










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Journal of Primary Health Care & Family Medicine
On-line version ISSN 2071-2936
Print version ISSN 2071-2928
Afr. j. prim. health care fam. med. (Online) vol.9 n.1 Cape Town 2017
http://dx.doi.org/10.4102/phcfm.v9i1.1559
EDITORIAL
The Besrour Papers: Seeking evidence for family medicine
David Ponka
Department of Family Medicine, University of Ottawa, Canada
It has been said that 'location is a matter of geography, but global is a matter of the heart'.1 This is very much the spirit that guided the creation of the Besrour Centre at the Canadian College of Family Physicians in 2015 and that has guided its mission to generate knowledge about family medicine globally. The Centre believes that family medicine lies at the heart of health systems and provides a much-needed intersection between the clinical domain of primary care and the broader aims of the primary health care sector more generally (Box 1).

The spread of family medicine is of great interest around the world. This is why the Besrour Centre (http://www.cfpc.ca/The_Besrour_Centre) and Canadian Family Physician (CFP) have been publishing a series of articles on the evolution of the discipline2,3,4,5 and why the latest Besrour paper6 is an attempt to give a geographic overview of family medicine's development in each continent. Readers of The African Journal of Primary Health Care and Family Medicine will be interested to compare the discipline on the African continent with how it has evolved elsewhere. In addition, Dr John Parks and colleagues at the American Academy of Family Physicians and the Robert Graham Center conducted a comprehensive survey and developed a map of global family medicine in 2013.7 While family medicine has been slower to take hold in Africa compared to other parts of the world, we can also show that training there is now well established.
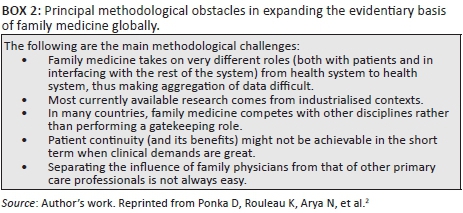
Certainly, surveying the remarkable spread of family medicine is indirect evidence of its utility, but we must do more to synthesise and aggregate data on the discipline. The Besrour Papers series initially deals with the methodological obstacles to studying such a diverse field2 (Box 2). The principal obstacle is the lack of a globally accepted definition of what constitutes a 'family doctor' because of the diverse roles that we play in our communities. A family doctor in Africa looks very different from a family doctor in Canada and, indeed, family doctors within Africa may look very different from one another. Are there core elements that inextricably bind us together? Some would suggest continuity of care is one such core feature. But this may be less achievable, at least initially, in contexts where clinical demand is overwhelming, such as parts of Africa. Others would point to comprehensiveness of services but, again, these vary greatly according to remoteness and community needs.
Perhaps this response to local context and need is a positive core element of our discipline. We should not seek homogeneity just for the sake of study and collating data. But are there any other competencies that we can consider universally fundamental to family medicine? In Canada, we use the Canadian Medical Education Direction for Specialists (CanMEDS) - Family Medicine framework.8 The generic CanMEDS framework (medical expert, communicator, collaborator, manager, health advocate, scholar and professional) is adapted with more unique family medicine attributes: being community-based, serving a defined population and having an approach based on the patient-physician relationship. The relationship with patients might not be unique to family doctors, but in the Canadian context, it is central to our role and our identity. Other regions have developed their own frameworks,5 and others continue this important process of self-definition. This is an essential prerequisite to continue to generate evidence on family medicine.
Because of these necessary local adaptations and the related diversity, we have also used narratives to better understand common threads in the discipline.3 There is perhaps a special role for narrative to describe a heterogeneous field and one based on relationships. And it is very likely that studying family medicine will continue to require a number of mixed-method approaches.
We continue to reach for evidence that family medicine plays, and can play in the future, a central role towards improving global health. Our next strategy, considering the heterogeneity of data that we have described, is to engage in high-quality cross-country comparisons9 with our partners in Brazil, another country where family doctors form the backbone of the health system. In doing so, we are reminded of how much we have to learn from one another.
References
1. Novak Z. Alpine heights (photograph). Can Med Educ J [serial online]. 2017 [cited 2017 May 2];8(2). Available from: https://journalhosting.ucalgary.ca/index.php/cmej [ Links ]
2. Ponka D, Rouleau K, Arya N, et al. Developing the evidentiary basis for family medicine in the global context. The Besrour Papers: A series on the state of family medicine in the world. Can Fam Physician [serial online]. 2015 Jul [cited 2017 Apr 24];61(7):596-600. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26380849 [ Links ]
3. Gibson C, Woollard R, Kapoor V, Ponka D. Narratives in family medicine: A global perspective. Can Fam Physician [serial online]. 2017 [cited 2017 Apr 24];63(2). Available from: http://www.cfp.ca/content/63/2/121 [ Links ]
4. Rouleau K, Ponka D, Arya N, et al. The Besrour conferences: Collaborating to strengthen global family medicine. Can Fam Physician [serial online]. 2015 Jul [cited 2017 Apr 24];61(7):578-581, 587-591. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26175361 [ Links ]
5. Gibson C, Arya N, Ponka D, Rouleau K, Woollard R. Approaching a global definition of family medicine. Can Fam Physician [serial online]. 2016 [cited 2017 Apr 24];62(11). Available from: http://www.cfp.ca/content/62/11/891 [ Links ]
6. Arya N, Gibson C, Ponka D, Haq C, Hansel S, Dahlman B, Rouleau K. Family medicine around the world: Overview by region. The Besrour Papers: A series on the state of family medicine in the world. Can Fam Physician. 2017 Jun;63(6):436-441. [ Links ]
7. Robert Graham Center. Maps, data, and tools [homepage on the Internet]. Washington, DC: Robert Graham Center; 2013 [cited 2017 Jul 15]. Available from: www.graham-center.org/rgc/maps-data-tools/interactive/world-health.html [ Links ]
8. Frank JR. The Royal College of Physicians and Surgeons of Canada. The CanMEDS 2005 physician competency framework [homepage on the Internet]. 2005 [cited 2017 Jun 30]. Available from: http://www.ub.edu/medicina_unitateducaciomedica/documentos/CanMeds.pdf [ Links ]
9. Cacace M, Ettelt S, Mays N, Nolte E. Assessing quality in cross-country comparisons of health systems and policies: Towards a set of generic quality criteria. Health Policy (New York) [serial online]. 2013 [cited 2017 May 11];112(1):156-162. Available from: http://www.sciencedirect.com/science/article/pii/S0168851013000961 [ Links ]
 Correspondence:
Correspondence:
David Ponka
dponka.md@gmail.com

