










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.18 no.1 Pretoria Mar. 2024
http://dx.doi.org/10.7196/SAJCH.2024.v18i1.1990
ARTICLE
Father absence at delivery at Pelonomi Tertiary Hospital in Bloemfontein: Reasons and associated demographic characteristics
J J van RooyenI; L de JagerII; S du PlessisII; J GoldbergII; J SalvageII; S SipikaII; G JoubertIII
IMB ChB, FCPaed (SA); Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIUndergraduate medical student at time of study; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIBA, MSc Department of Biostatistics, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND. The presence of fathers during the birth of their babies has been recognised as beneficial for both the mother and the baby.
OBJECTIVE. To investigate the reasons and demographic factors associated with father absence at delivery.
METHODS. We conducted a quantitative, cross-sectional study. Anonymous questionnaires were completed by mothers admitted to the postnatal ward at Pelonomi Tertiary Hospital in Bloemfontein, South Africa, after a live birth. Mothers answered questions regarding mother and father characteristics (age, employment, residence), whether the father was present or absent at delivery and the reasons for his absence.
RESULTS. The highest percentage (30.7%) of the 137 participating mothers was in the age range 20 - 25 years. More than half (56.2%) resided in Bloemfontein/Mangaung, and 70.6% were unemployed. Most mothers (68.4%) were multiparous. In total, 81.0% of fathers were absent at delivery, although 50.0% had planned to be at the delivery. The main reason for their absence was employment (52.7%), which can be substantiated by the fact that most fathers (80.3%) were employed. For more than half (58.1%) of the deliveries, neither the father nor any other person (family member or friend) was present at the delivery. There was no association between maternal or paternal demographics and father absence at delivery.
CONCLUSION. Father absence was common. Community-based programmes must encourage father involvement in all spheres of their children's lives and create awareness of the impact that their presence during birth can have.
The first 1 000 days of life have been identified as a critical time for optimal growth, learning and development.[1] The presence of fathers during their child's birth is recognised as beneficial for mother and baby.[2] Previously, labour was considered an event that did not require the father's presence.[2] However, this view has changed over the years, as the father's presence during labour has been reported to have a positive impact on the labour process and the health of the mother and the baby.[3] Almost all women in industrialised countries have their partners with them during birth, and evidence suggests that women prefer their partners to be present during labour.[4] During labour, the father's presence has been reported to decrease anxiety, labour hours, caesarean deliveries, improve maternal and foetal outcomes, strengthen the bond between the parents, as well as the bond between father and child. Furthermore, this process increases preparedness for fatherhood.[5]
Several factors may influence the presence or absence of a father at birth.[2] Research shows that a father's presence throughout pregnancy increases his willingness to be part of the birth process and present postpartum.[6] The father's absence may be instigated by fear of seeing their partner in pain and distress, a sense of feeling helpless, and not knowing how to comfort their partner during labour.[7] However, some fathers reported feeling excluded and unrecognised during the process.[7] Over the years, these factors have been improved significantly by midwives and nurses offering support and a sense of importance and gratitude to the father for being present.[8] This leads to a positive attitude from the father, which has been shown to psychologically and physiologically benefit the mother since, in most cases, the father's support helps the mother cope with pain. Severe labour pains may result in fetal distress, which is lowered in the father's presence.[9] A study conducted in Croatia[10] found that when husbands were present at delivery, mothers experienced shorter labour. There were fewer cases of intrauterine asphyxia and caesarean sections compared with mothers in the group whose husbands were not present. Existing literature shows that fathers who were absent at birth were also absent at follow-up intervals of 4, 12 and 24 months.[11]
Approximately 50% of South African (SA) children are living without daily contact with their fathers.[12] A study in Johannesburg found that contributors to father absence in an SA context included failure to pay traditional pre-marital payments to a bride's family (lobola and damages), as well as socioeconomic factors, e.g. paying for school fees and other tangible aspects of a child's life.'131 Other factors included ideas of masculinity and the relationship between the parents.[13] If the parents are separated or divorced, the father may be excluded from the family dynamic or allowed only specific time slots to visit the children.
It is essential to conduct research in other communities (including other provinces, cities, towns and districts) to identify and compare reasons for father absence, as these findings are important to influence and inform community programmes.[13] In research conducted abroad, factors identified for father absence included drug abuse, mental illness and violent behaviour.[14] Another study[15] identified labour migration and military service as factors contributing to absence.
Earlier research conducted by Shinn[16] in 1978 pointed to the possibility that the absence of fathers in single-parent families can lead to detrimental effects on children's cognitive development as assessed by standardised IQ and achievement tests and school performance. Studies have made it evident that the absence of fathers during the first year of a child's development has long-term negative consequences for the child.[1,171] The previous notion that the absence of fathers was insignificant has been challenged in many ways by available literature.[13] These include aspects pertaining to social, behavioural and academic development and the presence of a father figure.[13]
'Father-hunger', a term described by Herzog, is a child's need to have a tangible and emotional relationship with their father. It describes the child's feeling of distress or despair when the relationship is non-existent. 'Father hunger' and absence are evident and prevalent in SA.[18] One experimental study analysed IQs of socially disadvantaged premature African American babies at 3 years. It was found that when daily parental engagement occurred, higher IQs were predicted.'191 The National Survey of Children from the USA found that father involvement was positively linked to academic achievement in affluent families.[20] Lower academic achievement was observed in children whose fathers worked for the US military. This lack of achievement may be due to the stress of unique risks undertaken by their fathers.[15]
In low-income secure families, high father involvement was linked to low delinquency rates for males and females during early adulthood.[20] Father engagement lowered the risk of behavioural issues in boys and mental and emotional complications in girls.[19]
SA researchers found that children who had a present father in their household had a greater chance of having access to community resources as well as higher levels of household expenditure and increased protection.[13]
The presence of fathers during the first 1 000 days of development has positive effects on both child and father, where involvement in caregiving could influence a father's hormones and brain responses to infant stimuli.[21] The birth of a first child is a critical transition into fatherhood, where a smoother transition into this period could predict better involvement of fathers in subsequent years. However, this transition and involvement are influenced by many societal factors, such as expectations and opportunities, including paid parental leave.[21]
This study aimed to investigate whether fathers are present at their child's birth at Pelonomi Tertiary Hospital, Bloemfontein.
The objectives of the present study were to
• determine the mothers' and fathers' demographic information,
• investigate whether the fathers were present at the delivery,
• investigate reasons for fathers being absent at the delivery, and
• investigate associations between demographic characteristics and father absence at the birth.
Ethics
The protocol was approved by the Health Sciences Research Ethics Committee (HSREC), University of the Free State (ref no. UFS-HSD2018/0235/2509). As required by HSREC, implicit consent was given by the mothers when they chose to complete the anonymous questionnaire. Permission to conduct the study was obtained from the Free State Department of Health.
The hospital psychologist's details were provided to all mothers who agreed to participate in the study for consultation in cases where the questionnaire may have caused some discomfort, embarrassment, psychological stress, or harm to the mothers.
Methods
Study design, population and sampling
This was a quantitative, cross-sectional study. All mothers admitted to the postnatal ward at Pelonomi Tertiary Hospital, Bloemfontein, after a live delivery from 10 to 23 November 2018, were approached for participation. Both vaginal deliveries and caesarean sections were included as fathers are allowed to attend both modes of delivery at the hospital.
Mothers under the age of 20 years were excluded from this study owing to ethical concerns about the legal age of consent for sexual intercourse. Teenage mothers may also have had different experiences surrounding the birth and reasons for the fathers' absence compared with older mothers.
Illiterate mothers were not included owing to limited time for data collection and a lack of human resources.
Pelonomi Tertiary Hospital receives referrals from level 1 and 2 hospitals in central and southern Free State. The average number of live deliveries per month at Pelonomi Tertiary Hospital for January and February 2018 was 343.5, giving an average daily live delivery rate of 11.45. During the designated two-week period, it was estimated that ~168 live deliveries would occur.
Data collection
Anonymous and self-completed questionnaires were handed out to all mothers in the Pelonomi Tertiary Hospital postnatal ward who had a live delivery during the previous day or night. The questionnaire was available in English, Afrikaans and Sesotho. The questionnaires were handed out daily at 06h00 by the researchers, who were available to clarify any misunderstandings. No personal identifiers were recorded on any datasheets. Completed questionnaires were collected in a box on the same morning that they were handed out.
Pilot study
A pilot study was conducted on one day, during which 16 mothers completed the questionnaire. Issues with specific questions were identified and changed so that they could be interpreted unambiguously, thus increasing the reliability of the questionnaire. Data collected during the pilot study were excluded from the final data analysis.
Data analysis
Data were entered into a Microsoft Excel spreadsheet and analysed by the Department of Biostatistics, Faculty of Health Sciences, University of the Free State, using SAS (version 9.4; SAS Institute, USA). Results were summarised as frequencies and percentages. Associations were investigated using chi-squared or Fisher's exact tests.
Results
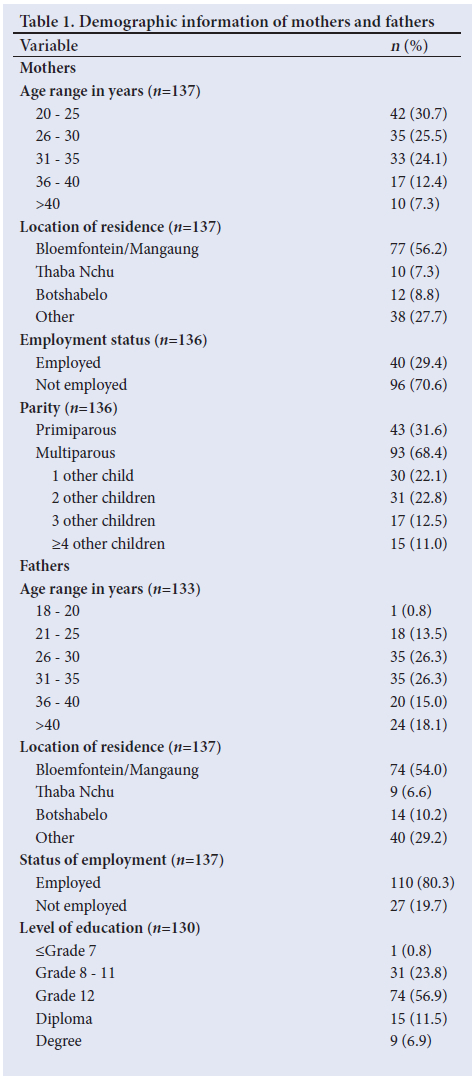
In total, 137 questionnaires were handed out and all were completed. All mothers reported that they knew their child's father. Table 1 summarises demographic information of the mothers and fathers. The highest percentage of mothers were in the 20 to 25 years age range (30.7%; n=42). More than half (56.2%; n=77) resided in Bloemfontein/ Mangaung and 70.6% (n=96) were unemployed. Most of the mothers (68.4%; n=93) were multiparous. The highest percentage of fathers were in the 26 to 30 years (26.3%; n=35) and 31 to 35 years (26.3%; n=35) age ranges. More than half (54.0%) of the fathers also resided in Bloemfontein/Mangaung and 80.3% (n=110) were employed. Most fathers (56.9%; n=74) had Grade 12 as their highest level of education.
One-third (30.9%; n=42) of the mothers had persons other than the father present at the birth, of whom 57.1% (n=24) were family members (Table 2).
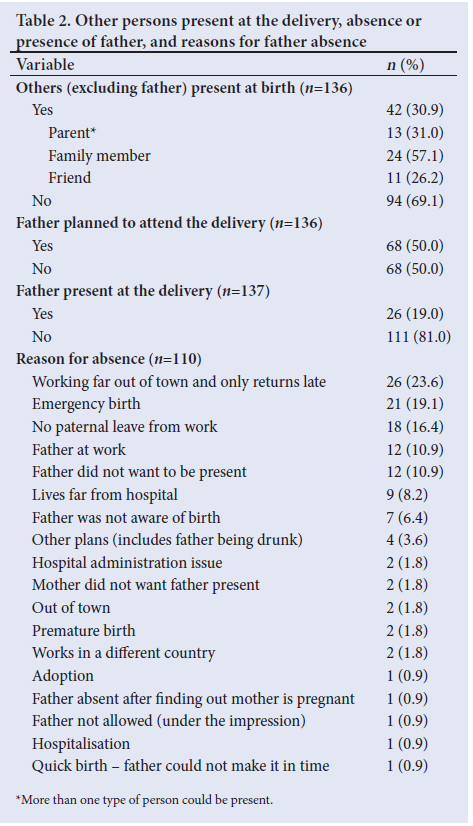
Half (50.0%) of the fathers had planned to attend the delivery, while only 19.0% were present. Of the 68 fathers who planned to attend the delivery, 33.8% were present. Of the 68 fathers who did not plan to attend the delivery, 4.4% were present (p<0.01).
The main reasons for the fathers' absence at delivery included the following: the father worked far out of town and returned late (23.6%); emergency birth (19.1%); and the father was unable to get paternal leave from work (16.4%). None of the fathers were absent owing to any of the following reasons: military service; father unknown; father in jail; illness; or father deceased.
In 79 of 136 deliveries (58.1%) for which the information was known, the mother was unaccompanied. Of the 110 cases where fathers were reported as absent, 28.2% (n=31) of the mothers reported someone else being present, compared with 42.3% of the 26 cases where the father was present (p=0.16).
Table 3 shows the association between the demographics of the parents and the fathers' absence or presence at birth.
There were no statistically significant differences for any of the mothers' demographic variables, including age, residence, employment and parity status, between the deliveries where the father was absent and the deliveries where the father was present. There were no statistically significant differences between the two groups' fathers' ages, residence, employment status and education level. There was a statistically significant difference between the two groups regarding planning to attend the delivery (p<0.01) (Table 3).
Discussion
Our findings indicate the absence of most fathers at the time of delivery for this study population investigated. Even if the father planned on attending the delivery, the vast majority of the fathers were not present. In a study[11] conducted in the USA, 231 fathers were questioned about their presence at the birth of their child.
All 31 fathers intended to be present at birth, but only 58% were eventually able to attend.
The most common reasons the fathers were absent at delivery in the current study included working out of town and returning home late, emergency birth and no paternal leave from work. Employment limits the possibility of a father's presence at the delivery. Shenk et al.[15] found that labour migration contributed to father absence in rural Bangladesh. Pelonomi Tertiary Hospital receives many complicated cases from other regional and district hospitals. In such cases, it may be difficult for the father to attend the delivery because of possible problems with transport, leave from work and the time of delivery. However, more than half (56.2%) of the women participating in our study were from Bloemfontein/Mangaung, where the hospital is situated.
Fathers living further away from the hospital may have been absent at delivery because emergency births complicate transport arrangements. In addition, healthcare services in the periphery may not be able to accommodate the fathers' needs at such short notice.
In 2013, a study in Johannesburg[13] indicated that many fathers leave town or leave the child's mother after birth. In our study, only one father was reported to have left the mother once he found out she was pregnant. The fathers' perspectives were reported in the Johannesburg study, whereas our study reported the mothers' perspectives. It was anticipated that some fathers might be absent because of customary cultural practices, but none of the participating mothers reported the father's absence because of cultural reasons. Similarly, no mothers indicated that the father of their child was unknown.
Most mothers were unaccompanied at delivery, which was indicative of a lack of support. At a community hospital in the Witwatersrand, the presence of a labour companion correlated strongly with positive effects during and after labour. These favourable outcomes included mothers having a higher self-esteem score, decreased levels of anxiety and postpartum depression 6 weeks after birth, while the mothers also felt that they coped well during labour.[22] In another SA study,[23] mothers supported throughout labour perceived that they had less labour pain.
In this study, almost a third of the mothers indicated that they were employed. According to a US study,[24] families with employed mothers had increased father involvement.
A study in England[25] found that multiparous women had a minor increased rate of father absenteeism at delivery compared with primiparous women. In our study, no association was found between the mother's parity and the father's absence. Although one might expect to see more fathers present when it is the mother's first child, it may not have been the father's first child. Socioeconomic and sociocultural factors may also have played a role in the difference in findings between the two studies.
Study limitations
All the results, including demographics and reasons for father absence, were gathered from the mothers' perspectives and did not include any of the fathers' opinions. A limited number of reasons for absence were accumulated owing to the data collection method. Personal interviews could have provided more detailed information on the reasons for the fathers' absence. The present study was conducted in a public hospital, limiting the population to a socioeconomic group that uses public healthcare services. Owing to the anonymity of the questionnaires and time and practical constraints, it was not possible to follow up on the fathers' presence at different intervals, e.g. at 6 and 12 months post birth. Our study was conducted before new legislation regarding paternal leave came into effect on 1 January 2020 in section 17 of the Labour Laws Amendment Act of 2018.[26]
Conclusion and recommendations
Many fathers in our cohort were absent at their child's delivery. The primary reasons for their absence was related to employment commitments. Demographic factors were not significantly associated with the fathers' absence or presence at delivery.
Larger-scale research should be conducted to determine the long-term presence of fathers through the life course of children to aid governmental education programmes surrounding father involvement and child development in SA. It is also important to conduct research based on the perspective of fathers to understand how they interpret their roles in the lives of their children. To improve the understanding of this issue, it would be required to include researchers familiar with customs and practices pertaining to child birth in particular settings and communities.
Fathers should be encouraged to attend antenatal clinic visits and classes to educate themselves on the birth process and the positive effects of their support of the mother during labour. If the father cannot attend the delivery, it may be suggested for the couple to arrange a companion. Antenatal programmes should encourage fathers to create a plan for the time leading up to the delivery so that they are prepared in terms of financing transport. Community programmes should educate fathers on their rights during the delivery, including paternal leave from work and being allowed to accompany the mother during labour. Employers should be made aware of the employees' rights during the time of pregnancy and around the time of delivery.
Declaration. This manuscript is based on the report by student authors LdJ, SdP, JG, JS and SS as a requirement of the MB ChB research modules.
Acknowledgements. The authors thank the mothers for their participation in this study, Dr Olive Khaliq (lecturer, Department of Paediatrics and Child Health, UFS) for finding and summarising additional literature, and Ms T Mulder, medical editor/writer, Faculty of Health Sciences, UFS, for technical and editorial preparation of the manuscript.
Author contributions. JJvR was the supervisor of this study, suggested the concept, assisted with the protocol development, interpretation of data and write-up of the study. LdJ, SdP, JG, JS and SS (undergraduate medical students at the time of the study, UFS), developed the protocol, collected data and wrote the first draft of the manuscript. GJ assisted with planning, performed data analysis and assisted with the interpretation and write-up of the article.
Funding. None.
Conflicts of interest. None.
References
1. Berg A. The importance of the first 1 000 days of life. J Child Adolesc Ment Health 2016;28(2):iii-vi. https://doi.org/10.2989/17280583.2016.1223803 [ Links ]
2. Ocho ON, Moorley C, Lootawan KA. Fathers' presence in the birth room - implications for professional practice in the Caribbean. Contemp Nurse 2018;54(6):617-629. https://doi.org/10.1080/10376178.2018.1552524 [ Links ]
3. Longworth MK, Furber C, Kirk S. A narrative review of fathers' involvement during labour and birth and their influence on decision-making. Midwifery 2015;31(9):844-857. https://doi.org/10.1016/j.midw.2015.06.004 [ Links ]
4. Dellmann T. 'The best moment of my life': A literature review of fathers' experience of childbirth. Aust Midwifery 2004;17(3):20-26. https://doi.org/10.1016/S1448-8272(04)80014-2 [ Links ]
5. Bowen SM, Miller BC. Paternal attachment behavior as related to presence at delivery and preparenthood classes: A pilot study. Nurs Res 1980;29(5):307-311. [ Links ]
6. Coutinho EC, Antunes JG, Duarte JC, Parreira VC, Chaves CM, Nelas PA. Benefits for the father from their involvement in the labour and birth sequence. Procedia Soc Behav Sci 2016;217(2016):435-442. https://doi.org/10.1016/j.sbspro.2016.02.010 [ Links ]
7. Vehviläinen-Julkunen K, Emelonye A. Spousal participation in labor and delivery in Nigeria. Ann Med Health Sci Res 2014;4(4):511-515. https://doi.org/10.4103/2141-9248.139290 [ Links ]
8. Kululanga LI, Sundby J, Malata A, Chirwa E. Striving to promote male involvement in maternal health care in rural and urban settings in Malawi - a qualitative study. Reprod Health 2011;8:36. https://doi.org/10.1186/1742-4755-8-36 [ Links ]
9. Austin MP, Leader L. Maternal stress and obstetric and infant outcomes: Epidemiological findings and neuroendocrine mechanisms. Aust N Z J Obstet Gynaecol 2000;40(3):331-337. https://doi.org/10.1111/j.1479-828x.2000.tb03344.x [ Links ]
10. Herman R, Hodek B, Ivicević-Bakulić T, Kosec V, Kraljević Z, Fures R. 'The effect of the presence of the husband during childbirthj. Lijec Vjesn 1997;119(8-9):231-232. [ Links ]
11. Bellamy JL, Thullen M, Hans S. Effect of low-income unmarried fathers' presence at birth on involvement. J Marriage Fam 2015;77(3):647-661. https://doi.org/10.1111/jomf.12193 [ Links ]
12. Holborn L, Eddy G. First Steps into Healing the South African Family. Johannesburg: South African Institute of Race Relations, 2011. [ Links ]
13. Mavungu EM. Provider expectations and father involvement: Learning from experiences of poor 'absent fathers' in Gauteng, South Africa. Afr Sociol Rev 2013;17(1):65-78. [ Links ]
14. Franséhn M, Bäck-Wiklund M. The presence of the absent father: How lone mothers with sons construct and animate the absent father through narratives. Eur J Soc Work 2008;11(4):369-381. https://doi.org/10.1080/13691450802075006 [ Links ]
15. Shenk MK, Starkweather K, Kress HC, Alam N. Does absence matter? A comparison of three types of father absence in rural Bangladesh. Hum Nat 2013;24(1):76-110. https://doi.org/10.1007/s12110-013-9160-5 [ Links ]
16. Shinn M. Father absence and children's cognitive development. Psychol Bull 1975;85(2):295-324. https://doi.org/10.1037/0033-2909.85.2.295 [ Links ]
17. Lamb ME, Pleck JH, Levine JA. The role of the father in child development: The effects of increased paternal involvement. In: Lahey BB, Kazdin AE, eds. Advances in Clinical Child Psychology. New York: Plenum, 1985:229-266. [ Links ]
18. Herzog J. Father hunger: Explorations with adults and children. Oxfordshire: Routledge, 2013. [ Links ]
19. Sarkadi A, Kristiansson R, Oberklaid F, Bremberg S. Fathers' involvement and children's developmental outcomes: A systematic review of longitudinal studies. Acta Paediatr 2008;97(2):153-158. https://doi.org/10.1111/j.1651-2227.2007.00572.x [ Links ]
20. Schlomer GL, Cho H-J. Genetic and environmental contributions to age at menarche: Interactive effects of father absence and LIN28B. Evol Hum Behav 2017;38(6):761-769. https://doi.org/10.1016/j.evolhumbehav.2017.06.002 [ Links ]
21. Bakermans-Kranenburg MJ, Lotz A, Alyousefi-van Dijk K, van IJzendoorn M. Birth of a father: Fathering in the first 1,000 days. Child Dev Perspect 2019;13(4):247-253. https://doi.org/10.1111/cdep.12347 [ Links ]
22. Wolman WL, Chalmers B, Hofmeyr GJ, Nikodem VC. Postpartum depression and companionship in the clinical birth environment: A randomised, controlled study. Am J Obstet Gynecol 1993;168(5):1388-1393. https://doi.org/10.1016/s0002-9378(11)90770-4 [ Links ]
23. Hofmeyr GJ, Nikodem VC, Wolman WL, Chalmers BE, Kramer T. Companionship to modify the clinical birth environment: Effects on progress and perceptions of labour, and breastfeeding. Br J Obstet Gynaecol 1991;98(8):756-764. https://doi.org/10.1111/j.1471-0528.1991.tb13479.x [ Links ]
24. Sandberg JF, Hofferth SL. Changes in children's time with parents: United States, 1981 - 1997. Demography 2001;38(3):423-436. https://doi.org/10.1353/dem.2001.0031 [ Links ]
25. Redshaw M, Henderson J. Fathers' engagement in pregnancy and childbirth: evidence from a national survey. BMC Pregnancy Childbirth 2013;13:70. https://doi.org/10.1186/1471-2393-13-70 [ Links ]
26. National Department of Labour, South Africa. Labour Laws Amendment Act, 2018 (Act No. 10 of 2018). Government Gazette No. 42925:1699. 2019. [ Links ]
 Correspondence:
Correspondence:
J J van Rooyen
VanRooyenJ1@ufs.ac.za
Accepted 28 September 2023


{kind=link}