










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkHealth SA Gesondheid (Online)
versión On-line ISSN 2071-9736
versión impresa ISSN 1025-9848
Health SA Gesondheid (Online) vol.18 no.1 Cape Town oct. 2013
ORIGINAL RESEARCH
Factors influencing the quality of patient data captured by nurses for the tuberculosis control programme in Oshakati District, Namibia
Linda V. KagasiI; Lindiwe ZunguI; Muhammad E. HoqueII
IDepartment of Health Studies, University of South Africa, South Africa
IIDepartment of Public Health, University of Limpopo, South Africa
ABSTRACT
Effective tuberculosis control relies heavily upon the general health system of the country, particularly on well-functioning primary healthcare services. This study investigated factors influencing the quality of data for the tuberculosis control programme in Oshakati district in Namibia. A quantitative, contextual, cross-sectional descriptive survey was conducted using 50 nursing personnel of different cadres who were sampled from five departments in Oshakati State Hospital. Data was collected by means of a self-administered questionnaire. Most participants reported that tuberculosis-related training improved correct recording and reporting amongst nursing personnel, which is a requirement for a quality tuberculosis control programme. The number of documents to be completed for each patient influences the quality of data recording and completeness. Factors such as the lack of resources and of adequate training as well as knowledge of tuberculosis control guidelines, in particular the use of records to capture the core tuberculosis indicators, influence the quality of data in the tuberculosis control programme. Knowledge, attitudes and practice are the main factors influencing the quality of data in the tuberculosis control programme in Oshakati district.
OPSOMMING
Die effektiewe beheer van tuberkulose steun grootliks op die algemene gesondheidstelsel van 'n land, veral op die goeie werkende primêre gesondheidsorgdienste. Die studie het faktore wat die gehalte van data vir die teringbeheerprogram in die Oshakati Distrik in Namibië ondersoek.'n Kwantitatiewe, kontekstuele, kruisseksionele, beskrywende opname was onderneem met 'n steekproef van 50 verpleegpersoneel van verskillende kadres uit vyf departemente in Oshakati Staatshospitaal. Data was deur middel van 'n selftoegediende vraelys ingewin. Die meeste deelnemers het genoem dat teringverwante opleiding die korrekte afneem en rapportering onder verpleegpersoneel verbeter het, wat 'n vereiste is vir 'n gehalte teringbeheerprogram. Die aantal dokumente wat vir elke pasiënt voltooi moet word, beïnvloed die gehalte van data-aantekening en volledigheid. 'n Tekort aan bronne en gepaste opleiding, en kennis van tering-beheerriglyne, veral die gebruik van teringrekords om die kern teringaanwysers op te neem, was ander belangrike faktore wat die gehalte van data in die teringbeheerprogram beïnvloed het. Kennis, houdings en praktyk is die vernaamste faktore wat die gehalte van data in die program in die Oshakati Distrik beinvloed.
Introduction
Tuberculosis (TB) remains a major cause of morbidity and mortality in many countries and is a significant health problem worldwide (World Health Organization [WHO] 2008a:3). In 2005, the WHO reported that the global incidence of TB was estimated to be 136 cases per 100 000 people per year (WHO 2008a:3). The burden of TB in Namibia was reported to be 765 cases per 100 000 of the population in 2006 and 2007 (Ministry of Health and Social Services [MoHSS] 2008:6). This is reported to be the second-highest Case Notification Rate in the world after Swaziland (MoHSS 2008:6). The WHO targets for tuberculosis control by 2015 include 100% direct observed therapy short-course (DOTS) coverage, 70% case detection and 85% treatment success rates (WHO 2006:6).
In 2010, an estimated 8.8 million new cases of TB were reported worldwide, with over 1 million TB deaths (WHO 2011). South Africa is ranked as having the third-highest TB incidence after China and India, with a TB incidence of 971 per 100 000 compared with the global average of 137 per 100 000 in 2009 (WHO 2010).
Effective TB control relies heavily upon the general health system of the country, in particular well-functioning primary healthcare (PHC) services. They contribute substantially to strengthening the health systems, which include the direct observed therapy (DOT) strategies (WHO 2006). Furthermore in trying to control the incidence of TB, the WHO developed the 'Stop TB Strategy' which comprises the following components: (1) Pursuing high-quality DOT expansion and enhancement; (2) Addressing TB/HIV, multiple drug resistance TB (MDR-TB) and other challenges; (3) Contributing to health system strengthening, engaging all health care providers, empowering individuals, groups and communities with TB awareness and control information; and (4) Enabling and promoting operational research related to TB control (WHO 2008a:8).
In healthcare settings the quality of data is viewed as a continuous process, as opposed to a one-time activity. This is exhibited in the literature reviewed for this study which concurs with the definition provided in Tomey (2000:382), namely that continuous quality improvement is a preventive, problem-solving process which results in effective and efficient service. Green and Bowie (2005:246) emphasise that the characteristics of accessibility, accuracy, comprehensiveness, comprehension consistency, definition, granularity, precision, relevance and data timeliness are important in ensuring data quality.
One of the attributes of reliable and valid data is its completeness. According to a study in the United Kingdom, complete data allow governments to be reassured concerning full disclosure of outcomes by the centre of origins, thus assisting in the process of validation, monitoring and feedback geared toward improving data quality (Fine et al. 2003:25).
The advent of the Electronic Tuberculosis Register in data collection relies on data-collection tools at health facilities which significantly influence the quality of data, including the completeness of data collected. But capturing of the data relies on the person that enters the data into the system, rather than the tools, so the data capturers need to be motivated in order to capture the data correctly and comprehensively. The experience in Botswana in this regard highlights problems in the paper-based TB data collection system (Vranken et al. 2002:112).
In Namibia, the Ministry of Health TB guidelines clearly describe the flow of data from the facility level up to the district level, whilst various reporting forms are illustrated clearly. However, the guidelines do not provide details regarding data-verification processes, timeliness as regards the information reaching the various management levels, the frequency of feedback to evaluate the achievements of the programme and gaps identified during supervisory visits (MoHSS 2006:50).
To date, the country has achieved coverage of 100%, hence all public health facilities are implementing the DOT strategy as part of the National TB control programme. At the district level, the district TB register and the electronic tuberculosis register are the core data-collection tools available (MoHSS 2006:50). At the facility level, the nurse's main function in the TB programme is to enter data and ensure that data quality is maintained as well as to report monthly to the district TB coordinators on the caseloads in the facility and other treatment outcomes as stipulated in the TB guidelines (MoHSS 2006:50).
A total of 12 zonal review meetings have been held, with the last being held in the Omusati region in January 2009 (MoHSS 2009:10). The information shared in these meetings is district based, not facility based. According to the twelfth review meeting, aspects of ensuring data quality were not incorporated in detail in the presentations by each district. However, one aspect of data quality highlighted by Oshakati district during this meeting revealed that data on the MDR situation was not available for assessment of the progress achieved during the reporting quarter (MoHSS 2009:10).
Problem statement
The burden of TB in Namibia was reported to be 765 per 100 000 people in the 2006 and 2007 annual report (MoHSS 2008a:6). Obtaining quality data involves the recording and reporting of existing, newly-diagnosed and known TB cases. This fulfils a key role in the strengthening of health systems and in improving the quality of data collected, which is useful in the monitoring and evaluation of programme performance. This is supported by the WHO Stop TB Strategy (WHO 2006:11) which emphasises the need for reliable data that support monitoring and evaluating the performance of strategies in TB control.
There is limited information documented on the steps taken to ensure data quality in the TB control programme in Namibia, particularly in Oshakati district where the prevalence of TB is high. This is evidenced by the health reports presented during the quarterly review meetings by the Ministry of Health (MoHSS 2009:10). This study therefore addressed factors that influenced the quality of data for TB control management which plays a crucial role in assessing treatment outcomes, in early identification of programme needs as well as in identifying gaps in TB management programmes.
Purpose of the study
The purpose of the study was to identify factors that influence the quality of data for the Tuberculosis (TB) control programme in Oshakati district in Namibia.
Trends
According to the Stop TB Strategy by the WHO, poor quality vital statistics and demographic information, lack of data on patterns of healthcare utilisation, weaknesses in the surveillance system and poor disease-notification systems were identified as major factors influencing the quality of data and that affect the control and management of TB programmes (WHO 2008b:1). This is as a result of the quality of data collected in the health system as well as data collected specifically in the TB programmes (WHO 2008b:2). Quality improvement and timely dissemination of quality data are essential in assisting health authorities at all levels to make effective decisions with regard to disease control. Similarly, the success of the Stop TB Strategy depends on reliable recording and reporting systems of TB surveillance that provide effective information and report on the components of assessing the TB control and management programme (Nadol et al. 2008:58).
Contribution to the field
This study investigated the factors that influenced the quality of data in the TB control programme. The results of the survey will assist in programme planning at all health operational levels as a basis for TB control and management, specifically the monitoring and evaluation component. It would assist in the development of monitoring and evaluation tools and revision of existing TB guidelines. It would further improve the data-collection tools that are currently being used, assist in revising related health policies and integrate the existing health systems for efficiency and effectiveness. Lastly, the information is intended to contribute to strengthening data collection practices geared toward the strengthening of TB control and management efforts in Oshakati district.
Research design and method
Design and setting
A descriptive contextual cross-sectional design based on a quantitative approach was used for this study in order to identify and describe factors that influenced data quality for the TB control programme in Oshakati district, Namibia. According to Polit and Beck (2006:504), cross-sectional studies are appropriate for describing relationships amongst phenomena occurring at a fixed point in time.
The study was conducted at Oshakati State Hospital, Namibia. According to the current Oshakati district structure (MoHSS 2008:6), the hospital is responsible for all of the health services in the district; this includes both the clinical and primary healthcare services. The clinical services are provided by the Oshakati State Hospital and the clinical personnel comprise doctors, registered nurses and enrolled nurses. Oshakati district lacks a district hospital, as do other districts, as the State Hospital is one of the three intermediate hospitals in the country. Oshakati district was chosen as a study setting as it houses one of the intermediate hospitals, the Oshakati State Hospital. This institution serves the four north central regions, which are the highest populated regions, in Namibia (National Planning Commission 1997:22).
Population
The population for this study comprised the different cadres of nurses (registered, enrolled and student nurses) working at the Oshakati State Hospital. A total of 101 nurses worked in the hospital at the time that the study was conducted.
The Oshakati State Hospital makes use of a staff establishment document that lists all the staff currently working in the hospital according to their various departments and nursing cadre. This was consulted during this study.
Sample size and sampling technique
The sample size was chosen at a ratio of 2:1, which means two nurses from the morning and afternoon shifts and one nurse from the night shift. This took into consideration the three shifts that nurses work in three out of the six targeted departments (i.e. morning, afternoon and night shifts). According to Polit and Hungler's guidelines (1999:489), the researchers chose the most effective sample size (55) that would demonstrate the relationship statistically.
In this study, multi-stage sampling techniques were used to select the study subjects. First of all, different departments were considered as 'strata'. Next, from within each stratum, nursing personnel were stratified according to the nursing cadre that they belonged to. Finally, a random sampling method (by means of computer-generated random numbers) was used to select the samples from each department using the nursing staff database obtained from the nurse manager of each unit. The inclusion criteria for this study included all nursing staff from the different departments, namely, the TB clinic, the TB ward, the HIV clinic and the medical wards for both male and female patients. These departments were chosen as they were the points where most of the TB diagnoses in the hospital were made.
It should be noted that the study was conducted at a time when the student nurses had completed their final examination for the year and were completing their clinical training. According to the unit nurse managers, the final-year student nurses were able to complete the documents and patients' records with minimal supervision.
Data collection methods
Data collection was conducted at the study site between July and November 2009. A self-administered questionnaire that consisted of both closed- and open-ended questions was used to collect information from the participants on the factors influencing the quality of data for the TB control programme at Oshakati district in Namibia. The data-collection tool was divided in two main parts and the first part collected participants' demographic characteristics. The second part gathered data that described factors that influenced data quality for TB control at Oshakati State Hospital. This section was limited to three variables and divided into three subsections, which included factors relating to the participants' knowledge, attitude and practice, all of which influenced the quality of data in the TB programme in Oshakati district. A return box for all completed questionnaires was placed in each sampled department at the nurse managers' offices and was emptied by the researcher on alternate days.
Data analysis
Data were entered into a Microsoft Excel 2003 spreadsheet and imported to the Statistical Package for Social Sciences (SPSS version 18.0) for data analysis. The participants' sociodemographic variables and factors influencing data quality for the TB control programme at the study site were summarised using descriptive summary measures, expressed as mean (standard deviation) for continuous variables and percentage for categorical variables.
Ethical considerations
Ethical approval to conduct the study was obtained from the Research Ethics Committee of the Department of Health Studies at the University of South Africa (Project no: 3732-496-9). Permission to conduct the study was obtained from the Ministry of Health in Namibia as well as from the relevant authorities at Oshakati State Hospital. Written informed consent to participate in the study was obtained from each of the participants prior to distribution of questionnaires. For the purpose of ensuring anonymity of data, participants were requested not to include their personal information. Confidentiality of data obtained was upheld at all time as only the researchers had access to the data collected.
Reliability and validity
The questionnaire was developed by the researchers by the following the knowledge, attitudes, beliefs and practices surveys guidelines recommended by the WHO (WHO 2008b:2). It was also assessed by experts in the field of TB management and was refined accordingly, based on the input received from the experts. The questionnaire was pretested using nurses from a nearby hospital who were also involved in TB control programmes. This was done in order to solicit the clarity and appropriateness of the questionnaire and to make it more user friendly. These measures were done so as to ensure the validity and reliability of the tool.
Discussions of results
A total of 55 nurses was approached to participate in this study and 50 of them gave informed consent, making a response rate of 90.9%.
Participants' sociodemographic data
Table 1 summarises the distribution of the participants' sociodemographic characteristics. The results showed that the majority (84%, n= 42) of the participants were women, compared with a small proportion (16%, n= 8) who were men. Most of them (44%, n= 22) were less than 25 years old, followed by those between the ages of 46-55 years (22%, n= 11).
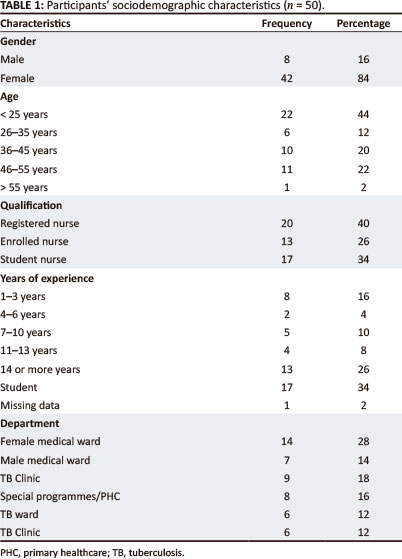
The results revealed that 40% (n= 20) of the participants were registered nurses, followed by student nurses (34%, n= 17) who were in their final year of study and, lastly, enrolled nurses (26%, n= 13). Regarding years of working experience, the highest proportion (26%, n= 13) had worked for 14 years or more, followed by those with less than three years' work experience (16%, n= 8). In terms of departmental representation, the female medical ward had the highest representation (28%, n= 14) compared with the other departments, as is shown in Table 1.
Factors influencing data quality in the programme
Quality of data is an important component in ensuring that that strategies used in monitoring and evaluating programmes that have been implemented are accurate and valid. Good quality information is essential in order to evaluate the magnitude of disease transmission in a country and to determine the nature of health care services and treatment to be provided (Braga 2007:2).
Table 2 shows the participants' views regarding factors influencing the quality of data for the TB control programme in the study site. The results indicated that the majority (90%, n= 45) of the participants reported that receiving training on TB could improve the recording and reporting of data required for TB control, thus enhancing the quality of data captured and reported.
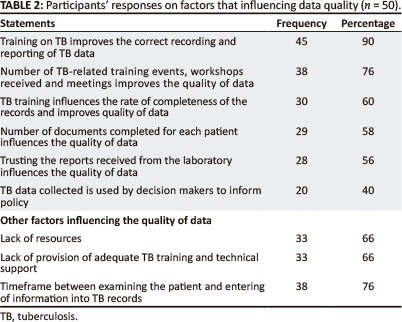
Furthermore, 76% (n= 38) of the participants reported that the amount of TB training received improved the quality of data in the TB control programme. This was further explained by 60% (n= 30) of the participants who reported that the amount of training they received improved both the accuracy and completeness of data recording at the health facility level. Similarly, findings from a Malawian study conducted amongst health care workers (HCWs) on TB training and technical support showed that the number of training sessions attended by HCWs improved the recording of complete information at the facility level (Chaulagai et al. 2005:378). Such findings clearly indicate that the recording of quality data for an effective TB control programme could be achieved through the provision of regular on-the-job training and provision of the necessary technical support for HCWs.
Completion of documents for the programme
As shown in Table 2, more than half (58%, n = 29) of the participants reported that the number of documents to be completed for each patient influenced the quality of data in the TB control programme. On the question of trusting the laboratory reports, 56% (n = 28) of the participants stated that the format of the laboratory reports influenced the quality of data transfer in the TB control programme. Furthermore, the majority (76%, n = 38) of the participants mentioned that the time that they took to conduct physical examinations on patients and thereafter capture the findings of the assessments on the TB registers also influenced the quality of data captured for the TB control programme.
In South Africa, findings from a survey conducted in the Eastern Cape Province revealed that health workers are faced with myriad books and forms used to collect data for managers, but with minimal integration and a lack of vision for the utilisation of this data at the local level. Findings also showed that data collected by clinic staff seemed to be insufficient for adequate management of services rendered (Shaw 2005:633).
Lack of resources and training
Other factors reported by participants that influence the quality of data in TB control programme in Oshakati State hospital included the lack of material and human resources (66%, n = 33) and the lack of provision of adequate TB training (66%, n = 33) for nurses.
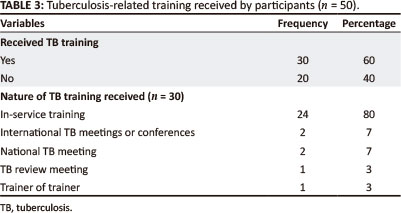
Regarding TB training, participants were asked if they had received any form of on-the-job TB training at Oshakati State hospital. As shown in Table 3, a higher proportion (60%, n = 30) of participants reported that they had received TB training compared with those who indicated that they had not (40%, n = 20). Of those who had received training, the majority (80%, n = 24) reported that they had received in-service training followed by equal numbers (7%, n = 2) of those who mentioned receiving training from international and local meetings or conferences respectively.
A Nigerian study on the training of front-line health workers with regard to TB control revealed that the capabilities and competencies of the health workers largely determine the quality and efficiency of the TB control programme. Thus, efficient human resources development is vital for the purpose of facilitating TB control in developing countries and appropriate training of front-line personnel is an important component of this process (Awofeso, Schelokova & Dalhatu 2008:1). In addition, the WHO Global Plan to Stop TB 20062015 has recognised that the main human resource issue affecting TB control is the lack of health care personnel with the necessary skills to render quality services for TB control programmes (WHO 2006:50, 2008b:2).
Clinical practices influencing the quality of data for the programme
Participants were asked to indicate clinical practices that influenced the quality of data in the TB control programme at Oshakati State hospital. Findings showed that the majority (82%, n = 41) of the participants stated that the turnaround time for sputum pathology results and frequent auditing of TB data (80%, n = 40) are clinical practices that influence the quality of TB data. It is accepted that the quality of laboratory services has a strong influence on the nature and quality of care provided to patients (Awofeso et al. 2008:7) and is an essential component of the TB control programme. This therefore places an increasing demand on the quality (WHO 2003, 2011) and establishment of good laboratory services which include, amongst other things, the ready availability of standard operating procedures (WHO 2011).
Therefore, systematic interventions such as high-quality training for laboratory workers and efficient quality assurance systems must be implemented with a view to improving on the acquisition of accurate, reliable and timely data for a quality TB control programme. In addition, a study conducted by Zurovac et al. (2004:1084) in Kenya showed that an assessment of the roles of laboratories in the effectiveness of TB programmes acknowledged the need for well-trained staff in quality laboratory service management.
As shown in Table 4, other practices reported by the participants which influenced the quality of data included the number of technical supportive supervision sessions provided by regional managers (58%, n= 29) and also technical support provided from the regional level (34%, n= 17).
Conclusion
The findings of this study clearly point out that quality data are essential in order to determine the effectiveness of TB control programmes, identify existing gaps and devise relevant interventions that would improve the quality of TB control services. Hence, the accuracy, validity and completeness of data recorded are crucial, as well as timely reporting which is essential for early treatment and care. In essence, good quality data will serve as a useful tool for robust local, national, and global efforts to control and, eventually, eliminate TB.
Recommendations
The importance of data quality in an effective TB control programme cannot be overemphasised. In line with the findings of this study, interventions recommended to enhance the quality of data include the following:
• Additional user-friendly tools are needed in order to promote the recording and capturing of quality TB data by nurses. It is envisaged that interventions would be reinforced by the number and lucidity of the documents to be completed and by the functionality of record management systems at facility level so that the information needed to support and sustain TB control programmes is captured accurately.
• Regular on-the-job TB training such as capturing information should be provided at an appropriate level for the different cadres of nurses and laboratory workers in order to promote their competence in quality data management which will ultimately improve their daily data recording and capturing practices.
• Availability and adherence to standard laboratory operating procedures is equally important in order to ensure dependable TB laboratory services which will enhance the diagnosis, care and treatment service provision.
• Further research is essential in order to assess the quality and impact of on-the-job TB training provided to nurses at facility level. At the national level, the quality of training can be evaluated by its impact on TB case detection, treatment outcomes and validity of reports from TB control programmes. The latter is particularly significant because the effectiveness of a country's TB control programme is measured by the level of smear-positive pulmonary TB case detection and treatment success rates.
Acknowledgements
Competing interest
The authors declare that they have no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
Author's contributions
L.V.K. (Department of Health Studies, University of South Africa) was the project leader and performed the experiments. L.V.K. and L.Z. (Department of Health Studies, University of South Africa) were responsible for experimental and project design. M.E.H. (Department of Public Health, University of Limpopo) made conceptual contributions and wrote the manuscript. L.V.K. and L.Z. prepared the samples and all calculations were performed by both L.V.K. and M.E.H.
References
Awofeso, N., Schelokova, I. & Dalhatu, A., 2008, 'Training of front-line health workers for tuberculosis control: lessons from Nigeria and Kyrgyzstan', Human Resources for Health 6(20), 1-9. [ Links ]
Braga, J.U., 2007, 'Tuberculosis surveillance and health information system in Brazil, 2001-2003' viewed 21 July 2011, from http://www.scielo.br/pdf/rsp/v41s1/en_6494.pdf [ Links ]
Chaulagai, C.N., Moyo, C.N., Koot, J., Sambakunsi, T.C., Khunga, F.M. & Naphini, P.D., 2005, 'Design and implementation of a health management information system in Malawi: issues, innovation and results' Health Policy and Planning 20(6), 375384. http://dx.doi.org/10.1093/heapol/czi044, PMid:16143590 [ Links ]
Fine, L.G., Keogh, B.E., Cretin, S., Orlando, M. & Gould, M.M., 2003, 'How to evaluate and improve the quality and credibility of an outcomes database: validation and feedback study on the UK cardiac surgery experience', British Medical Journal 326(7379), 25-28. http://dx.doi.org/10.1136/bmj.326.7379.25 [ Links ]
Green, M.A. & Bowie, M.J., 2005, Essentials of health information management: principles and Practices, Cengage Learning, New York. [ Links ]
Ministry of Health and Social Services, 2006, National guidelines for the management of Tuberculosis, 2nd edn., Windhoek. [ Links ]
Ministry of Health and Social Services, 2008, 'National tuberculosis and leprosy control programme, Annual Report 2006/2007', Windhoek. [ Links ]
Ministry of Health and Social Services, 2009, 'The twelfth zonal TB meeting report', Outapi Town Lodge, Omusati. [ Links ]
Nadol, P., Stinson, K.W., Coggin, W., Naicker, M., Wells, C.D., Miller, B., et al., 2008, 'Electronic tuberculosis surveillance systems: a tool for managing today's TB programs', International Journal of Tuberculosis and Lung Diseases 12(3 Suppl 1), 58-59. [ Links ]
National Planning Commission, 1997, National population policy for sustainable development, Windhoek. [ Links ]
Polit, D.F. & Beck, C.T., 2006, Essentials of nursing research: methods, appraisal and utilization, 6th edn., Lippincott Williams & Wilkins, London. PMid:10482253 [ Links ]
Polit, D. & Hungler, B.P., 1999, Nursing research principles and method, 6th edn., Lippincott, New York. [ Links ]
Shaw, V., 2005, 'Health information system reform in South Africa: developing an essential data set', Bulletin of the World Health Organization 83(8), 632-636. PMid:16184283 PMCid:PMC2626324 [ Links ]
Tomey, A.M., 2000, Guide to nursing management and leadership, 6th edn., Mosby, Missouri. [ Links ]
Vranken, R., Coulombier, D., Kenyon, T., Koosimile, B., Mavunga, T., Coggin, W., et al., 2002, 'Use of a computerized tuberculosis register for automated generation of case finding, sputum conversion, and treatment outcomes reports', International Journal of Tuberculosis and Lung Diseases 6(2), 111-120. PMid:11931409 [ Links ]
World Health Organization, 2003, Stop TB special project. Quality assurances of sputum microscopy in DOTS programmes, WHO, Geneva, Switzerland, viewed 24 February 2011, from http://www.who.int/ihr/training/laboratory_quality/11_cd_rom_tb_eqa_wpro.pdf [ Links ]
World Health Organization, 2006, The stop TB strategy. Building on and enhancing DOTS to meet TB-related millennium development goals, WHO, Geneva, Switzerland. [ Links ]
World Health Organization, 2008a, Implementing the STOP TB strategy: a handbook for the national TB control programme, WHO, Geneva, Switzerland. [ Links ]
World Health Organization, 2008b, Stop TB policy paper. Contributing to health system strengthening. Guiding principles for national TB programmes, WHO, Geneva, Switzerland. [ Links ]
World Health Organization, 2010, WHO policy on TB infection control in healthcare facilities, congregate settings and households, WHO, Geneva, Switzerland. [ Links ]
World Health Organization, 2011, 'WHO report 2011: Global tuberculosis control', viewed 30 June 2012, from http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdf [ Links ]
Zurovac, D., Rowe, A.K., Ochola, S.A., Noor, A.M., Midia, B., English, M., et al., 2004, 'Predictors of the quality of health worker treatment practices for uncomplicated malaria at government health facilities in Kenya', International Journal of Epidemiology 33(5), 1080-1091. http://dx.doi.org/10.1093/ije/dyh253, PMid:15256523 [ Links ]
 Correspondence:
Correspondence:
Muhammad Hoque
16 Piedmont Garden, 2 Piedmont Street, Durban
4091, South Africa
Email: muhammad.ehsanul@gmail.com
Received: 08 Oct. 2011
Accepted: 18 June 2013
Published: 22 July 2013

