










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Primary Health Care & Family Medicine
versão On-line ISSN 2071-2936
versão impressa ISSN 2071-2928
Afr. j. prim. health care fam. med. (Online) vol.14 no.1 Cape Town 2022
http://dx.doi.org/10.4102/phcfm.v14i1.3256
ORIGINAL RESEARCH
Lifestyle determinants of diabetes mellitus amongst people living with HIV in the Eastern Cape province, South Africa
Nokwanda E. BamI; Wezile ChithaII; Jafta NtsabaIII; Sibusiso C. NomatshilaIV; Teke ApalataV; Sikhumbuzo A. MabundaVI
IDepartment of Nursing, Faculty of Health Sciences, North-West University, Mahikeng, South Africa
IIHealth Systems Innovation Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIDepartment of Nursing, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
IVDepartment of Public Health, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
VDepartment of Laboratory Medicine and Pathology, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
VIThe George Institute for Global Health, Faculty of Health Sciences, University of New South Wales, Sydney, Australia
ABSTRACT
BACKGROUND: Type 2 diabetes mellitus (DM) has serious consequences for those affected. Little is documented on the lifestyle determinants of type 2 DM in people living with human immunodeficiency virus (PLWHIV
AIM: This study aimed to assess the lifestyle determinants of type 2 DM amongst PLWHIV who were on antiretroviral treatment (ARV
SETTING: This study was undertaken in 10 community health clinics and 140 clinics in South Africa's Eastern Cape province
METHODS: This case control study was undertaken amongst PLWHIV who were on ARV in OR Tambo district
RESULTS: Cases and controls showed statistically significant differences on the duration of time on ARV (p < 0.0001), vigorous work (p = 0.019), participation in moderate sport (p = 0.007) and consuming daily fruit and vegetable servings (p = 0.021). Those reporting to be on ARVs for 6 to 10 years were three times more likely to be diabetic than those who had only been on ARV for a year or less (odds ratio [OR] = 3.0; p = 0.017) and in comparison, to participants who reported having one serving, participants who had four fruit and vegetable servings daily were 3.2 times more likely to be diabetic (OR = 3.2; p = 0.002
CONCLUSION: This study revealed significant nutritional imbalances on fruit and vegetable servings and on participation in moderate sport resulting in poor diabetic control. Routine screening and measurements need to focus on dietary and physical lifestyle determinants of type 2 DM in order to counsel patients on ARV on balanced nutrition and optimise outcomes in the quality care of PLWHIV
Keywords: lifestyle; people living with HIV; PLWHIV; type 2 DM; HIV/AIDS; patients; ARV.
Background
Age, female gender, diet, smoking and obesity are independently and collectively associated with higher risk of type 2 diabetes mellitus (DM).1 This is besides the established association between combined antiretroviral treatment (ARV) and DM.2,3,4,5 Indicators of obesity such as weight, body fat percentage, waist-hip circumference and body mass index (BMI) that are above the designated values are known to forecast DM.4,6
Human immunodeficiency virus (HIV) is hypothesised to predispose patients to DM through several mechanisms, some of which are not as yet completely understood.7 A 2014 United States (US) study8 found the prevalence of DM to be higher in overweight and HIV infected patients (3.9% and 12.7%) compared with amongst non-HIV infected patients (3.1% and 7.8%).8 Furthermore, type 2 DM has been reported to be more prevalent in people living with HIV (PLWHIV) at about 5.0% higher amongst females; 4.1% higher in the age-group between 20 and 44 years and 3.5% higher amongst non-obese PLWHIV when compared with the general population.4,9,10
It is further hypothesised that viral load fluctuations cause life-long inflammation, which in turn leads to DM because of the resultant insulin resistance; patients with low levels of cluster of differentiation 4 (CD4) count were reported to have higher problems with glucose metabolism than those with higher CD4 counts and through poorly understood mechanisms ARVs are highly associated with the prevalence of DM.2,3,4,9,10 Thus, greater risks for DM amongst PLWHIV are consistently and significantly associated with HIV disease progression.4,9,10
Even though ARVs should improve the immune status of PLWHIV, however, comorbid HIV and DM aggravated by ARVs has immunosuppressive consequences that create multiple complications for the sufferers and hasten deterioration, reduce quality healthcare and may result in death.2,11,12 Regardless of the HIV status, obese and overweight patients should have a balanced lifestyle that aims for the loss of 5% - 7% of their initial weight in order to improve insulin sensitivity, control hyperglycaemia and maintain overall quality of life.13,14
The purpose of embarking on an HIV-related study is that HIV infection amongst diabetes patients has deadly outcomes, that is, poorly controlled blood sugar levels resulting in kidney disease and neuropathy.12 Furthermore, South Africa has the highest global HIV and DM comorbid prevalence.2 A study conducted in the Eastern Cape, one of its rural provinces found a 21 times significantly higher association of being diabetic for PLWHIV on protease inhibitors (PIs) when compared with those on the fixed dose combination (FDC) of tenofovir, emtricitabine and efavirenz (p < 0.0001); stavudine (D4T) and zidovudine (AZT) were also reported to have higher associations with diabetes in comparison to patients on FDC (p < 0.05).2 Furthermore, that same study found a threefold higher association between a longer duration on ARVs and DM (p < 0.005).2
In the context of this study, some lifestyle determinants have affected the health of individuals through the development of type 2 DM, thus increasing complications and mortalities. The study sought to investigate the lifestyle determinants of type 2 DM in the context of antiretroviral drugs to make recommendations for mitigation measures. Hence, embarking on the study to describe the predictors and determinants of DM and identify lifestyle determinants associated with type 2 DM in PLWHIV on ARV. In addition, the 2013 South African national food-based-dietary guidelines pointed out that South African communities fall short on nutrition guidelines on fruit and vegetable servings both on national and individual levels.15 The author further described the variance to be related to fruit and vegetable quantities and sizes that were less than 200 g, thus exposing the population to non-communicable diseases (NCDs).15
The findings were much less than the ideal daily fruit and vegetable servings of 400 g, an equivalence of five servings or 80 g daily that is recommended to protect against NCDs, including cancers, cardiovascular disease and type 2 DM.16 Such an endeavour could enhance the care standards for patients with DM and PLWHIV17 and also make recommendations that could align the national policies with the World Health Organization (WHO) food guidelines.15,16 The results of the study will also contribute to better understanding of the multi-morbidity of HIV and type 2 DM and improve knowledge on how to maintain the quality of life amongst PLWHIV receiving ARV.
Methods
Design
A quantitative multicentre unmatched case-control study design was used to determine the lifestyle predictors of diabetes amongst PLWHIV on ARVs. Type 2 DM patients on treatment with comorbid HIV and on antiretroviral therapy (cases) were selected and compared with PLWHIV on antiretroviral therapy without DM (controls). This study draws on the design, population and sample of participants described by Bam et al.2
Setting and sample
This study was conducted in healthcare facilities of the Eastern Cape, one of South Africa's provinces. This is the second biggest province by surface area and the fourth most populous,18 as it has increased from 6.6 million in 2011 to 6.7 million in 2020.18 It has eight health districts, OR Tambo district being the largest was conveniently chosen for this study. The study site included 10 community health centres (CHCs) and 140 clinics that had a total of 2467 patients with diabetes amongst PLWHIV.
Two controls for every case were recruited from the HIV-positive patients who were in attendance in the same clinics as the cases. Cases were identified from the primary care information system in use between the 01st of April 2015 and the 31st of March 2016. Controls were identified through a simple random sampling process of the same information system as the cases and ensured that cases and controls represented the same health facilities and sub-districts. The study was explained to them and thereafter those who met the criteria voluntarily participated after an invitation to do so was extended to them till the desired sample size was achieved. The sample size was determined using the equation:

where n was the minimum sample size; Zα for a 95% confidence interval is a constant (1.96); p the anticipated proportion diabetes prevalence amongst PLWHIV is 8%4; and e is the maximum error accepted by the researchers at 4%.
This sample size of 177 represents the number of cases and thus 354 controls were recruited.
To be included, potential cases had to be at least 18 years old with type 2 DM on treatment and on ARVs for no less than 12 months. Cases and controls were unmatched in this study. We excluded patients with a history of defaulting ARVs on at least three different occasions.
Data collection
A structured, standardised and validated self-administered questionnaire survey that was adapted from the WHO Stepwise tool-2016 was translated from English to isiXhosa and administered to consenting individuals. The questionnaire enquired on participants' socio-demographic characteristics, physical activity, dietary practices and medical history. Socio-demographic factors measured include the level of education and marital status. Levels of physical activities included the types of work, recreational exercise and sport activities. Dietary practices assessed details on the intakes of fruit and vegetables and related dietary practices. Medical history included the arterial blood pressure (BP), medication including but not limited to ARVs and their complications, weight and height. Other objective measures include the height in centimetres, weight in kilograms and upper arm BP using a digital stadiometer (seca 787) and a digital BP monitor (Omron HEM-7321-E), respectively. Notwithstanding, medical records were used for the confirmation of participants' clinical records. The study was piloted in full on three primary care attendees in one of the communities that was eventually used for the study.
Data analysis
Data were captured in Microsoft Excel Office 16 and analysed using Stata 16.1 (Stata Corp., Lakeway Drive USA) was used for data management and analysis. The Shapiro-Wilk test was used to explore the normality of numerical data.19 As a result of non-normality of the distribution they were summarised using medians, 25th percentile and 75th percentile (interquartile range). Categorical variables were described using frequency tables and percentages. The Chi-squared test was used to compare two categorical variables. However, if 20% or more of the expected frequencies were less than 5 or observed frequencies less than 1 then the Fisher's exact test was used. The Mann-Whitney U test was used to compare the differences of two medians. Logistics regression analyses were used to report lifestyle determinants or predictors of type 2 DM. Purposeful selection of variables was undertaken to determine the best fitting model for inclusion in the multivariable model.2,20 An odds ratio (OR) is the relative measure of association used in this study and the 95% confidence intervals (95% CI) is used to report on the precision of estimates. The multivariable logistics regression analyses were adjusted for age and BMI as known confounders. For statistical significance, the p-value was set at less than or equal to 5% (p ≤ 0.05).
Ethical considerations
Formal ethical approval was sought with the Research Ethics Committee of Walter Sisulu University (075/2016). Gate - keeper permission to conduct the research was obtained from the Eastern Cape Department of Health and OR Tambo health district management and sub-districts. Research participants were informed about the purpose and objectives of the study prior to consenting to the study. The consent was sought by means of a letter and the participants were informed of their right to withdraw from the study at any time without penalty. The ethical principles that were applied in this study were respect of participants by obtaining permission, freedom to choose participation, anonymity and confidentiality, beneficence, privacy and dignity of the research participants.
Results
A total of 177 (33.3%) of cases and 354 (66.7%) of controls were recruited into the study. Table 1 summarises demographic characteristics of participants and shows that there was no statistical difference between the sex of cases and controls (p = 0.927); cases and controls had statistical differences when stratified by the level of education (p = 0.030), participation in moderate sport (p = 0.007 and undertaking vigorous work (p = 0.019). There were statistical differences on the number of years on ARVs between cases and controls (p < 0.0001).
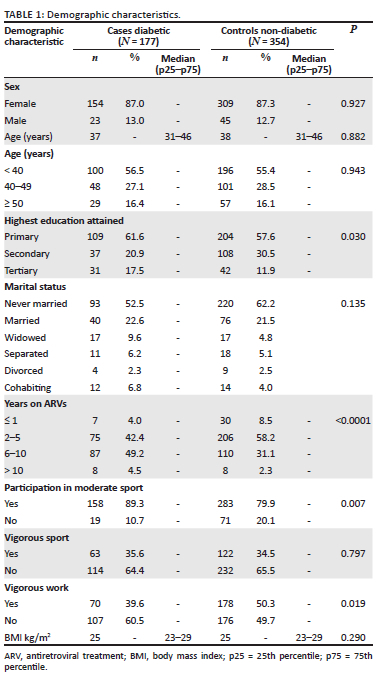
Table 2 shows the vegetables and fruit eating habits of participants and shows a statistical difference in the daily fruit servings of cases and controls (p = 0.021). On average, 85.9% (152/177) of cases and 89.8% (318/354) of controls consumed one or two fruit daily. Only 6.2% (11/177) of cases and 7.6% (27/354) of controls consumed five fruit and vegetable servings daily.
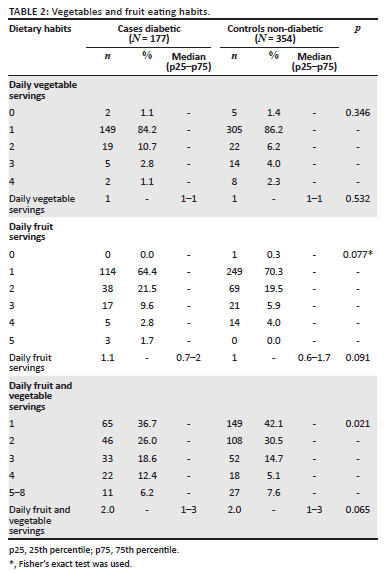
Table 3 shows that whilst 41.8% (74/177) of cases had previously been given BP advice, only 26.0% (92/354) of controls had been given BP advice (p < 0.0001). Other statiscally significant associations were the advice given on salt reduction (p = 0.021); the use of conventional antihypertensives (p < 0.0001) and being informed of a high BP (p < 0.0001).
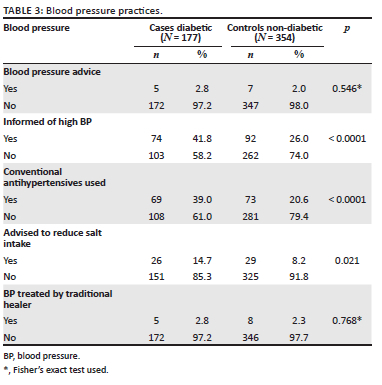
Table 4 shows the univariable and adjusted multivariable predictors of DM. Univariable analysis showed statistically significant associations of primary education (p = 0.048), tertiary education (p = 0.012); participation in moderate sport (p = 0.008); undertaking vigorous work (p = 0.020); a report of having an average of four fruit and vegetable servings per day (p = 0.003); previously being informed of having a high BP and being on conventional antihypertensives (p < 0.0001) and being previously given advice on the need for dietary salt reduction (p = 0.021). In addition, there was a 3.4 and 4.3-fold higher association with diabetes for those who were on ARVs for 6-10 years (p = 0.006) and more than 10 years, respectively, (p = 0.026), in comparison to participants who had only been on ARVs for 12 months or less and these were statistically significant.

Adjusted multivariable analysis showed that those reporting to have a tertiary education were twice more likely to be diabetic when compared with those with secondary education and this was statistically significant (p = 0.030). Other statistically significant associations include those participating in moderate sport, as they were 90% probable to be diabetic (p = 0.030); those reporting to be on ARVs for 6 to 10 years were 3.2 times more likely to be diabetic than those who had only been on ARVs for a year or less (p = 0.012) and those who reported having an average of four fruit and vegetable servings daily were 3.2 times more likely to be diabetic in comparison to those who reported having one daily fruit and vegetable servings (p = 0.002). Furthermore, those who reported undertaking vigorous work were 40% less likely to be diabetic compared with those who did not and this was statistically significant (p = 0.004).
Discussion
South Africa has shown great success in controlling the spread of HIV.21 The South African District Health Barometer (DHB) 2019/2020 reported a high number of adults whose viral loads were suppressed successfully per year.21 To the contrary, the country has seen prevalent type 2 DM amongst PLWHIV.2,21 This study, therefore, aimed to evaluate the lifestyle determinants of type 2 DM in the context of HIV or AIDS in the Eastern Cape province, one of South Africa's rural provinces. The findings of the study will not only add value to research practices but are also significant for health promoters, clinicians and regulators to refine knowledge, implement informed practices and enhance policies that will elevate the standard of care for PLWHIV.
The global report on type 2 DM describes the lifestyle determinants of DM as the lifestyle factors that contribute to the onset of type 2 DM, which include unhealthy diets, physical inactivity, smoking, alcohol, ethnicity and age.22 The report further explains that these factors are important in the prevention of type 2 DM. The results of this study were able to reveal the lifestyle determinants of type 2 DM amongst the PLWHIV on ARVs within the rural CHCs and clinics in South Africa. The multivariate analysis illustrated significant statistical differences between the cases and controls in the type 2 DM predictors such as level of education, physical activities, dietary habits and prolonged years on ARVs. The results show the need for routine screening and assessment of the lifestyle determinants of type 2 DM amongst PLWHIV on ARVs.4
Furthermore, the participants who took part in vigorous work had 40% decreased probability of type 2 DM compared with those who did not engage in vigorous activities (p = 0.004). In this study the respondents reported participation in vigorous work three to four days per week for approximately an hour and included lifting heavy objects or digging or construction work, which increased breathing and heart rate for at least 10 min continuously. The results are consistent with those of the 2015 American Heart Association recommendations of moderate to vigorous work activity of three to four days per week to protect against disease like type 2 DM.23
Significant contradictions were observed on moderate sport. For example, the participants who reported participation in moderate sport such as soccer had 90% likelihood of developing type 2 DM compared with those who did not (p = 0.030). In addition, other contradictions noticed were on dietary habits. Participants who reported eating four fruit and vegetable servings daily had greater probability of type 2 DM than those who only ate one serving per day (p = 0.002). The majority of participants in this study did not meet the WHO minimal guidelines of eating about two or more servings of fruit and vegetables servings per day, which is equivalent to a maximum of 400 g or five fruit and vegetable servings per day.16 This is contrary to a study by Frank et al. in low- and middle-income countries, which assessed participants from the age of 15 and above and found that older individuals were more likely to adhere to the recommended guidelines compared with younger individuals and females were more likely to comply with the guidelines than males.16,24 However, this study could not find any statistical difference between males and females and they still became more diabetic than their counterparts who had only one fruit and vegetable serving per day. This is unfortunately the limitation of self-reported data.
The WHO guidelines on fruit and vegetable serving further stipulate that adherence to the recommended daily servings could possibly prevent the occurrence of NCDs including type 2 DM.25 Furthermore, in order to achieve successful self-monitoring amongst diabetic patients, motivation is critical for effective self-monitoring and control of type two DM.26 These authors add that absence or lack of motivation in the form of supportive close friends or family members has negative consequences that may tamper with effective self-monitoring resulting in failure to adhere to DM control measures as observed in the study.26 It was not in the scope of this study to measure and monitor the fruit and vegetable quantities for the participants, but sought to evaluate the lifestyle determinants of type 2 DM. Future research needs to focus on the physical and dietary determinants of type 2 DM and particularly assess the fruit and vegetable measurements for individualised counselling on balanced nutrition for patients on ARVs.27
Antiretroviral drugs were significant lifestyle determinants of type 2 DM. The participants who were on ARVs for 6 to 10 years were 3.2 times more likely of being diabetic than those who were only on treatment for a year, and this was statistically significant (p = 0.012). The results are aligned with existing research amongst PLWHIV receiving ARVs.2,4 Notwithstanding the given findings, long-term prospective studies to establish causality would need to be carried out to confirm the causal link and mechanism of action between antiretroviral drugs and DM.2
This study had a few limitations. Firstly, this is a case-control study that could not ascertain causality but could only ascertain the existence of associations. Secondly, the information on exercise and nutrition was not triangulated. This could have helped establish certainty in the association between exercise and nutrition amongst PLWHIV. These could therefore be subjects of future qualitative and quantitative prospective studies.
Conclusion
The study found that the traditional risk factors such as a lack of physical activity, high BP, and a high BMI still play a role in the development of type 2 DM in the context of PLWHIV. In the diabetic-only population, however, the traditional risk factors seem ineffective as the odds of type 2 DM remained high despite vigorous sporting activity. The odds of type 2 DM were higher amongst the participants with tertiary education than those with primary education. Furthermore, the participants who were widows, separated, in cohabitation or married had higher probabilities of type 2 DM than those who were never married. Further research is therefore imperative to establish the specific issues that predispose married people, widows and people in cohabitation relationships to type 2 DM in order to tailor their care needs accordingly. In the context of HIV and AIDS moderate to vigorous work and sporting activity with increased intensity of at least three to four days per week is recommended not only to strengthen the heart muscle but also control type 2 DM.
Acknowledgements
The authors are grateful to the participants for their support of the study and time given to complete the questionnaires. The authors would also like to thank Dr Ndebia for data analysis of the thesis and the WSU library staff for assistance.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
N.E.B. contributed to study design, sourced supplementary funding, investigation, interpretation of results, wrote the first draft of the manuscript and edited versions of the manuscript. W.C. sourced funding and manuscript writing. J.N. contributed to study design and edited versions of the manuscript. S.C.N. and T.A. edited versions of the manuscript. S.A.M. oversaw all aspects of the manuscript, contributed to study design, data analysis, interpretation of results, compiled edits from other authors and signed off on the final version of the manuscript. The data set were accessed and verified by N.E.B. and S.A.M. All authors had full access to all the data in the study and had collective responsibility for the decision to submit for publication.
Funding information
The work reported herein was made possible through funding by the South African Medical Research Council (SAMRC) through its Division of Research Capacity Development (MRC-RFA-CC 01-2014) under the SAMRC Research Strengthening and Capacity Development Initiative (RCDI) Programme. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC.
Data availability
The original data of this study can be made available upon reasonable request from the corresponding author, N.E.B.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1. Pinchevsky Y, Butkow N, Raal FJ, Chirwa T, Rothberg A. Demographic and clinical factors associated with development of type 2 diabetes: A review of the literature. Int J Gen Med. 2020;2020(13):121. https://doi.org/10.2147/IJGM.S226010 [ Links ]
2. Bam NE, Mabunda SA, Ntsaba J, Apalata T, Nomatshila SC, Chitha W. The association between HIV tri-therapy with the development of type-2 diabetes mellitus in a rural South African district: A case-control study. PLoS One. 2020;15(12):e0244067. https://doi.org/10.1371/journal.pone.0244067 [ Links ]
3. Poornima M, Walvekar PR, Mallapur M, Katti S. Assessment of susceptibility to diabetes mellitus among rural population using Indian Diabetic Risk Score-a Cross Sectional Study. Int J Health Sci Res. 2016;6(2):54-58. [ Links ]
4. Gebrie A, Tesfaye B, Gebru T, Adane F, Abie W, Sisay M. Diabetes mellitus and its associated risk factors in patients with human immunodeficiency virus on anti-retroviral therapy at referral hospitals of Northwest Ethiopia. Diabetol Metabol Syndr. 2020;12(1):1-8. https://doi.org/10.1186/s13098-020-00527-1 [ Links ]
5. Adeyemi OM, Livak B, Orsi J, et al. Vitamin D and insulin resistance in non-diabetic women's interagency HIV study participants. AIDS Patient Care and STDs. 2013;27(6):320-325. https://doi.org/10.1089/apc.2012.0400 [ Links ]
6. Khatoon H, Hoda Z, Bais PS. To determine the association of anthropometric measurements and lipid profile with sagittal abdominal diameter in type 2 diabetes mellitus. Int J Health Sci Res. 2016;6(2):142-147. [ Links ]
7. Reid M, Tsima B, Kirk B. HIV and diabetes in Africa. Afr J Diabetes Med. 2012;20(2):28-32. [ Links ]
8. Hadigan C, Kattakuzhy S. Diabetes mellitus type II and abnormal glucose metabolism in the setting of HIV. Endocrinol Metabol Clin N Am. 2014;43(3):685. https://doi.org/10.1016/j.ecl.2014.05.003 [ Links ]
9. Tien PC, Schneider MF, Cox C, et al. Association of HIV infection with incident diabetes mellitus: Impact of using hemoglobin A1C as a criterion for diabetes. J Acquir Immune Defic Syndr (1999). 2012;61(3):334. https://doi.org/10.1097/QAI.0b013e31826bfc32 [ Links ]
10. Dimala CA, Atashili J, Mbuagbaw JC, Wilfred A, Monekosso GL. A comparison of the diabetes risk score in HIV/AIDS patients on highly active antiretroviral therapy (HAART) and HAART-naïve patients at the Limbe Regional Hospital, Cameroon. PLoS One. 2016;11(5):e0155560. https://doi.org/10.1371/journal.pone.0155560 [ Links ]
11. Moyo D, Tanthuma G, Mushisha O, et al. Diabetes mellitus in HIV-infected patients receiving antiretroviral therapy. S Afr Med J. 2014;104(1):37-39. https://doi.org/10.7196/samj.6792 [ Links ]
12. Pillay S, Aldous C, Mahomed F. A deadly combination-HIV and diabetes mellitus: Where are we now? S Afr Med J. 2016;106(4):378-383. https://doi.org/10.7196/SAMJ.2016.v106i4.9950 [ Links ]
13. American Diabetes Associationa. American Diabetes Association (ADA) diabetes guidelines summary recommendation from NDEI. Natl Diabetes Educ Initiat. 2016;39(1):1-46. [ Links ]
14. Mutimura E, Hoover DR, Shi Q, et al. Insulin resistance change and antiretroviral therapy exposure in HIV-infected and uninfected Rwandan women: A longitudinal analysis. PLoS One. 2015;10(4):e0123936. https://doi.org/10.1371/journal.pone.0123936 [ Links ]
15. Naudé CE. 'Eat plenty of vegetables and fruit every day': A food-based dietary guideline for South Africa. S Afr J Clin Nutr. 2013;26:S46-S56. [ Links ]
16. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases: 2013-2020 [homepage on the Internet]. Geneva; 2013 [cited 2021 Jun 09]. Available from: https://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf;jsessionid=AC930DF3FDA6BAB53D4A943E5D2DE924?sequence=1 [ Links ]
17. Monroe AK, Glesby MJ, Brown TT. Diagnosing and managing diabetes in HIV-infected patients: Current concepts. Clin Infect Dis. 2015;60(3):453-462. https://doi.org/10.1093/cid/ciu779 [ Links ]
18. Statistics South Africa. Mid-year population estimates 2020 [homepage on the Internet]. Pretoria: StatsSA; 2020 [cited 2021 Jun 09]. Available from: http://www.statssa.gov.za/publications/P0302/P03022020.pdf [ Links ]
19. Vetter TR. Fundamentals of research data and variables: The devil is in the details. Anesth Analg. 2017;125(4):1375-1380. https://doi.org/10.1213/ANE.0000000000002370 [ Links ]
20. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Sour Code Biol Med. 2008;3(1):1-8. https://doi.org/10.1186/1751-0473-3-17 [ Links ]
21. Massyn N, Barron P, Day C, Ndlovu N, Padarath A. District health barometer, 2018/19 [homepage on the Internet]. Durban: Health Systems Trust; 2020 [cited 2021 Jun 09]. Available from: https://www.hst.org.za/publications/District%20Health%20Barometers/DHB%202019-20%20Complete%20Book.pdf [ Links ]
22. World Health Organization. Noncommunicable diseases: Risk factors [homepage on the Internet]. [cited 2021 Jun 09]. Available from: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/ncd-risk-factors [ Links ]
23. American Heart Association. Moderate to vigorour - What is your level of intensity? [homepage on the Internet]. 2015 [cited 2021 Jun 09]. Available from: https://www.heart.org/en/healthy-living/fitness/fitness-basics/aha-recs-for-physical-activity-in-adults [ Links ]
24. Frank SM, Webster J, McKenzie B, et al. Consumption of fruits and vegetables among individuals 15 years and older in 28 low-and middle-income countries. J Nutr. 2019;149(7):1252-1259. https://doi.org/10.1093/jn/nxz123 [ Links ]
25. Agudo A, Joint FAO/WHO Workshop on Fruit and Vegetables for Health (2004: Kobe, Japan). Measuring intake of fruit and vegetables [electronic resource]/Antonio Agudo [homepage on the Internet]. World Health Organization; 2005 [cited 2021 Jun 09]. Available from: https://apps.who.int/iris/handle/10665/43144 [ Links ]
26. Lambrinou E, Hansen TB, Beulens JW. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur J Prev Cardiol. 2019;26(2_suppl):55-63. https://doi.org/10.1177/2047487319885455- [ Links ]
27. Schiever JF, Visser J, Van der Merwe M, Nel D. Evaluation of nutrition care to adult patients on HAART attending primary healthcare facilities in Mpumalanga. S Afr J Clin Nutr. 2019;32(1):13-20. https://doi.org/10.1080/16070658.2017.1412183 [ Links ]
 Correspondence:
Correspondence:
Nokwanda Bam
nok_bam@yahoo.co.uk
Received: 20 Sept. 2021
Accepted: 13 Feb. 2022
Published: 12 May 2022

