










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSA Journal of Industrial Psychology
versão On-line ISSN 2071-0763
versão impressa ISSN 0258-5200
SA j. ind. Psychol. vol.42 no.1 Johannesburg 2016
http://dx.doi.org/10.4102/sajip.v42i1.1264
ORIGINAL RESEARCH
Work-family conflict based on strain: The most hazardous type of conflict in Iranian hospitals nurses
Morteza CharkhabiI, II; Riccardo SartoriII; Andrea CeschiII
IFaculty of Psychology and Educational Science, K U Leuven, Belgium
IIDepartment of Human Sciences, University of Verona, Italy
ABSTRACT
ORIENTATION: Work and family conflicts continuously and negatively affect employees' performance. Previous research has mostly studied the impact of the two distinct dimensions of work-family conflict (WFC) and family-work conflict (FWC) on health outcomes, whereas the impact of more specific dimensions of these two general types of conflict on health outcomes is little known. Therefore, we now need to also measure the impact of more specified types of these conflicts on health outcomes.
RESEARCH PURPOSE: The purpose of this study was to propose a causal model of the effects of six different types of WFC (time, strain and behaviour) and FWC (time, strain and behaviour) on the mental and physical health of hospital nurses to identify the most hazardous type of conflict they faced.
MOTIVATION FOR THE STUDY: This research was conducted to outline which specific type of WFC or FWC is able to act as the strongest antecedent of mental and physical health in nurses.
RESEARCH DESIGN, APPROACH AND METHOD: Three hundred and eleven nurses from six hospitals were selected by simple random sampling. Data were collected using a Carlson WFC scale as well as an SF-36 mental-physical health scale based on a cross-sectional research design. The data were analysed using structural equation modelling and SPSS.
MAIN FINDINGS: The final model showed that, firstly, the effects of WFC types (time, strain and behaviour) on health outcomes were much greater than the effects of FWC types (time, strain and behaviour). Secondly, WFC and FWC based on strain were stronger predictors of health outcomes. Finally, strain-based WFC was identified to be the most hazardous type of conflict in our study.
PRACTICAL IMPLICATIONS: These findings can be employed by hospital managers to block all the potential factors that may increase strain-based WFC in the workplace. Moreover, this study helps hospitals to use special educational programs directed at reducing strain-based WFC.
CONTRIBUTION/VALUE-ADD: This research clearly revealed that a specific type of WFC may more likely influence the health situation of nurses.
Introduction
Over the past two decades, many hospitals have faced an increasing demand for health care because of the aging population (Lembrechts, Dekocker, Zanoni & Pulignano, 2015). The shortage of experienced nurses in both Western and Eastern countries also intensifies the working conditions for hospital nurses (McDermid, Peters & Jackson, 2012). This situation gives rise to an imbalance between the work and family aspects of their lives, which is labelled as work-family conflict (WFC) (e.g. Pal & Saksvik, 2008). One of the ways for nurses to reduce the heavy work demands is for nurses to leave the nursing profession (e.g. Bruck, Allen & Spector, 2002). Another way is by understanding the impacts of different types of WFC and family-work conflict (FWC) on the health situation of hospital nurses (Russell, O'Connell & McGinnity, 2009). This allows us to identify the most hazardous type of conflict as well as to plan more personalized methods and solutions for overcoming this conflict type.
Information and statistics collected from different countries around the world show that health problems lead many staff members to abandon their jobs. For example, in the Netherlands about 58% of work-related disabilities are linked to mental health (Grundemann, Nijboer & Schellart, 1991), whilst in England it is estimated that about 30%-40 % of illness-related absences are attributable to some form of mental disease (O'Leary, 1993). In line with these statistics, many Iranian researchers have shown that a huge number of Iranian employees are suffering from poor mental and physical health (e.g. HashemiNazari, Khosravi, FaghihZadeh & EtemadZadeh, 2007; HashemiSheykh Shabani, Arshadi & Bazrafkan, 2011) and are planning to quit their jobs (e.g. Sabokro, Baghbani & Amiri, 2013). Such health problems of nursing staff are leading to increased absences from work, have a negative effect on productivity and profitability, and impose a great loss on employers (Rajgopal, 2010). Studies conducted by the World Health Organization (WHO) and the International Labour Organization to investigate staff health in work environments show that increasing attention has been paid to mental health in the workplace (Gabrial & Liimatainen, 2000). According to research conducted by the European Agency of Safety and Health at Work (Cox, Griffiths & Rial-Gonzalez, 2000), 25% of public service workers, such as nurses, suffered from work-related health problems, such as job stress.
Recent research on shifting personnel, such as nurses, has studied the role of variables that may have negative and destructive effects on the mental and physical health of people. In this regard, a number of researchers have acknowledged that WFCs and FWCs negatively affect mental and physical health (Grzywacz & Bass, 2003; Oomens, Geurts & Scheepers, 2007).
Considering the fact that in nursing factors such as work shifts, long working hours, high workload per working shift, numerous encounters with sick people, efforts to respond to the demands of the work and family areas, and violence by clients in the workplace impose an imbalance between the work and family domains (Adib Hajbagheri, Salsali & Ahmadi, 2004), we are expecting to observe a high level of WFC and FWC in hospital nurses. In fact, the selection of nurses for our research sample may allow us to test our research hypotheses in a highly relevant context where the likelihood of occurrence of WFC and FWC is considerable. The purpose of the present study is to investigate the effects of six different types of WFC (time, strain and behaviour) and FWC (time, strain and behaviour) on the mental and physical health of nurses in order to identify which type of these conflicts has more negative effects on the mental and physical health of hospital nurses.
Nursing background in Iran
The Islamic Republic of Iran is a country of 70 million people, more than two-thirds of them under 30 years of age (Madad, 2007). Iranians are Muslims (98%), and their official language is Farsi, or Persian. According to the WHO, Iran's literacy rate is 82%; life expectancy for men is 70 years and 73 years for women (World Health Organization, 2008).
In Iran until 1915, patients received care from untrained hospital personnel. Subsequently, foreign missionaries came to Iran, and whilst they were performing their religious duties in Iran, they also introduced a modern kind of nursing and provided health care services. The missionaries trained a small number of Iranian women to care for hospital patients (Farsi, Dehghan-Nayeri, Negarandeh & Broomand, 2010). In 1916, the first nursing program was established in Tabriz City. After the Islamic revolution in 1979 and during the Iran-Iraq war, more male students were needed to enrol in the nursing programs. This was because male nurses were required to take care of male soldiers in the armed services. In 1986, approximately 50% of the baccalaureate students admitted to the nursing programs were men; however, at the present time, this number has decreased to approximately 20% (Nikbakht Nasrabadi, Lipson & Emami, 2004). At present, the baccalaureate program is the basic nursing program at the academic level and is the only way to registration as a professional nurse. Currently, there are approximately 70,000 nurses employed in the Iranian health care system. Male and female nursing students are enrolled at various universities to study nursing from the bachelor's to the doctoral level. Today, nursing in Iran is a recognized profession with its own association, Nursing Organization of the Islamic Republic of Iran, founded in 2000. This organization is charged with improving and promoting the Iranian nursing profession.
Socially and economically, nursing is a medium-prestige occupation in Iran, and nurses are working under the same pressures and demanding conditions as other nurses across the world. As most of the nurses in Iran are Muslim, and they have been brought up in the Islamic religious tradition, religion may not be considered as an unusual and cumbersome issue that may influence the work and family lives of nurses. But we should not ignore the importance of some recent issues such as the unfair international sanctions against Iran, which may influence the extent to which nurses perceive work-life and family-life conflict in their lives.
Work and family conflicts and health situation
In comparison with the past two decades, attaining a balance between work and family demands has become problematic for the majority of organizations, employees and families. It is widely accepted that incompatibility or conflict between these two domains has adverse effects on the health and well-being of employees (e.g., Kinnunen, Feldt, Geurts & Pulkkinen, 2006; Noor, 2003).
In recognition of this fact, it needs to be mentioned that, in spite of the various studies carried out by psychologists on work and family conflicts and their effects on the mental and physical health of staff in different countries, there are still numerous service staff that experience WFC and FWC in their daily lives. The evidence is taken from numerous studies that generally show negative effects of WFC on mental and physical health (e.g. Brough & O'Driscoll, 2005; Frone, Russell & Cooper, 1992; Grzywacz & Fuqua, 2000; Rozanti, Mohd Amin & Mohd Amin, 2014; Thomas & Ganster, 1995) and also negative effects of FWC on health outcomes (Cooklin et al., 2014; Grzywacz, 2000).
The importance of this issue is demonstrated by studies showing that WFC is significantly related to an increase in smoking, drinking alcohol, hypertension and obesity (Frone, 2000; Grzywacz, 2000, 2003; Kinnunen, Geurts & Mauno, 2004; Klitzman, House, Israel & Mero, 1990) whereas FWC is positively related to psychological distress (Frone, 2000). Reviewing research carried out in the past has led us to ask ourselves why, given the huge body of research in this field, this issue is still challenging and problematic. Trying to answer this question reveals a gap in knowledge regarding the link between conflicts and health outcomes.
In fact, most of the former research in this area has investigated the relationship of WFC and FWC with health outcomes in general (e.g. Mesmer-Magnus & Viswesvaran, 2005), whereas only a small portion of research has tried to go further and make a connection between some specific types of conflicts and health outcomes (e.g. Greenhaus & Beutell, 1985).
To overcome this challenge, we decided to take a deeper look at this association and investigate the effects of six different types of work and family conflicts on mental and physical health in order to answer the basic question of which type of conflict amongst the six would have more negative impact on the mental and physical health of nurses. Before achieving this aim, we have to explore definitions and approaches with regard to work and family conflicts.
Literature review
Work-family conflict generally refers to the extent to which work- and family-related demands interfere with each other and is typically defined as "a type of inter-role conflict that occurs as a result of incompatible role pressures from the work and family domains" (Greenhaus & Beutell, 1985, p. 77). With regard to work and family conflicts, an important point of view that has gained experimental support is the so-called spillover theory. According to this theory, the attitudes and experiences of a person in a domain (e.g. work) are positively related to the person's attitudes and experiences in another domain (e.g. family) (Brough & O'Driscoll, 2005). Although these spillover effects could be positive or negative, most of the studies on spillover concentrate on the negative effects of work-family imbalance (Carlson & Kacmar, 2000; Frone, 2003).
Another approach on WFC states that it appears when participation demands in the work domain are in contrast with participation demands in the family domain whereas FWC occurs when participation demands in the family domain are opposed to participation demands in the work domain. It is also possible to detect that the conflicts that emerge between these two domains could have important effects on the quality of life in both of the domains (Adams, King & King, 1996). As reported by Krause (2003), such a definition of WFC is based on the belief that we are dealing with a complex structure with multiple forms interacting in multiple domains. This phenomenon is assumed to be bidirectional, where work can interfere with family (work-to-family conflict) and family can interfere with work (family-to-work conflict; Frone, Yardley & Markel, 1997). Evidence suggests that WFCs and FWCs are different but reciprocally related (Byron, 2005; Mesmer-Magnus & Viswesvaran, 2005).
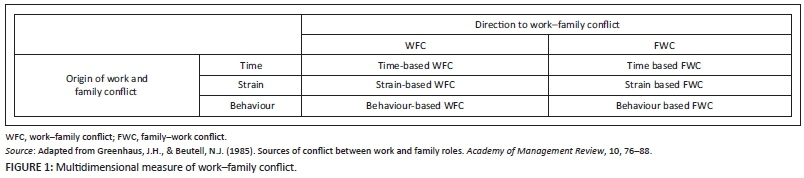
Although the theories mentioned above are not without criticism (Bellavia & Frone, 2005; Geurts & Demerouti, 2003), researchers typically argue that there are three major types of WFC: (1) time-based conflict (e.g. missing a family birthday party because of a work-related demand), (2) strain-based conflict (e.g. being irritable with family members following a stressful day at work), and (3) behaviour-based conflict (e.g. treating family members in the same way one treats subordinates in the workplace). Similarly, they have categorized FWC into three types: (1) time-based conflict (e.g. missing a work meeting because of a family-related demand), (2) strain-based conflict (e.g. being irritable with colleagues at work following a stressful day with the family), and (3) behaviour-based conflict (e.g. treating colleagues in the same way as one treats someone in the family) (Greenhaus & Beutell, 1985).
To elaborate, time-based and strain-based conflicts may occur because human resources are limited in terms of time and energy, which affects one's ability to cope with the demands of membership in different roles (Gutek, Searle & Klepa, 1991). Behaviour-based conflict originates from the existence of contradictory norms and expectations in one person's roles (Cooper, Dewe & O'Driscoll, 2001). Thus, the attitudes, values, and behaviours expected in one role may conflict with the same in another role (Cooper et al., 2001). As an example, characteristics that may be considered valuable in the workplace, such as materialism and aggression, may conflict with the needs and expectations of family members. The difficulty that people have reconciling these divergent claims could give rise to behavioural conflicts (Greenhaus & Beutell, 1985). Figure 1, adapted from Greenhaus and Beutell (1985, p. 78), graphically summarizes the different relationships established within the available literature between time-based, strain-based and behaviour-based conflicts and the work and family domain role expectations.
Based on the literature review, we find that until now most of the researchers in this area have generally been trying to consider only relationships between WFC or FWC (as two general types of conflict) and mental or physical health (e.g. Greenhaus, Allen & Spector, 2006). Regarding the importance of mental and physical health in the workplace (Gabrial & Liimatainen, 2000), what is lacking is a comprehensive study to cover the associations of the six different styles of WFC (time, strain and behaviour) and FWC (time, strain and behaviour) with mental and physical health. Thus, as mentioned earlier, the main goal of this research (and the gap that it is designed to fill) is to draw a causal model for a better understanding of the relationships between these six different conflicts and health outcomes (mental and physical). Moreover, the results will allow us to compare the negative effects of these six conflicts on health outcomes of nurses. For this reason, we have to review the associations between these conflicts and health outcomes specifically.
Time-based conflict and health outcomes
The essence of the conflict between the work and family domains is based in scarcity theory, whereby personal resources such as time, energy, and attention are deemed to be finite and the expending of greater resources in one domain (i.e. work) inevitably results in reducing the amount of resources left for the other domain (i.e. family) (Edwards & Rothbard, 2000; Greenhaus & Powell, 2003). In one of the earliest studies conducted within the work-family framework, Staines and O'Connor (1980) showed that competing demands for time is one of the most commonly cited challenges in balancing the work and family domains. Consistent with the work of Staines and O'Connor, other researchers suggest two forms in which time-based conflict manifests: (1) where it is physically impossible to satisfy the time demands of one role because of the time pressures of another role and (2) where one is mentally preoccupied with one domain despite being physically present in and attempting to meet the demands of the other domain (Greenhaus & Beutell, 1985). Therefore, on the basis of evidence suggesting that lack of time or time pressure can give rise to conflict in both domains of work and family, we proposed the following group of hypotheses:
H1: WFC based on time is negatively related to mental health.
H2: WFC based on time is negatively related to physical health.
H3: FWC based on time is negatively related to mental health.
H4: FWC based on is negatively related to physical health.
Strain-based conflict and health outcomes
Research on interrole conflict indicates that the excessive demands of one role inhibit the performance of the other role by creating strain for the individual in the form of dissatisfaction, tension, anxiety and fatigue (Edwards & Rothbard, 2000; Greenhaus & Beutell, 1985). In reviewing Greenhaus and Beutell's (1985) explanation of strain-based conflict, Edwards and Rothbard (2000) emphasize the depletion of personal resources needed for role performance as a result of physical and psychological strain. Thus, strain-based conflict does not imply competing demands directly but, rather, a situation in which participation in one domain results in either physical or psychological strain, which hinders role performance in the other domain (Edwards & Rothbard, 2000). In another study conducted by the same authors, it was found that individuals invested greater amounts of time in painful or dissatisfying role domains to overcome unpleasant experiences (Rothbard & Edwards, 2003). A negative psychological strain thus results in extensive time involvement in one domain, reducing the amount of time available for role performance in the other, potentially satisfying domain and resulting in conflict. Therefore, competing time demands can produce both strain-based and time-based conflict. Despite being conceptually distinct, time-based and strain-based conflicts have been found to share a number of sources within the work and family domains (Greenhaus & Beutell, 1985). Thus, in line with Rothbard & Edwards (2003) and Edwards and Rothbard (2000), we proposed the following group of hypotheses:
H5: WFC based on conflict is negatively related to mental health.
H6: WFC based on conflict is negatively related to physical health. H7: FWC based on conflict is negatively related to mental health.
H8: FWC based on conflict is negatively related to physical health.
Behaviour-based conflict and health outcomes
The final type of WFC is called behaviour-based conflict. When certain patterns of in-role behaviour become incompatible with expectations regarding behaviour in another role, behaviour-based conflict is said to occur (Greenhaus & Beutell, 1985). For example, an aggressive, confrontational and assertive approach to problem solving may be desirable in a work setting, whereas it might be inappropriate in a family setting, where a warm, nurturing and collaborative approach is preferred (Edwards & Rothbard, 2000; Greenhaus & Beutell, 1985). Like strain-based conflict, behaviour-based conflict depicts a 'negative spillover' from one domain to another, where behaviour desired and developed in one domain influences behaviour in the other domain whilst simultaneously inhibiting role performance in that latter domain (Edwards & Rothbard, 2000). Considering the results obtained by Edwards & Rothbard (2000), especially on the negative spillover process, we proposed the following group of hypotheses:
H9: WFC based on behaviour is negatively related to mental health.
H10: WFC based on behaviour is negatively related to physical health.
H11: FWC based on behaviour is negatively related to mental health.
H12: FWC based on behaviour is negatively related to physical health.
Research design
Research approach
A cross-sectional survey design was used to reach the research aims. Cross-sectional designs entail the collection of data on more than one case at a single point in time, after which the data are examined to detect patterns of association (Bryman & Bell, 2003).
Research Method
Sampling and data collection
Overview: The data for this study were collected as part of a larger research project for designing and testing a new model of the most important predictors of the mental and physical health of nurses. This new model was designed to conduct basic research on the health-related needs of Iranian nurses, who are working under demanding conditions, and to develop intervention materials to protect the health of these workers. Data were collected by structured self-reported surveys from nurses employed in six hospital units in the southwest of Iran. In the following sections, we describe the sampling, data collection, measures, and analysis strategy for each data source.
Recruitment: Male and female nurses who were formerly or are currently employed in six big hospitals were eligible to participate in this research. Participants were purposefully selected to ensure the inclusion of workers in a wide variety of nursing jobs in these hospitals. Such purposive sampling is typically used in qualitative research to find people who have depth and breadth of experience in an occupation and are sufficiently articulate and thoughtful to provide useful data (Quandt & Arcury, 1997). The selected people were informed about the instructions needed for filling out self-reported surveys. At the end of this step, we could get a collection of contributions from a variety of nurses.
Participants
In this study, 311 male (n = 46) and female (n = 265) hospital nurses from six units completed the clarified surveys. Their ages ranged from 21-57 years (M = 33.19, SD = 7.03). Slightly over half of them were married or living with their partners (n = 191), and the rest were single (n = 120). The majority reported having a formal education, with at least a bachelor's degree (n = 223). Also, the participants had working records ranging from 1-30 years (M = 9.41, SD = 6.08).
Data collection
Data were collected through the questionnaire method (survey), where self-reported questionnaires were administered. Closed-ended questions were used to gather information. The participants were given adequate time and freedom to answer the questions, allowing for accurate information to be collected. The use of closed-ended questions helped in restricting the participants from having to answer certain questions and in gathering a wide range of information.
Data analysis
The data were analysed by structural equation modelling (SEM) and SPSS Version 21. We used SEM as we wanted to examine the effects of six types of conflicts (or observed variables) on health outcomes (or latent variables) simultaneously. All the model indices were checked, and the final model indices were found to be statistically significant and acceptable.
Measuring instruments
Mental and physical health scale: The mental and physical health of nurses was assessed by the mental and physical health self-reported tool (Ware, Kosinski, Turner-Bowker, Gandeck, 2007). This tool consists of 36 items and can measure mental and physical components separately. We modified the rating scale from an effective response set to a frequency response set in order to better characterize the frequency of mental and physical health in this population. Our experience in conducting research in this population suggests that nurses have difficulties when responding to items with affective response sets (e.g. strongly agree to strongly disagree). Response options were never, rarely, sometimes, often, and always. In the present study, reliability (Cronbach's a) and validity for mental health were 0.91 and 0.70, and for physical health, they were 0.90 and 0.68, respectively.
Work-family conflict scale: In order to measure WFCs and FWCs, the 18-item multidimensional-measure work-family questionnaire by Carlson, Kacmar and Williams (2000) was used. This scale evaluates all six types of work and family conflicts. The domain of answers was ordered on a Likert scale from 1 (completely disagree) to 5 (completely agree). Nine items on this test measure WFCs, and the remaining 9 items evaluate FWCs. Higher scores on this test show more WFC. The items on this questionnaire are divided into six categories so that the first three items are about time-based WFC (the time spent on a job that reduces the time required for family activities), the second three items are about time-based FWC (the time spent on family activities that reduces the time required for doing the job), the third three items are about strain-based WFC (the amount of energy spent on doing the job that reduces the energy remaining for family activities), the fourth three items are about strain-based FWC (the amount of energy spent on family activities that reduces the energy remaining for doing the job), the fifth three items are about behaviour-based WFC (the interference of working behaviours and norms with family behaviours and norms), and the sixth three items are about behaviour-based FWC (the interference of family behaviours and norms with working behaviours and norms). Carlson et al. (2000) reported the reliability coefficient with Cronbach's alpha for this test to vary between 78.0 and 87.0. Final coefficients for the WFC dimension of this scale have been calculated as 85.0 and 67.0 using Cronbach's alpha and bisection, respectively. Final coefficients for the FWC dimension of this scale have been calculated as 80.0 and 72.0 using Cronbach's alpha and bisection, respectively.
Results
Resolving the issues that were stated in the preceding section, the data were processed using the statistical software package SPSS 21 and the SEM package AMOS 21. The research results are presented in two parts: (1) descriptive statistics and (2) structural model.
Descriptive statistics
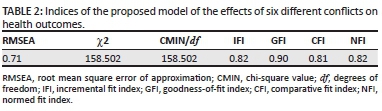
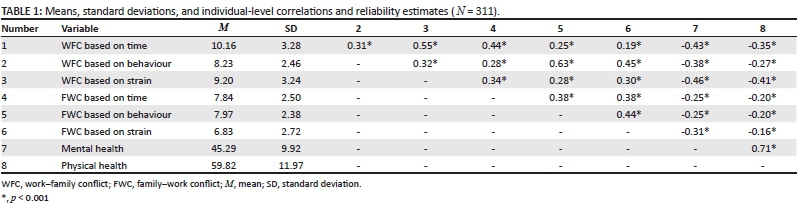
Table 1 shows the descriptive statistics and the covariance matrix between the independent and dependent variables in the present study. In Table 1, all the correlations and descriptive information are given.
As seen in Table 1, there is a negative, strong and highly significant association between the three types of WFC (time, behaviour and strain) and mental and physical health. In the table, in the WFC category, the highest correlations can be seen between WFC based on strain and mental health (r = -0.46, p = 0.001) and between WFC based on strain and physical health (r = -0.41, p = 0.001). Moreover, Table 1 shows that the relationships between all types of FWC (time, behaviour and strain) and mental and physical health are statistically significant but negative. The highest correlations can be seen between FWC based on strain and mental health (r = -0.31, p = 0.001) and between FWC based on time and FWC based on behaviour (together) and physical health (r = -0.20, p = 0.001). In fact, the table shows that all forms of WFC and FWC have a negative effect on the mental and physical health of nurses but the amount of this relation between the various types of work and family conflicts and health outcomes varies.
Structural model
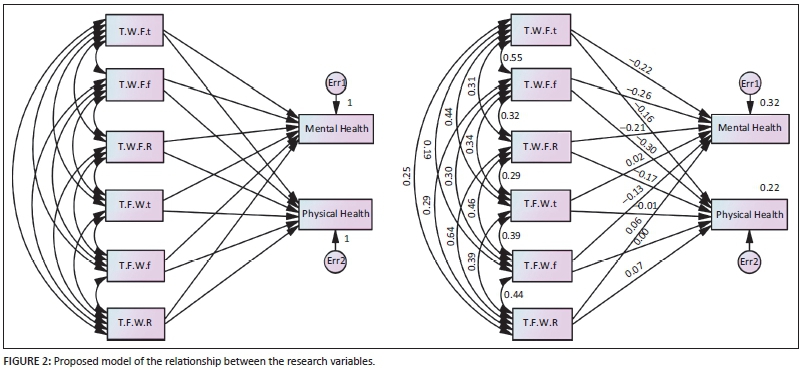
As a methodological point, it must been taken into account that for more generalization of the results, it would not be so realistic if we paid attention only to the simple correlations between these conflicts and health outcomes without considering other conflicts in the same time and situation. This is so because in a real situation each nurse is experiencing all these types of conflict at the same time and we do not know which of them can have a more negative effect on the health of a nurse compared with the others. It would be necessary to draw a comprehensive causal model using SEM to consider all of these causal relations simultaneously in order to find out the destructive portion of each conflict on health outcomes whilst considering other coexisting conflicts. In that case, the results will be more realistic and generalized. To achieve this goal, on the basis of the literature, we drew a proposed model by the SEM method (Figure 2).
Table 2 shows that revisions are necessary in order to propose an improved model.
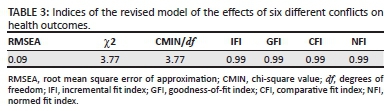
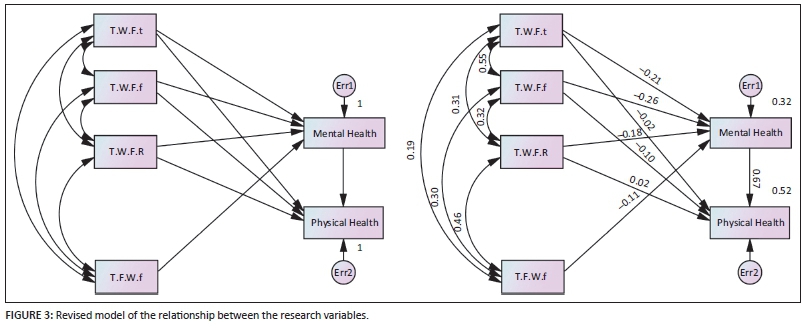
In the second model presented, we tried to draw a revised model of the dynamic relations amongst the variables. For this, we made some new connections between the variables and removed some of the former connections from the first model. Moreover, we correlated and removed the standard errors between the latent variables. Then, after a lot of changes we created the revised model with an improved collection of indices, presented in Figure 3.
Table 3 shows the improved indices in the revised model. We concluded that these model indices are scientifically acceptable, but regarding the amount of regression sums, we again decided to make modifications in the revised model and created a final model of the arrangement between the research variables.
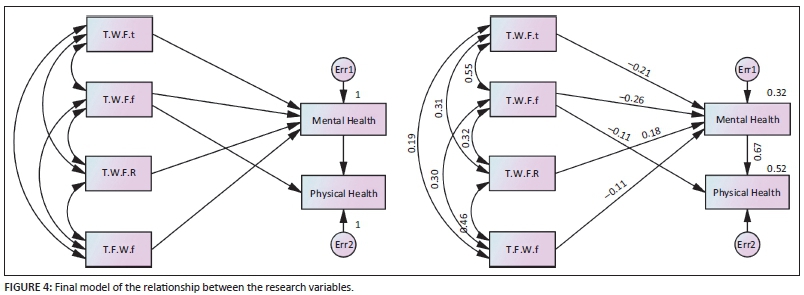
We removed some of the weak or insignificant relations between the variables in the revised model and established our final model as displayed in Figure 4.
As you can observe in Table 4, the new indices displayed indicate that the numbers, arrangements, and connections between variables are defined correctly.
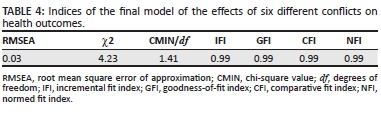
A comparison of the three models shows that the final SEM analyt (χ2/df = 1.41, goodness-of-fit [GFI] = 0.99, comparative fit index [CFI] = 0.99, incremental fit index [IFI] = 0.99, normed fit index [NFI] = 0. 99, and root mean square error of approximation [RMSEA] = 0.03). Based on the final model, we investigated the proposed hypotheses.
The first group of hypotheses were related to the association between WFC/FWC based on time and health outcomes. The results showed that WFC based on time is significantly related to mental health, providing support for H1 (β = 0.64, p < 0.001), but is not significantly related to physical health, so that H2 is rejected. Similarly, FWC based on time did not have a significant relation with both mental and physical health. Thus, both H3 and H4 were rejected.
The second group of hypotheses concerned the association between WFC/FWC based on strain and health outcomes. In support of H5 and H6, we showed that WFC based on strain is significantly related to both mental health (β = 0.78, p < 0.001) and physical health (β = 0.39, p < 0.01) whereas FWC based on strain is only correlated to mental health (β = 0.41, p < 0.03) but not to physical health. Therefore, H7 is approved, but H8 is rejected.
The last group of hypotheses focussed on the relation between WFC based on behaviour and health outcomes (H9 and H10) and FWC based on behaviour and health outcomes (H11 and H12). As is clear in the final model, WFC based on behaviour is significantly related to mental health (β = 0.73, p < 0.001) but not to physical health. Therefore, H9 is approved, but H10 is rejected. In addition, we could not find significant relations between FWC based on behaviour and both health outcomes. Therefore, both H11 and H12 are rejected.
Discussion and conclusion
The study examined the direct effects of six different types of WFC (time, behaviour and strain) and FWC (time, behaviour and strain) simultaneously on the mental and physical health of nurses. In fact, the most important gap in current research compared with earlier related studies was the lack of simultaneous and specific attention to the negative effects of the six different types of WFC and FWC on health outcomes.
Reviewing the past research showed that there was no research done that had investigated the relation between these six conflicts and health outcomes in the same time period. Most of the former studies had investigated WFC and FWC as two distinct constructions with regard to health outcomes (Frone, Russell & Cooper, 1992; Grzywacz & Fuqua, 2000; Thomas & Ganster, 1995) or had focussed only on the relationship of one aspect of these conflicts with health outcomes (Grzywacz, 2000). Our study found that both mental and physical health are affected by WFC (time, behaviour and strain) and FWC (time, behaviour and strain) but this impact is more from WFC (time, behaviour and strain) than from FWC.
These findings are consistent with scarcity theory, whereby employees' resources such as time, energy and attention are deemed to be finite and the expending of greater resources in one domain (i.e. work) inevitably results in reducing the amount of resources left for the other domain (i.e. family). Moreover, the findings are also in line with the work of Staines and O'Connor (1980). Other researchers suggest two forms in which time-based conflict manifests: (1) where it is physically impossible to satisfy the time demands of one role because of time pressures in another role and (2) where one is mentally preoccupied with one domain despite being physically present in and attempting to meet the demands of another. This is consistent with our finding about the negative effect of WFC based on time on mental health (H1).
Our results also suggest that when personal resources are depleted as a result of physical and psychological strain, one can expect the occurrence of conflict in employees. Thus, strain-based conflict does not imply competing demands directly but, rather, a situation in which participation in one domain results in either physical or psychological strain that hinders role performance in the other domain (Edwards & Rothbard, 2000, 2003). This supports of our findings about the negative effects of both WFC based on strain and FWC based on strain on mental and physical health (H5, H6 and H7). A comparison of all the types of conflicts revealed that WFCs/FWCs based on strain have more significant connections with health outcomes than other types of conflicts. Also, the results showed that the most hazardous type of conflict is WFC based on strain, which had the highest significant negative effect in reduction of both mental and physical health levels in nursing staff (H5 and H6); this must be taken seriously into account in future research.
We also showed that WFC based on behaviour is negatively related to mental health (H9). It should be noted that consistent with strain-based conflict, behaviour-based conflict depicts a 'negative spillover' from one domain to another, where behaviour desired and developed in one domain influences behaviour in the other domain whilst simultaneously inhibiting role performance in that latter domain (Edwards & Rothbard, 2000). When certain patterns of in-role behaviour become incompatible with expectations regarding behaviour in another role, behaviour-based conflict is expected to occur (Greenhaus & Beutell, 1985).
Furthermore, the results obtained from SEM clearly indicate three important points. Firstly, the predictive power of all three types of WFC for the mental and physical health levels of nurses is considerably higher than that of all three types of FWC. Health experts should especially pay attention to this result and focus more on finding methods for decreasing the negative effect of these three types of WFC. Secondly, the fact that the highest number of participants in this study were women (Nf= 265) makes these results very interesting. It means that women nurses face more conflicts and pressures in their work roles than in their family roles, which indicates the change in women's focus from family-relevant roles to the work area and its relevant roles. In other words, work roles impose a higher negative load on the mental and physical health of employed women than family roles. Thirdly, a simple correlation amongst the variables showed that strain-based conflict is the strongest of the different types of conflict. The results obtained from SEM also confirmed this finding. This means that assigning more responsibilities to a person with time and energy remaining constant could definitely cause him or her mental and physical difficulties. Therefore, assigning more responsibility, especially to employed women, should go along with increased task time or an increase in the individual's power to prevent this type of conflict. Fourthly, strain-based conflict is one of the most dangerous styles of WFC and FWC, and serious efforts must be made to prevent its occurrence by using proper interventions and methods inside the hospital.
Limitations
This study has some limitations, like other studies. Firstly, we drew our sample from staff nurses. This limits the generalization of our results to other samples. Secondly, given the cross-sectional design of this study, causal relationships amongst the variables cannot be established. Longitudinal studies should be employed to test the hypotheses. Finally, all the questionnaires we used in this study were self-reports. It would be better to use a combination of self-report questionnaires and objective assessments in future research. We also suggest that future studies test for an indirect effect from physical or psychological strain to physical health through mental health as our structural model showed that it would be possible to imagine such a path, although we did not test it in our study.
Acknowledgements
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
M.C. and R.S. contributed equally to the writing of this article. A.C. reviewed and edited the text.
References
Adams, G.A., King, L.A., & King, D.W. (1996). Relationships of job and family involvement, family social support and work-family conflict with job and life satisfaction. Journal of Applied Psychology, 81(4), 411-420. [ Links ]
Adib Hajbaghery, M., Salsali, M., & Ahmadi, F. (2004). The factors facilitating and inhibiting effective clinical decision-making in nursing: A qualitative study. BMC Nursing, 3(2), 1-11. [ Links ]
Bellavia, G., & Frone, M. (2005). Work-family conflict. In J. Barling, E.K. Kelloway, & M. Frone (Eds.), Handbook of work stress (pp. 113-147). Thousand Oaks, CA: Sage. [ Links ]
Brough, P., & O'Driscoll, M. (2005). Work-family conflict and stress. In A. Antoniou & C. Cooper (Eds.), A research companion to organizational health psychology (pp. 346-365). Cheltenham, UK: Edward Elgar. [ Links ]
Bruck, C.S., Allen, T.D., & Spector, P.E. (2002). The relation between work-family conflict and job satisfaction: A finer-grained analysis. Journal of Vocational Behavior, 60(3), 336-353. [ Links ]
Bryman, A., & Bell, E. (2003). Business research methods. Oxford, UK: Oxford University Press. [ Links ]
Byron, K. (2005). A meta-analytic review of work-family conflict and its antecedents. Journal of Vocational Behavior 67, 169-198. [ Links ]
Carlson, D.S., & Kacmar, K.M. (2000). Work-family conflict in organization: Do life role values make a difference? Journal of Management, 26, 1031-1054. [ Links ]
Carlson, D.S., Kacmar, K.M., & Williams, L.J. (2000). Construction and initial validation of a multidimensional measure of work-family conflict. Journal of Vocational Behavior, 56, 249-276. [ Links ]
Cooklin, A.R., Westrupp, E., Strazdins, L., Giallo, R., Martin, A., & Nicholson, J.M. (2014). Mothers' work-family conflict and enrichment: Associations with parenting quality and couple relationship. Journal of Child: Care, Health and Development. http://dx.doi.org/10.1111/cch.12137 [ Links ]
Cooper, C.L., Dewe, P.J., & O'Driscoll, M.P. (2001). Organizational stress: A review and critique of theory, research, and applications. Thousand Oaks, CA: Sage. [ Links ]
Cox, T., Griffiths, A. & Rial-Gonzalez, E. (2000). European Agency for Safety and Health at Work, Office for Official Publications of the European Communities, Belgium. [ Links ]
Deeromram, C., Suwannimitr, A., & Jundeekrayom, S. (2010). Mental health promotion among nursing students. Journal of Social Sciences, 6(2), 133-140. [ Links ]
Edwards, J., & Rothbard, N. (2000). Mechanisms linking work and family: Clarifying the relationship between work and family constructs. Academy of Management Review, 25(1), 178-199. [ Links ]
Farsi, Z., Dehghan-Nayeri, N., Negarandeh, R., & Broomand, S. (2010). Nursing profession in Iran: An overview of opportunities and challenges. Japan Journal of Nursing Science, 7, 9-18. http://dx.doi.org/10.1111/j.1742-7924.2010.00137.x [ Links ]
Frone, M. R. (2000). Work-family conflict and employee psychiatric disorders: The National Comorbidity Survey. Journal of Applied Psychology, 85(6), 888-895. [ Links ]
Frone, M.R. (2003). Work-family balance. In J.C. Quick & L.E. Tetrick (Eds.) Handbook of occupational health psychology (pp. 143-162). Washington, DC: American Psychological Association. [ Links ]
Frone, M.R., Russell, M., & Cooper, M.L. (1992). Antecedents and outcomes of work-family conflict: Testing a model of work-family interface. Journal of Applied Psychology, 77(1), 65-78. [ Links ]
Frone, M.R., Yardly, M., & Markel, K.S. (1997). Developing and testing a model of work-family interface. Journal of Vocational Behavior, 50, 146-167. [ Links ]
Gabrial, P., & Liimatainen, M.R. (2000). Mental health in the workplace. Geneva, Switzerland: International Labour Office. [ Links ]
Greenhaus, J., & Powell, G. (2003). When work and family collide: Deciding between competing role demands. Organizational Behavior and the Human Decision Processes, 90(2), 291-303. [ Links ]
Greenhaus, J.H., Allen, T.D., & Spector, P.E. (2006). Health consequences of work-family conflict: The dark side of the work-family interface. In P.L. Perrewe & D.C. Ganster (Eds.), Research in occupational stress and wellbeing (Vol. 5, pp. 61-98). Amsterdam: JAI Press. [ Links ]
Greenhaus, J.H., & Beutell, N.J. (1985). Sources of conflict between work and family roles. Academy of Management Review, 10, 76-88. [ Links ]
Grundemann, R.W, Nijboer, D., & Schellart, A.J. (1991). The work relatedness of drop out from work for medical reasons. Den Haag, Netherlands: Ministry of Social Affairs and Employment. [ Links ]
Grzywacz, J.G. (2000). Work-family spill over and health during midlife: Is managing conflict everything? American Journal of Health Promotion, 14(4), 236-243. [ Links ]
Grzywacz, J.G. (2003). Work, family and mental health: Testing different models of work-family fit. Journal of Marriage and Family, 65, 248-262. [ Links ]
Grzywacz, J.G., & Bass, B.L. (2003). Work, family, and mental health: Testing different models of work-family fit. Journal of Marriage and Family, 65, 248-262. [ Links ]
Grzywacz, J.G., & Fuqua, J. (2000). The social ecology of health: Leverage points and linkages. Behavioral Medicine, 26, 101-115. [ Links ]
Geurts, S.A.E., & Demerouti, E. (2003). Work/non-work interface: A review of theories and findings. In M.J. Schabracq, J.A.M. Winnubst, & C.L. Cooper (Eds.), The handbook of work and health psychology (pp. 279-312). Chichester, UK: Wiley. [ Links ]
Gutek, B.A., Searle, S., & Klepa, L. (1991). Rational versus gender role explanation of work-family conflict. Journal of Applied Psychology, 76, 560-568. [ Links ]
HashemiSheykh Shabani, S.E., Arshadi, N., & Bazrafkan, H. (2011). Structural analysis of work-family conflict regarding job satisfaction and mental health. Journal of Counseling and Family Therapy, 1(3), 349-365. [ Links ]
Kinnunen, U., Geurts, S., & Mauno, S. (2004). Work-family conflict and its relationship with satisfaction and well-being: A one year longitudinal study on gender differences. Work & Stress, 18(1), 1-22. [ Links ]
Kinnunen, U., Feldt, T., Geurts, S., & Pulkkinen, L. (2006). Types of work-family interface: Well-being correlates of negative and positive spillover between work and family. Scandinavian Journal of Psychology, 47(2), 149-162. http://dx.doi.org/10.1111/j.1467-9450.2006.00502.x [ Links ]
Klitzman, S., House, J.S., Israel, B.A., & Mero, R.P. (1990). Work stress, non-work stress, and health. Journal of Behavioral Medicine, 13, 221-243. [ Links ]
Krause, A.E. (2003). Work-family balance: The relationship between employment type, work-family conflict in women. Unpublished master's thesis, University of Witwatersrand, Johannesburg, South Africa. [ Links ]
HashemiNazari, S.S., Khosravi, J., FaghihZadeh, S., & EtemadZadeh, S.H. (2007). Investigating the mental health situation of fire organization employees using GHQ. Research Journal of Hakim, 10(2), 56-64. (In Persian) [ Links ]
Lembrechts, L., Dekocker, V., Zanoni, P., & Pulignano, V. (2015). A study of the determinants of work-to-family conflict among hospital nurses in Belgium. Journal of Nursing Management, 23, 898-909. http://dx.doi.org/10.1111/jonm.12233 [ Links ]
Madad, M. (2007). Statistical Center of Iran. Retrieved March 15, 2008, from http://www.sci.org.ir/portal/faces/public/census85 (in Persian) [ Links ]
McDermid, F., Peters, K., & Jackson, D. (2012). Factors contributing to the shortage of nurse faculty: A review of the literature. Nurse Education Today, 32(5), 565-569. [ Links ]
Mesmer-Magnus, J., & Viswesvaran, C. (2005). Convergence between measures of work-to-family and family-to-work conflict: A meta-analytic examination. Journal of Vocational Behavior, 67, 215-232. [ Links ]
Nikbakht Nasrabadi, A., Lipson, J.G., & Emami, A. (2004). Professional nursing in Iran: An overview of its historical and sociocultural framework. Journal of Professional Nursing, 20, 396-402. [ Links ]
Noor, N.M. (2003). Work- and family-role experiences, work-family conflict and women's well-being: Some observations. Community, Work and Family Journal, 6, 297-319. [ Links ]
O'Leary, L. (1993). Mental health at work. Occupational Health Review, 45, 23-26. [ Links ]
Oomens, S., Geurts, S., & Scheepers, P. (2007). Combining work and family in the Netherlands: Blessing or burden for one's mental health ? International Journal of Law and Psychiatry, 30, 369-384. [ Links ]
Pal, S.O., & Saksvik, P. (2008). Work-family conflict and psychosocial work environment stressors as predictors of job stress in a cross-cultural study. International Journal of Stress Management, 15(1), 22-42. [ Links ]
Quandt, S.A., & Arcury, T.A. (1997). Qualitative methods in arthritis research. Overview and data collection. Arthritis & Rheumatism, 10, 273-281. [ Links ]
Rajgopal, T. (2010). Mental well-being at the workplace. Indian Journal of Occupational and Environmental Medicine, 14(3), 66-70. [ Links ]
Rothbard, N. P., & Edwards, J. R. (2003). Investment in work and family roles: a test of identity and utilitarian motives. Personnel Psychology, 56(3), 699-729. http://dx.doi.org/10.1111/j.17446570.2003.tb00755.x [ Links ]
Rozanti, A., Mohd Amin, H., & Mohd Amin, S. (2014). Work-family conflict and work-family enrichment and their consequences in Malaysia. Middle-East Journal of Scientific Research, 19(5), 729-733. [ Links ]
Russell, H., O'Connell, P.J., & McGinnity, F. (2009). The impact of flexible working arrangements on work-life conflict and work pressure in Ireland. Gender, Work and Organization, 16(1), 73-97. [ Links ]
Sabokro, M., Baghbani, S., & Amiri, A.N. (2013). Work-family conflict: The role of organizational supportive perception in turnover intention: Case study of nurses of Tehran's hospitals. In V. Ribiere & L. Worasinchai (Eds.), Proceedings of the International Conference on Management, Leadership and Governance (pp. 282-288). Kidmore End, UK: Academic Conferences International Limited. [ Links ]
Staines, G., & O'Connor, P. (1980). Conflicts among work, leisure, and family roles. Monthly Labour Review, 103(8), 35-39. [ Links ]
Thomas, L.T., & Ganster, D.C. (1995). Impact of family-supportive work variables on work-family conflict and strain: A control perspective. Journal of Applied Psychology, 80, 6-15. [ Links ]
Ware, J. E., Jr., Kosinski, M., Turner-Bowker, D. M., & Gandeck, B. (2007). User's manual for the SF-12v2TM Health Survey (with a supplement documenting the SF-12® Health Survey). Lincoln, RI: QualityMetric Incorporated. [ Links ]
World Health Organization. (2008). Diabetes in the eastern Mediterranean region. Retrieved August 08, 2009, from http://www.emro.who.int/ncd/pdf/Diabetes_in_EMRO.pdf [ Links ]
 Correspondence:
Correspondence:
Morteza Charkhabi
morteza.charkhabi@univr.it
Received: 30 Dec. 2014
Accepted: 03 Nov. 2015
Published: 20 June 2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}