authors declare that they have no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
Authors' contributions
C.E.N. (Durban University of Technology) was the study leader and was involved in compiling and editing the manuscript. H.H.G. (Durban University of Technology) compiled and wrote the manuscript and searched for reference material. Both authors read and approved the final article.
References
Briley, M.E. & Roberts-Gray, C., 1999, 'Position of the American Dietetic Association: Nutrition standards for child-care programs', Journal of the American Dietetic Association 99(8), 981-988. http://dx.doi.org/10.1016/S0002-8223(99)00235-7 [ Links ]
Burden, T., Sheeshka, J., Hedley, M., Lero, D.S. & Marsh, S., 2000, 'Development, implementation and evaluation of a nutrition education program for informal (unlicensed) child caregivers', Journal of Nutrition Education 32(2), 104-110. http://dx.doi.org/10.1016/S0022-3182(00)70527-9 [ Links ]
Department of Health, 1998, Integrated nutrition programme for South Africa. Draft 5. Broad guidelines for implementation, Department of Health, Pretoria. [ Links ]
Egal, F. & Valstar, A., 2007, HIV/AIDS and nutrition: helping families and communities to cope, viewed 04 July 2013, from http://www.fao.org/docrep/X4390T/X4390T04.HTM [ Links ]
Food and Nutrition Technical Assistance (FANTA), 2008, Guide to monitoring and evaluation of nutrition assessment, education and counselling of people living with HIV, FANTA, AED, Washington, DC. [ Links ]
Ganyaza-Twalo, T. & Viviers, A., 2012, Report on the National Council of Provinces Child Rights Seminar: Investing in children, Parliament of the Republic of South Africa, Cape Town. [ Links ]
Grobbelaar, H., Napier, C. & Oldewage-Theron, W., 2013, 'Nutritional status and food intake data on children and adolescents in residential care facilities in Durban', The South African Journal of Clinical Nutrition 26(1), 29-36. [ Links ]
Harrison, C. & Crocker, S., 2011, Healthy eating matters: Food and nutrition toolkit for residential care settings, Ministry of Children and Youth Services, Ontario. [ Links ]
Hendrie, G., Cox, D. & Coveney, J., 2008, 'Nutrition knowledge as a predictor of nutrient intake and dietary quality', Journal of Nutrition Education and Behavior 40(4), S49-S50. http://dx.doi.org/10.1016Zj.jneb.2008.03.077 [ Links ]
Human Sciences Research Council (HSRC), 2013, Nutritional status of children - Media Release No. 2, Cape Town, South Africa. [ Links ]
Labadarios, D., Swart, R., Maunder, E.M.W., Kruger, H.S., Gericke, G.J., Kuzwayo, P.M.N. et al., 2008, 'Executive summary of the National Food Consumption Survey Fortification Baseline (NFCS-FB-I) South Africa, 2005', South African Journal of Clinical Nutrition 21(3), 245-300. [ Links ]
Lero, D.S., Sheeshka, J.D., Burden, T.J. & Crocker, S., 1999, 'What do informal (unlicensed) child caregivers want and need to know about nutrition: A needs assessment', The Canadian Journal of Research in Early Childhood Education 7(4), 329-338. [ Links ]
Manary, M.J. & Solomons, N.W., 2004, 'Public health aspects of undernutrition' in M.J. Gibney, B.M. Margetts, J.M. Kearney & L. Arab, (eds.), Public Health Nutrition, pp. 178-191, Wiley-Blackwell, Oxford. [ Links ]
Matji, J., 2008, 'Assessment and analyses of community nutrition problems' in N.P. Steyn & N. Temple (eds.), Community nutrition textbook for South Africa: A rights-based approach, pp. 837-846, South African Medical Research Council, Tygerberg. [ Links ]
Meintjies, H., Leatt, A. & Berry, L., 2006, 'Demography of South Africa's children', in Monson, J., Hall, K., Smith, C. & Shung-King, M. (eds.), South African Child Gauge 2006, pp. 67-69, Children's Institute, University of Cape Town, Cape Town. [ Links ]
Meintjies, H., Moses, S., Berry, L. & Mampane, R., 2007, 'Home truths: The phenomenon of residential care for children in a time of AIDS', Children's Institute, University of Cape Town and Centre for the Study of AIDS, University of Pretoria. [ Links ]
Morroni, C. & Myer, L., 2008, 'Study design' in G. Joubert & R. Ehrlich (eds.), Epidemiology: A research manual for South Africa, pp. 77-93, Oxford University Press, Cape Town . [ Links ]
Nahikian-Nelms, M., 1997, 'Influential factors of caregiver behavior at mealtime: A study of 24 child-care programs', Journal of the American Dietetic Association 97(5), 505-509. http://dx.doi.org/10.1016/S0002-8223(97)00130-2 [ Links ]
National Association of Child Care Workers (NACCW), 2011, About us, viewed 04 July 2013, from http://www.naccw.org.za/about/index.html [ Links ]
Parmenter, K. & Wardle, J., 1999, 'Development of a general nutrition knowledge questionnaire for adults', European Journal of Clinical Nutrition 53(4), 298-308. http://dx.doi.org/10.1038/sj.ejcn.1600726 [ Links ]
Pivarnik, L.F., Richard, N.L., Patnoad, M.S. & Gable, R.K. 2012, 'Assessment of food safety knowledge and attitudes of managers of residential childcare institutions (RCCI) in the Northeast', Food Protection Trends 32(6), 296-308. [ Links ]
Romaine, N., Mann, L., Kienapple, K. & Conrad, B., 2007, 'Menu planning for childcare centres: practices and needs', Canadian Journal of Dietetic Practice and Research 68(1), 7-13. http://dx.doi.org/10.3148/68.1.2007.7 [ Links ]
South Africa, 1983, Child Care Act 74 of 1983, Government Printer, Pretoria. [ Links ]
South Africa, 2007, Children's Amendment Act 41 of 2007, Government Printer, Pretoria. [ Links ]
Story, M., Neumark-Sztainer, D. & French, S., 2002, 'Individual and environmental influences on adolescent eating behaviors', Journal of the American Dietetic Association 102(3 Suppl.), S40-S51. http://dx.doi.org/10.1016/S0002-8223(02)90421-9 [ Links ]
UNICEF, 1989, Understanding the Convention on the Rights of the Child, viewed 04 July 2013, from http://www.unicef.org/crc/index_understanding.html [ Links ]
UNICEF, 2009, Children and AIDS - fourth stocktaking report, viewed 04 July 2013, from http://www.unicef.org/publications/flles/Children_and_AIDS_Fourth_Stocktaking_Report_EN_120209.pdf [ Links ]
Vorster, H.H., 2009, 'Introduction to human nutrition: A global perspective on food and nutrition' in M.J. Gibney, S.A. Lanham, A. Cassidy & H.H. Vorster (eds.), Introduction to human nutrition, 2nd edn., pp. 1-11, Wiley-Blackwell, Oxford. [ Links ]
Wenhold, F., Kruger, S. & Muehlhoff, E., 2008, 'Nutrition for school-age children and adolescents' in N.P. Steyn & N. Templ (eds.), Community nutrition textbook for South Africa: a rights-based approach, pp. 441-478, South African Medical Research Council, Tygerberg. [ Links ]
Whati, L.H., Senekal, M., Steyn, N.P., Nel, J.H., Lombard, C. & Norris, S., 2005, 'Development of a reliable and valid nutrition knowledge questionnaire for urban South African adolescents', Nutrition 21(1), 76-85. http://dx.doi.org/10.1016/j.nut.2004.09.011 [ Links ]
Witten, C., Jooste, P., Sanders, D. & Chopra, M., 2003, Micronutrient programs in South Africa, viewed 18 April 2014, from http://www.idpas.org/pdf/2553_SouthAfrica.pdf [ Links ]
World Health Organization (WHO), 2002, The World Health Report 2002 - reducing risks, promoting healthy life, viewed 04 July 2013, from http://www.who.int/whr/2002/en.pdf [ Links ]
World Health Organization (WHO), 2008, 'Training course on child growth assessment, WHO child growth standards - Interpreting Growth Standards', WHO, Geneva. [ Links ]
World Health Organization (WHO), 2013, World Health Statistics, WHO, Geneva. [ Links ]
World Health Organization (WHO) and Food and Agricultural Organization of the United Nations (FAO), 2006, 'Guidelines on food fortification with micronutrients', viewed 04 July 2013, from http://www.who.int/nutrition/publications/guide_food_fortification_micronutrients.pdf [ Links ]
 Correspondence:
Correspondence:
Hendrina Grobbelaar
PO Box 1334
Durban 4000
South Africa
heleeng@dut.ac.za
Received: 23 Aug. 2013
Accepted: 04 Apr. 2014
Published: 06 Aug. 2014

