










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Primary Health Care & Family Medicine
On-line version ISSN 2071-2936
Print version ISSN 2071-2928
Afr. j. prim. health care fam. med. (Online) vol.16 n.1 Cape Town 2024
http://dx.doi.org/10.4102/phcfm.v16i1.4288
ORIGINAL RESEARCH
Prognostic awareness and prognostic information preferences among advanced cancer patients in Kenya
Hussein EliasI, II; Semra OzdemirIII, IV; Joann BairaviIII; Emmah AchiengII, V; Eric A. FinkelsteinIII, VI
IDepartment of Family Medicine, Moi University School of Medicine, Eldoret, Kenya
IIAcademic Model Providing Access to Healthcare (AMPATH), Eldoret, Kenya
IIILien Centre for Palliative Care, Duke-NUS Medical School, Singapore, Republic of Singapore
IVDepartment of Population Health Sciences, Duke Clinical Research Institute, Duke University, Durham, United States of America
VMoi Teaching and Referral Hospital, Eldoret, Kenya
VIDuke Global Health Institute, Duke University, Durham, United States of America
ABSTRACT
BACKGROUND: Cancer is the third leading cause of death in Kenya. Yet, little is known about prognostic awareness and preferences for prognostic information
AIM: To assess the prevalence of prognostic awareness and preference for prognostic information among advanced cancer patients in Kenya
SETTING: Outpatient medical oncology and palliative care clinics and inpatient medical and surgical wards of Moi Teaching and Referral Hospital (MTRH) in Eldoret, Kenya
METHODS: The authors surveyed 207 adults with advanced solid cancers. The survey comprised validated measures developed for a multi-site study of end-of-life care in advanced cancer patients. Outcome variables included prognostic awareness and preference for prognostic information
RESULTS: More than one-third of participants (36%) were unaware of their prognosis and most (67%) preferred not to receive prognostic information. Increased age (OR = 1.04, 95% CI: 1.02, 1.07) and education level (OR: 1.18, CI: 1.08, 1.30) were associated with a higher likelihood of preference to receive prognostic information, while increased symptom burden (OR= 0.94, CI: 0.90, 0.99) and higher perceived household income levels (lower-middle vs low: OR= 0.19; CI: 0.09, 0.44; and upper middle- or high vs low: OR= 0.22, CI: 0.09, 0.56) were associated with lower odds of preferring prognostic information
CONCLUSION: Results reveal low levels of prognostic awareness and little interest in receiving prognostic information among advanced cancer patients in Kenya
CONTRIBUTION: Given the important role of prognostic awareness in providing patient-centred care, efforts to educate patients in Kenya on the value of this information should be a priority, especially among younger patients
Keywords: prognosis; prognostic awareness; prognostic information preferences; advanced cancer; Kenya.
Introduction
Cancer is the third leading cause of death by non-communicable disease in Kenya and incidence rates are increasing, up 37 000 from 2012 to 47 887 new cases in 2018.1,2,3 Despite rising incidence, no information exists regarding prognostic awareness or preferences regarding prognostic information among patients with advanced cancer in Kenya. Based on evidence from other African countries, many advanced cancer patients in Kenya are likely to be unaware of their prognosis or not inclined to receive prognostic information.4,5
Prognostic awareness can be defined as awareness of disease incurability and shortened life expectancy6 is associated with more frequent end-of-life discussions,7 more patient-centric care,8,9 earlier palliative support, fewer unwanted resuscitations10 and increased shared decision-making.11 Despite these benefits, prognostic awareness remains low among patients with advanced cancer globally.5,12 Patient preference for receiving prognostic information is thought to have increased in recent years as informed decision-making has become more common in medical settings.13 Nevertheless, studies show mixed results with some suggesting patients prefer not to receive prognostic information.14,15
We therefore aimed to examine prognostic awareness and preference for prognostic information among patients with advanced cancer treated at a single cancer centre in Kenya. We also assessed the relationship between prognostic awareness and preference for prognostic information and patient factors. Based on prior literature, we hypothesised that greater prognostic awareness and preference for receiving prognostic information would be associated with younger age,13,16 higher education,14,15 higher income16,17 and higher symptom burden.18,19
Research methods and design
Study design
Data for this study were collected as part of the Asian and African Patient Perspectives Regarding Oncology Awareness, Care, and Health (APPROACH) study, a multi-country cross-sectional study of end-of-life care among advanced cancer patients.
Setting
Data for the Kenya site were collected at Moi Teaching and Referral Hospital (MTRH), Eldoret, a level 6 hospital offering specialised oncological and palliative services with a catchment area of 24 million residents in Western Kenya, Eastern Uganda and South Sudan.
Study population and sampling strategy
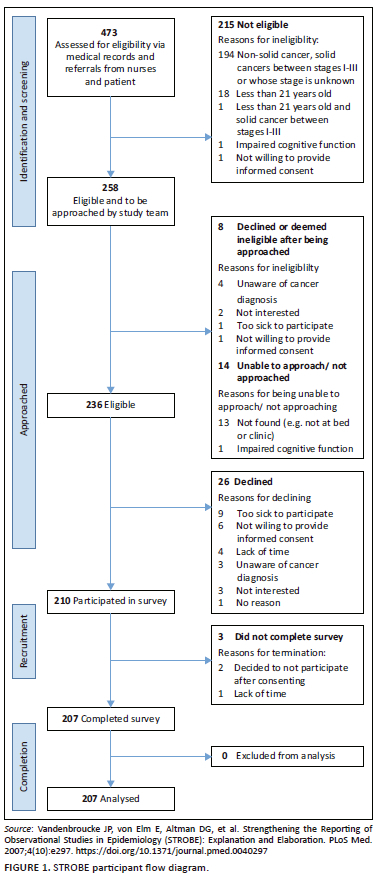
Eligible participants were: (1) ≥ 21 years old, (2) diagnosed with Stage IV solid cancer and (3) able to understand English and (4) seeking treatment at MTRH during the study period. Consistent with the multisite APPROACH protocol, we aimed to recruit a sample of 200 participants.20,21 To obtain this sample size, 473 patients were assessed for eligibility via daily screening of medical records of outpatients seen at the medical oncology and palliative care departments and inpatient medical and surgical wards and referrals from nurses and patient. Of the pool of patients, 266 were deemed ineligible based on medical record review or after being approached for the study or declined to participate. The remaining 207 patients were recruited for face-to-face interviews conducted at MTRH between October 2021 and February 2022. The STROBE participant flow diagram can be found in Figure 122. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist can be found in Online Appendix 1.
Measures
The survey questionnaire comprised validated scales and items developed by APPROACH study investigators in consultation with oncologists and research faculty at participating centres.23
Prognostic awareness
To assess prognostic awareness, participants were asked: 'Do you know the current stage (i.e. severity) of your cancer?'. As all respondents were advanced cancer patients, 'Early stage (Stage I, II, or III)' and 'don't know' responses were categorised as 'unaware' while 'Advanced cancer (Stage IV)' responses were categorised as 'aware'.
Patient preference for prognostic information
Patients were asked, 'Would you like to know how long you are likely to live under various treatment options?' A dichotomous variable for patient preference was created with a value of 1 for patients indicating, 'yes' in 'general or specific terms' and 0 for patients indicating 'no' or 'not sure'.
Participants' characteristics
Patients' age was extracted from patient medical records; all other variables were based on self-report. Participants reported years of education, perceived household economic status (0: low, 1: lower-middle, 2: upper middle or high) and how long they had known about their cancer diagnosis (0: <1 year, 1: 1 to 3 years, 2: > 3 years). Symptom burden was assessed using questions adapted from the Functional Assessment of Chronic Illness Therapy - Palliative Care instrument (FACIT-Pal) (Version 4).24 Examples of symptoms assessed included pain, shortness of breath and unintentional weight loss. The symptoms were scored on a 5-point Likert scale ranging from '0: not at all' to '4: very much'. Scores were then summed (total score range: 0 to 40) with higher scores indicating greater symptom burden.
Data analysis
We first summarise participants' characteristics with mean and standard deviations (s.d.) for continuous variables and frequencies and percentages for categorical variables. We then fit two binary logistic regression models to assess the association between participant characteristics and: (1) prognostic awareness and (2) preference for prognostic information. The dependent variables were prognostic awareness (0 = unaware, 1 = aware) and preference for prognostic information (0 = no or not sure; 1 = yes). Independent variables for both models were age, years of education, socioeconomic status and symptom burden.
We also conducted a post hoc estimation of the variance inflation factor (VIF) to assess multicollinearity between the independent variables.25 All analyses were conducted using Stata version 15.1.
Ethical considerations
Ethics approval was obtained from the National University Singapore-Institutional Review Board (NUS-IRB LB-15-319) and the Moi Institutional Research and Ethics Committee (IREC/2021/27). Trained interviewers obtained written informed consent from all participants prior to the survey. Only the trained interviewers and study team at MTRH had access to participants' confidential information. Participants were assigned a unique identification number and only de-identified data were collected and analysed.
Results
Participants' characteristics
Table 1 presents sample characteristics. Respondents ranged in age from 21 to 85 with a mean age of 55 (SD = 15.4) and an average of 8.5 (SD = 4.6) years of education. Slightly more respondents were female (57%) than male and most were married (76%). Perceived household economic status varied among participants with 37% indicating low, 38% indicating lower-middle and a quarter indicating upper-middle or high-income. Most participants (53%) had known of their cancer diagnosis for 1 to 3 years. Participants reported a mean symptom burden score of 13.9 (SD = 7.8; range: 0 to 37).
Prognostic awareness
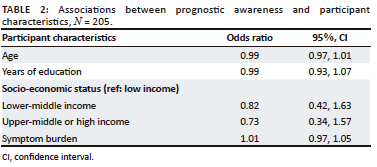
Nearly two-thirds of participants were aware of their prognosis (64%) (Table 1). When we examined participants' characteristics associated with prognostic awareness in the logistic regression model, we found no significant associations (Table 2).
Preference for prognostic information
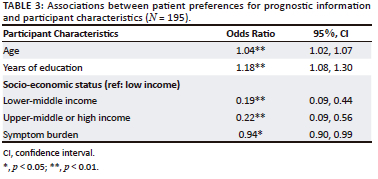
One-third (33%) of participants indicated a preference to receive prognostic information (Table 1). When we examined participants' characteristics associated with preference for prognostic information in the logistic regression model, we found significant associations with all participant characteristics (Table 3). Contrary to our hypotheses, increased age was associated with a higher likelihood (odds ratio [OR] = 1.04, 95% confidence interval [CI]: 1.02, 1.07) and increased symptom burden was associated with a lower likelihood (OR = 0.94, CI: 0.90, 0.99) of preference to receive prognostic information. Also contrary to our hypotheses, participants reporting higher perceived household income levels (lower-middle vs. low: OR = 0.19; CI: 0.09, 0.44 and upper middle or high vs. low: OR = 0.22, CI: 0.09, 0.56) were less likely to prefer receiving prognostic information. Supporting our hypothesis, participants reporting higher education levels were more likely (OR: 1.18, CI: 1.08, 1.30) to prefer prognostic information (Table 3). We did not observe multicollinearity in either of the multivariable models (VIF < 2).
Discussion
The primary aim of this study was to examine the prevalence of prognostic awareness and prognostic information preference among advanced cancer patients in Kenya. We also assessed associations between these outcomes and various participants' characteristics. More than one-third of participants (36%) were unaware of their prognosis (defined as current stage [i.e. severity] of cancer), and the majority of participants (67%) preferred not to receive prognostic information. Our findings related to prevalence of prognostic awareness are consistent with other studies of patients in Africa.5 Although our study did not investigate causal factors behind the low levels of prognostic awareness, prior research has suggested the paternalistic nature of the medical system in which patients are often not included as decision-makers, which may have played a role in low prognostic awareness.26,27 However, our results suggest most patients also prefer not to receive prognostic information.
To understand factors influencing prognostic awareness, we examined the relationships between awareness and preference for prognostic information and observable participants' characteristics. Prognostic awareness was not significantly associated with any of the patient factors examined; however, preference for prognostic understanding was strongly associated with patient factors. In line with prior literature, participants in our study reporting higher education levels were more likely to prefer to receive prognostic information.15 These findings are consistent with the notion that individuals with higher education levels tend to have better health literacy.
Contrary to prior studies, we found two generally disenfranchised groups, older adults and those reporting lower household income levels were more interested in receiving prognostic information than their counterparts. Older adults tend to have more emotional stability and to be more accepting of their situation,28 which may explain why they feel more comfortable requesting and receiving prognostic information.29 Although potential reasons for differences by perceived household income level are less obvious, it may be that individuals with lower income levels are more motivated to understand their illness trajectory so they have a better sense of related financial consequences, which may disproportionately impact their households.30 Lastly, we found higher symptom burden was associated with a lower likelihood of preference for prognostic information, perhaps suggesting patients with increased symptom burden are weary of receiving bad news.
Strengths and limitations
The strength of this study lies in its examination of patient prognostic awareness and preference for receiving prognostic information in a country in Africa (Kenya) where little information currently exists. This study has several limitations. One limitation was that the study was conducted in a single site in Kenya, and thus results may not be generalisable to other sites in Kenya or Africa. Likewise, the focus on a single condition (i.e. advanced cancer) and missing data (~5%) are additional limitations. Most importantly, this study evaluates correlations and thus cannot identify causal reasons behind the low levels of prognostic awareness and preference for receiving prognostic information. Future studies should explore causal factors related to low prognostic awareness and information preference among advanced cancer patients in Africa.
Conclusion
Our results reveal low levels of prognostic awareness and little interest in receiving prognostic information among advanced cancer patients in Kenya. Given the important role of prognostic awareness in providing patient-centred care, efforts to educate patients in Kenya on the value of this information should be a priority, especially among younger patients who were less likely to prefer prognostic information in our study. Interventions to address these concerns might include public health campaigns on the value of informed decision-making, provider training in health communication31 and protocols requiring informed consent32 and patient and provider education on advance care planning. Future research should test the effectiveness of these interventions in improving prognostic awareness.
Acknowledgements
The authors would like to acknowledge the financial support provided by the Duke Global Health Institute (DGHI) and the ongoing support from the COMPASS team. Declarations: The FACIT and all related works are owned and copyrighted by and the intellectual property of David Cella, Ph.D. Permission for use of the FACT or FACIT system of questionnaire is obtained by contacting information@facit.org.
Competing interests
The authors declare that they have no financial or personal relationship(s) that may have inappropriately influenced them in writing this article.
Authors' contributions
H.E. was involved in writing - review and editing, supervision, project administration, and funding acquisition. S.O. was responsible for writing - original draft, review and editing, formal analysis; supervision. J.B. performed project administration, writing - review and editing. E.A. was involved in writing - review and editing. E.A.F. was involved in writing - review and editing, supervision, project administration, funding acquisition.
Funding information
Financial support for this study was provided by Duke Global Health Institute (DGHI) (Grant no. 4531740-APPROACH). The funding agreement ensured the authors' independence in designing the study, interpreting the data, writing and publishing the report.
Data availability
De-identified data will be made available upon request and with proof of an approved ethics board approval.
Disclaimer
The views and opinions expressed in this article are those of the authors and are the product of professional research. It does not necessarily reflect the official policy or position of any affiliated institution, funder, agency, or that of the publisher. The authors are responsible for this article's results, findings, and content.
References
1. Jani PG, Craig H, Are C, Rooprai G. Cancer on the global stage: Incidence and cancer-related mortality in Kenya [homepage on the Internet]. World Health Organization Region: Africa. Harborside Press; 2021 [cited 2023 Aug 02]. Available from: https://ascopost.com/issues/february-25-2021/cancer-on-the-global-stage-incidence-and-cancer-related-mortality-in-kenya/ [ Links ]
2. Ministry of Health Kenya. National cancer control strategy 2017-2022. Nairobi: Ministry of Health Kenya; 2017. [ Links ]
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. https://doi.org/10.3322/caac.21492 [ Links ]
4. Nwankwo KC, Anarado AN, Ezeome ER. Attitudes of cancer patients in a university teaching hospital in southeast Nigeria on disclosure of cancer information. Psycho-Oncology. 2013;22(8):1829-1833. https://doi.org/10.1002/pon.3220 [ Links ]
5. Shen MJ, Prigerson HG, Ratshikana-Moloko M, et al. Illness understanding and end-of-life care communication and preferences for patients with advanced cancer in South Africa. J Glob Oncol. 2018;4:1-9. https://doi.org/10.1200/JGO.17.00160 [ Links ]
6. Diamond EL, Prigerson HG, Correa DC, et al. Prognostic awareness, prognostic communication, and cognitive function in patients with malignant glioma. Neuro Oncol. 2017;19(11):1532-1541. https://doi.org/10.1093/neuonc/nox117 [ Links ]
7. Tang ST, Chen CH, Wen F-H, et al. Accurate prognostic awareness facilitates, whereas better quality of life and more anxiety symptoms hinder end-of-life care discussions: A longitudinal survey study in terminally ill cancer patients' last six months of life. J Pain Symptom Manage. 2018;55(4):1068-1076. https://doi.org/10.1016/j.jpainsymman.2017.12.485 [ Links ]
8. Chu C, White N, Stone P. Prognostication in palliative care. Clin Med (Lond). 2019;19(4):306-310. https://doi.org/10.7861/clinmedicine.19-4-306 [ Links ]
9. Grad R, Légaré F, Bell NR, et al. Shared decision making in preventive health care: What it is; what it is not. Can Fam Physician. 2017;63(9):682-684. [ Links ]
10. Jackson VA, Jacobsen J, Greer JA, Pirl WF, Temel JS, Back AL. The cultivation of prognostic awareness through the provision of early palliative care in the ambulatory setting: A communication guide. J Palliat Med. 2013;16(8):894-900. https://doi.org/10.1089/jpm.2012.0547 [ Links ]
11. Kühne F, Hermann M, Preisler M, Rohrmoser A, Letsch A, Goerling U. Prognostic awareness in advanced disease: A review update and concept analysis. Front Psychol. 2021;12:629050. https://doi.org/10.3389/fpsyg.2021.629050 [ Links ]
12. Grant L, Downing J, Namukwaya E, Leng M, Murray SA. Palliative care in Africa since 2005: Good progress, but much further to go. BMJ Support Palliat Care. 2011;1(2):118-122. https://doi.org/10.1136/bmjspcare-2011-000057 [ Links ]
13. Xiao L, Peng M, Liu Y, Zhang L. Information, deliberation, and decisional control preferences for participation in medical decision-making and its influencing factors among Chinese cancer patients. Health Expect. 2021;24(5):1725-1736. https://doi.org/10.1111/hex.13312 [ Links ]
14. Tang ST, Liu TW, Chow JM, et al. Associations between accurate prognostic understanding and end-of-life care preferences and its correlates among Taiwanese terminally ill cancer patients surveyed in 2011-2012. Psychooncology. 2014;23(7):780-787. https://doi.org/10.1002/pon.3482 [ Links ]
15. Efficace F, Gaidano G, Sprangers M, et al. Preference for involvement in treatment decisions and request for prognostic information in newly diagnosed patients with higher-risk myelodysplastic syndromes†. Ann Oncol. 2014;25(2):447-454. https://doi.org/10.1093/annonc/mdt557 [ Links ]
16. Vlckova K, Tuckova A, Polakova K, Loucka M. Factors associated with prognostic awareness in patients with cancer: A systematic review. Psycho-Oncology. 2020;29(6):990-1003. https://doi.org/10.1002/pon.5385 [ Links ]
17. Wynn Mon S, Myint Zu WW, Myint Maw M, et al. Awareness of and preference for disease prognosis and participation in treatment decisions among advanced cancer patients in Myanmar: Results from the APPROACH study. Asia Pac J Clin Oncol. 2021;17(1):149-158. https://doi.org/10.1111/ajco.13430 [ Links ]
18. Chen J-S, Wen F-H, Chou W-C, Hsieh C-H, Chang W-C, Tang ST. Terminally ill cancer patients' distinct symptom-functional patterns/states are differentially associated with their accurate prognostic awareness in the last six months of life. J Palliat Med. 2019;22(7):782-789. https://doi.org/10.1089/jpm.2018.0538 [ Links ]
19. Bernat JK, Wittman DA, Hawley ST, et al. Symptom burden and information needs in prostate cancer survivors: A case for tailored long-term survivorship care. BJU Int. 2016;118(3):372-378. https://doi.org/10.1111/bju.13329 [ Links ]
20. Satija A, Bhatnagar S, Ozdemir S, et al. Patients' awareness of advanced disease status, psychological distress and quality of life among patients with advanced cancer: Results from the approach study, India. Am J Hosp Palliat Care. 2022;39(7):772-778. https://doi.org/10.1177/10499091211042837 [ Links ]
21. Wynn Mon S, Myint Zu WW, Myint Maw M, et al. Awareness of and preference for disease prognosis and participation in treatment decisions among advanced cancer patients in Myanmar: Results from the APPROACH study. Asia Pac J Clin Oncol. 2021;17(1):149-158. https://doi.org/10.1111/ajco.13430 [ Links ]
22. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007;4(10):e297. https://doi.org/10.1371/journal.pmed.0040297 [ Links ]
23. Jacob J, Palat G, Verghese N, et al. Health-related quality of life and its socio-economic and cultural predictors among advanced cancer patients: Evidence from the APPROACH cross-sectional survey in Hyderabad-India. BMC Palliat Care. 2019;18(1):94. https://doi.org/10.1186/s12904-019-0465-y [ Links ]
24. Lyons KD, Bakitas M, Hegel MT, Hanscom B, Hull J, Ahles TA. Reliability and validity of the Functional Assessment of Chronic Illness Therapy-Palliative care (FACIT-Pal) scale. J Pain Symptom Manage. 2009;37(1):23-32. [ Links ]
25. Hair JFJ, Anderson RE, Tatham RL, Black WC. Multivariate data analysis. 3rd ed. New York, NY: Macmillan; 1995. [ Links ]
26. Nwankwo KC, Ezeome E. The perceptions of physicians in southeast Nigeria on truth-telling for cancer diagnosis and prognosis. J Palliat Med. 2011;14(6):700-703. https://doi.org/10.1089/jpm.2010.0440 [ Links ]
27. Harris JJ, Shao J, Sugarman J. Disclosure of cancer diagnosis and prognosis in Northern Tanzania. Soc Sci Med. 2003;56(5):905-913. [ Links ]
28. Martins-Klein B, Bamonti PM, Owsiany M, Naik A, Moye J. Age differences in cancer-related stress, spontaneous emotion regulation, and emotional distress. Aging Ment Health. 2021;25(2):250-259. https://doi.org/10.1080/13607863.2019.1693972 [ Links ]
29. Ahalt C, Walter LC, Yourman L, Eng C, Pérez-Stable EJ, Smith AK. 'Knowing is better': Preferences of diverse older adults for discussing prognosis. J Gen Intern Med. 2012;27(5):568-575. https://doi.org/10.1007/s11606-011-1933-0 [ Links ]
30. Shankaran V, Jolly S, Blough D, Ramsey SD. Risk factors for financial hardship in patients receiving adjuvant chemotherapy for colon cancer: A population-based exploratory analysis. J Clin Oncol. 2012;30(14):1608-1614. https://doi.org/10.1200/JCO.2011.37.9511 [ Links ]
31. Mone S, Kerr H. Prognostic awareness in advanced cancer: An integrative literature review. BMJ Support Palliat Care. 2021;11(1):53-58. https://doi.org/10.1136/bmjspcare-2020-002287 [ Links ]
32. Nwodoh CO, Okoronkwo IL, Nwaneri AC, Ndubuisi I, Chinweuba AU, Iheanacho P. Terminally-ill patients' prognosis information preferences in an African setting: A qualitative descriptive study. Int J Afr Nurs Sci. 2020;13:100220. https://doi.org/10.1016/j.ijans.2020.100220 [ Links ]
 Correspondence:
Correspondence:
Eric Finkelstein
eric.finkelstein@duke-nus.edu.sg
Received: 04 Sept. 2023
Accepted: 26 Feb. 2024
Published: 11 Apr. 2024


{kind=link}