










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Primary Health Care & Family Medicine
versão On-line ISSN 2071-2936
versão impressa ISSN 2071-2928
Afr. j. prim. health care fam. med. (Online) vol.12 no.1 Cape Town 2020
http://dx.doi.org/10.4102/phcfm.v12i1.2215
SCIENTIFIC LETTER
Abnormal cervical cytology amongst women infected with human immunodeficiency virus in Limpopo province, South Africa
Samuel T. NtuliI, III; Eric MaimelaI; Linda SkaalI; Mabina MogaleII; Provia LekotaI
IDepartment of Public Health, Faculty of Health Sciences, University of Limpopo, Sovenga, South Africa
IIDepartment of Public Health, Faculty of Health Sciences, Sefako Makgatho Health Sciences University, Ga-Rankuwa, South Africa
IIIDepartment of Statistics and Operations Research, Sefako Makgatho Health Science University, Ga-rankuwa, South Africa
ABSTRACT
BACKGROUND: Cervical cancer remains the major public problem worldwide and the most common gynaecological malignancy in the developing world, particularly in sub-Saharan Africa.
AIM: To determine the prevalence of abnormal cervical cytology amongst women with and without human immunodeficiency virus (HIV) and examine the association between HIV and histological grading.
SETTING: The study was conducted in Limpopo province, which is the northernmost province of South Africa. The province has five district municipalities with one tertiary, five regional and thirty four district hospitals.
METHODS: We retrospectively reviewed cervical cancer cases in Limpopo province (LP) of South Africa, using data collected routinely by the National Health Laboratory Services (NHLS). The data on smears submitted for cytology between 2013 and 2015 were extracted from the Central Data Warehouse (CDW) database.
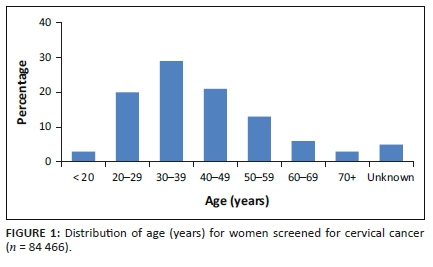
RESULTS: A total of 84 466 women were screened for cervical cytology smears. Their mean age was 39.8 ± 13.6 years, with range from 15 to 113 years; 77.2% were in the age group 30 years and older and 19.6% had an abnormal cervical cytology result. Overall, 46.4% of the women screened for cervical cancer were HIV infected. A significantly higher proportion of HIV-positive women had abnormal cytology than HIV-negative women (31.8% vs. 9.2%).
CONCLUSION: The prevalence of abnormal cytology amongst HIV-positive women is relatively high, and the risk appears to be significantly greater in all age groups. This finding highlights the need to ascertain HIV status of all women presenting with cervical cancer.
Keywords: cervical cancer; human immunodeficiency virus; Limpopo province; Prevalence; abnormal cytology.
Introduction
Cervical cancer (CC) is the most common gynaecological malignancy in the developing world, particularly in sub-Saharan Africa.1,2 Prevention of complications and improved survival from CC depend on early detection, treatment and human papillomavirus (HPV) vaccination before any sexual debut.3,4 Human papillomavirus has been known to increase with age; however, some age groups remain at higher risk of CC, especially those living with human immunodeficiency virus (HIV). The prevalence of abnormal cytology amongst HIV-positive women in African countries is 5% - 30%.5,6,7,8,9 In KwaZulu-Natal province of South Africa (SA), 54.9% of women living with HIV had abnormal Papanicolaou (Pap) smear results.10 In Limpopo province (LP), 26.7% of the HIV-positive migrant farm workers and sex workers had abnormal cervical cytology tests.11 Not surprisingly, studies report significantly higher burdens of abnormal cervical cytology in HIV-positive women, compared with HIV-negative women.12,13 The national guidelines in SA clearly state that women aged 30 years or older should be offered three free lifetime Pap smears,14 with recommendations to screen HIV-positive women annually.15 Despite all this, most women do not receive adequate screening.16,17,18 In LP, the annual screening coverage rates increased from 2.9% in 2007 to 4.2% in 201019; however, there is no information on the prevalence of cervical lesions amongst HIV-positive women. In an attempt to assess proportion of HIV-positive women with cervical lesions, our study analysed routinely collected data by the National Health Laboratory Services (NHLS).
Methods
We retrospectively reviewed CC cases in LP using data collected routinely by the NHLS. The data on smears submitted for cytology between 01 January 2013 and 31 December 2015 were extracted from the Central Data Warehouse database. The variables used for this study include date of smear collection, the women's ages at smear collection, HIV status, smear adequacy and smear cytology results. The details of the study setting, CC screening programme and data management are described in a previous study.19
Data were analysed using Stata® statistical software (Release 11; StataCorp, 2009, College Station, TX). Categorical and continuous variables were summarised using proportions (percentages) and means (standard deviation), respectively. The chi-square test was used to compare the two groups (i.e. HIV-positive and HIV-negative women). A p-value of less than 0.05 was considered to be statistically significant.
Ethical consideration
Ethical approval was obtained from Turfloop Research Ethics Committee (Ref: TREC/219/2106; PG) and permission to use the data was obtained from the National Health Laboratory Services (Ref No.: 2019609).
Results
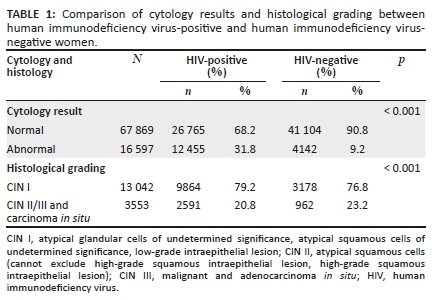
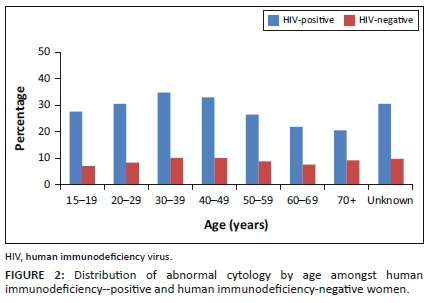
A total of 84 466 women were screened for cervical cytology smears. Their mean age was 39.8 ± 13.6 years, with range from 15 to 113 years. Figure 1 shows the age distribution of the women who participated in this study. Overall, 46% of the women screened for CC were HIV-infected. As shown in Table 1, a higher proportion of HIV-infected women had abnormal cytology as compared with women without HIV infection (31.8% vs. 9.2%, p < 0.05). With regard to histological grading, overall, 78.6% was low-grade squamous epithelial lesions Cervical intraepithelial neoplasm (CINI) and 21.4% was high-grade squamous epithelial lesions (CIN II/III and carcinoma in situ). For comparison of histological grading between HIV-positive and HIV-negative women, a significant higher proportion of HIV-negative women had CIN II/III and carcinoma in situ than those who tested HIV positive (23.2% vs. 20.8%, p < 0.05). In all age groups, the prevalence of abnormal cytology was significantly higher amongst HIV-positive women than amongst women who tested HIV-negative (p < 0.05; Figure 2).
Discussion
To our knowledge, this is the first study in LP to assess the prevalence of cervical lesions amongst HIV-positive women. Our finding shows that the prevalence of cervical lesions amongst HIV-positive women was 31.8%, which was significantly higher than 9.2% in HIV-negative women. This finding is slightly higher than 22% found in a study conducted in Swaziland12 but lower than 71.8% reported in Tanzania.13 Several studies conducted amongst women living with HIV found the prevalence of abnormal cytology of 54.9% in SA,10 26.7% in Kenya,5 26.8% in Tanzania,6 22.1% in Ethiopia,7 15.2% in Botswana9 and 6.0% in Nigeria.8 Afzal and co-authors in a study conducted in LP found that 26.7% of the HIV-positive migrant farm and sex workers had abnormal cytology.11 The reasons for various prevalence rates reported in these studies are unclear; however, it could be because of various methods used for CC screening20,21,22,23 and sexual practices of women,7,8,12,24,25 which is explained by higher burden of HPV infection.26,27,28,29
Despite the effectiveness of highly active retroviral therapy (ART) in preventing the development of cervical lesions,7,8 interestingly in our study, prevalence of abnormal cervical cytology was significantly higher in women with HIV than in women without HIV. Vafaei et al., in their study, reported a greater proportion of women with abnormal cervical cytology amongst HIV-positive women than in the general population.30 Although our study did not document CD4 count and/or whether HIV-positive women were on ART treatment or not, systematic reviews found that integration of cervical screening with HIV treatment is feasible and acceptable to women living with HIV.31,32
In accordance with SA national guideline on CC screening, our findings show that more than two-thirds of women screened were 30 years and older. Similarly, a study in Nigeria found that the majority of women screened for cervical lesions were 30 years and older.8 Not surprisingly, amongst younger women (< 30 years), abnormal cervical cytology was significantly higher in those with HIV. A retrospective study in Tygerberg Academic Hospital in Cape Town, SA, found many women younger than 30 years diagnosed with invasive CC.33 These findings support the recommendation made by Botha33 that all SA women should initiate cervical screening at the age of 25 years or at the time of diagnosis of HIV seropositivity.34
Studies in SA reported higher rates of CIN II/III and carcinoma in situ in HIV-positive women when compared with HIV-negative women.35,36 A similar finding was reported in LP amongst HIV-positive migrant farm workers and sex workers.11 In contrast, in this study, CIN II/III and carcinoma in situ were significantly higher amongst HIV-negative women than amongst HIV-positive women, which is in agreement with a study in Malawi.37 This study has several limitations similar to an earlier study in LP,19 which included limited clinical data such as missing HIV test results, unavailable CD4 count and ART treatment for HIV-positive women and screened patients not allocated the same laboratory identification number during follow-up visits.
Conclusion
Our study shows that the prevalence of abnormal cervical cytology amongst HIV-positive women is relatively high and the risk appears to be significantly greater in all age groups particularly young women. This finding highlights the need to ascertain HIV status of all women presenting with CC and more importantly implementation of effective HPV vaccination in the prevention of opportunistic infections in HIV-positive adults and adolescents.4
Acknowledgements
The authors thank the staff and management of the National Health Laboratory Services in Pietersburg Hospital of the Limpopo province for providing the data used in this study and Prof. Marianne Alberts and everyone who contributed in any way to the success of this study.
Competing interests
The authors have declared that no competing interest exists.
Authors' contributions
All authors contributed equally to this work.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability statement
Data is available from the authors upon request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69-90. https://doi.org/10.3322/caac.20107 [ Links ]
2.Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 cancer incidence and mortality worldwide: IARC cancer base No. 11. Lyon: International Agency for Research on Cancer; 2013. [ Links ]
3.Denny L, Prendiville W. Cancer of the cervix: Early detection and cost - Effective solutions. Int J Gynecol Obstet. 2015;131(S1):S28-S32. https://doi.org/10.1016/j.ijgo.2015.02.009 [ Links ]
4.Ghebre RG, Grover S, Xu MJ, Chuang LT, Simonds H. Cervical cancer control in HIV-infected women: Past, present and future. Gynecol Oncol Rep. 2017;21:101-108. https://doi.org/10.1016/j.gore.2017.07.009 [ Links ]
5.Memiah P, Mbuthia W, Kiiru G, et al. Prevalence and risk factors associated with precancerous cervical cancer lesions among HIV-infected women in resource-limited settings. AIDS Res Treat. 2012;2012:953743. https://doi.org/10.1155/2012/953743 [ Links ]
6.Kafuruki L, Rambau PF, Massinde A, Masalu N. Prevalence and predictors of cervical intraepithelial neoplasia among HIV infected women at Bugando Medical Centre, Mwanza-Tanzania. Infect Agent Cancer. 2013;8(1):45. https://doi.org/10.1186/1750-9378-8-45 [ Links ]
7.Gedefaw A, Astatkie A, Tessema GA. The prevalence of precancerous cervical cancer lesion among HIV-infected women in southern Ethiopia: A cross-sectional study. PLoS One. 2013;8(12):e84519. https://doi.org/10.1371/journal.pone.0084519 [ Links ]
8.Ononogbu U, Almujtaba M, Modibbo F, et al. Cervical cancer risk factors among HIV-infected Nigerian women. BMC Public Health. 2013;13:582. https://doi.org/10.1186/1471-2458-13-582 [ Links ]
9.Ramogola-Masire D, De Klerk R, Monare B, et al. Cervical cancer prevention in HIV-infected women using the 'see and treat' approach in Botswana. J Acquir Immune Defic Syndr. 2012;59(3):308-313. https://doi.org/10.1097/QAI.0b013e3182426227 [ Links ]
10.Katz IT, Butler LM, Crankshaw TL, et al. Cervical abnormalities in South African women living with HIV with high screening and referral rates. J Glob Oncol. 2016;2(6):375-380. https://doi.org/10.1200/JGO.2015.002469 [ Links ]
11.Afzal O, Lieber M, Dottino P, Beddoe AM. Cervical cancer screening in rural South Africa among HIV-infected migrant farm workers and sex workers. Gynecol Oncol Rep. 2017;20:18-21. https://doi.org/10.1016/j.gore.2016.12.011 [ Links ]
12.Jolly PE, Mthethwa-Hleta S, Padilla LA, et al. Screening, prevalence, and risk factors for cervical lesions among HIV positive and HIV negative women in Swaziland. BMC Public Health. 2017;17(1):218. https://doi.org/10.1186/s12889-017-4120-3 [ Links ]
13.Chambuso RS, Shadrack S, Lidenge SJ, et al. Influence of HIV/AIDS on cervical cancer: A retrospective study from Tanzania. J Glob Oncol. 2016;3(1):72-78. https://doi.org/10.1200/JGO.2015.002964 [ Links ]
14.South Africa Department of Health. National guidelines for cervical cancer screening programme [homepage on the Internet]. [cited 2018 Jan 07]. Available from: http://screening.iarc.fr/doc/SAcervical-cancer.pdf [ Links ]
15.Republic of South Africa. National consolidated guidelines for the Prevention of Mother-to-Child Transmission of HIV (PMTCT) and the management of HIV in children, adolescents and adults. Pretoria: Department of Health; 2014. [ Links ]
16.Hoque M, Hoque E, Kader SB. Evaluation of cervical cancer screening program at a rural community of South Africa. East Afr J Public Health. 2008;5(2):111-116. [ Links ]
17.Firnhaber C, Van Le H, Pettifor A, et al. Association between cervical dysplasia and human papillomavirus in HIV seropositive women from Johannesburg South Africa. Cancer Causes Control. 2010;21(3):433-443. [ Links ]
18.Firnhaber C, Mayisela N, Mao L, et al. Validation of cervical cancer screening methods in HIV positive women from Johannesburg South Africa. PLoS One. 2013;8(1):e53494 [ Links ]
19.Mamahlodi MT, Kuonza LR, Sue Candy S. Cervical cancer screening programme in Limpopo province: January 2007 to December 2010. South Afr J Gynaecol Oncol. 2013;5(1):4-10. [ Links ]
20.Begum SA, Rashid MH, Nessa A, Aziz MA, Zakaria SM, Roy JS. Comparative study between Pap smear and visual inspection using acetic acid as a method of cervical cancer screening. Mymensingh Med J. 2012;21(1):145-150. [ Links ]
21.Consul S, Agrawal A, Sharma H, Bansal A, Gutch M, Jain N. Comparative study of effectiveness of Pap smear versus visual inspection with acetic acid and visual inspection with Lugol's iodine for mass screening of premalignant and malignant lesion of cervix. Indian J Med Paediatr Oncol. 2012;33(3):161-165. https://doi.org/10.4103/0971-5851.103143 [ Links ]
22.Bhattacharyya AK, Nath JD, Deka H. Comparative study between pap smear and visual inspection with acetic acid (via) in screening of CIN and early cervical cancer. J Midlife Health. 2015;6(2):53-58. https://doi.org/10.4103/0976-7800.158942 [ Links ]
23.Izudi J, Adrawa N, Amongin D. Precancerous cervix in human immunodeficiency virus infected women thirty years old and above in Northern Uganda. J Oncol. 2016;2016:5473681. https://doi.org/10.1155/2016/5473681 [ Links ]
24.Moodley J, Constant D, Hoffman M, Salimo A, Allan B. Human papillomavirus prevalence, viral load and pre-cancerous lesions of the cervix in women initiating highly active antiretroviral therapy in South Africa: A cross-sectional study. BMC Cancer. 2009;9(1):275. https://doi.org/10.1186/1471-2407-9-275 [ Links ]
25.Horo A, Jaquet A, Ekouevi DK, et al. Cervical cancer screening by visual inspection in Cote d'Ivoire, operational and clinical aspects according to HIV status. BMC Public Health. 2012;12(1):237. https://doi.org/10.1186/1471-2458-12-237 [ Links ]
26.Richter K, Becker P, Horton A, Dreyer G. Age-specific prevalence of cervical human papillomavirus infection and cytological abnormalities in women in Gauteng Province, South Africa. S Afr Med J. 2013;103(5):313-317. https://doi.org/10.7196/SAMJ.6514 [ Links ]
27.McDonald AC, Tergas AI, Kuhn L, Denny L, Wright TC Jr. Distribution of Human Papillomavirus genotypes among HIV-positive and HIV-negative women in Cape Town, South Africa. Front Oncol. 2014;4:48. https://doi.org/10.3389/fonc.2014.00048 [ Links ]
28.Tayib S, Allan B, Williamson AL, Denny L. Human papillomavirus genotypes and clinical management of genital warts in women attending a colposcopy clinic in Cape Town, South Africa. S Afr Med J. 2015;105(8):679-684. https://doi.org/10.7196/SAMJnew.7890 [ Links ]
29.Ebrahim S, Mndende XK, Kharsany AB, et al. High burden of Human Papillomavirus (HPV) infection among young women in KwaZulu-Natal, South Africa. PLoS One. 2016;11(1):e0146603. https://doi.org/10.1371/journal.pone.0146603 [ Links ]
30.Vafaei H, Asadi N, Foroughinia L, et al. Comparison of abnormal cervical cytology from HIV positive women, female sex workers and general population. Int J Community Based Nurs Midwifery. 2015;3(2):76-83. [ Links ]
31.Sigfrid L, Murphy G, Haldane V, et al. Integrating cervical cancer with HIV healthcare services: A systematic review. PLoS One. 2017;12(7):e0181156. https://doi.org/10.1371/journal.pone.0181156 [ Links ]
32.White HL, Meglioli A, Chowdhury R, Nuccio O. Integrating cervical cancer screening and preventive treatment with family planning and HIV-related services. Int J Gynaecol Obstet. 2017;138(Suppl 1):41-46. https://doi.org/10.1002/ijgo.12194 [ Links ]
33.Diarra A, Botha MH. Invasive cervical cancer and human immunodeficiency virus (HIV) infection at Tygerberg Academic Hospital in the period 2003-2007: Demographics and characteristics. South Afr J Gynaecol Oncol. 2017;9(1):1-5. https://doi.org/10.1080/20742835.2017.1333700 [ Links ]
34.Botha MH, Guidelines for cervical cancer screening in South Africa. S Afr J Gynaecol Oncol. 2017;9(1):8-12. [ Links ]
35.Kuhn L, Wang C, Tsai WY, Wright TC, Denny L. Efficacy of human papillomavirus-based screen-and-treat for cervical cancer prevention among HIV-infected women. AIDS. 2010;24(16):2553-2561. https://doi.org/10.1097/QAD.0b013e32833e163e [ Links ]
36.Hank E, Hoque ME, Zungu L. Cervical precancerous lesions and cancer among patients in the gynaecology outpatient department at a tertiary hospital in South Africa. Asian Pac J Cancer Prev. 2013;14(8):4903-4906. https://doi.org/10.7314/APJCP.2013.14.8.4903 [ Links ]
37.Kohler RE, Tang J, Gopal S, et al. High rates of cervical cancer among HIV-infected women at a referral hospital in Malawi. Int J STD AIDS. 2016;27(9):753-760. https://doi.org/10.1177/0956462415592999 [ Links ]
 Correspondence:
Correspondence:
Samuel Ntuli
tsntuli@hotmail.com
Received: 01 Aug. 2019
Accepted: 01 Mar. 2020
Published: 06 Oct. 2020

