










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.17 no.4 Pretoria Dez. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i4.1998
ARTICLE
Borderline hypernatraemia and mortality rates in South African infants: A single-centre observational study
N NakaI; F SolomonII, III; S A MadhiIV, V; A IzuIV, V; J M PettiforVI; Z DangorVIII; S.G LalaVII, VIII
IMMed (Paeds); Department of Paediatrics, Chris Hani Baragwanath Academic Hospital, and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMFamMed; South African Medical Research Council Vaccines and Infectious Diseases Analytical Unit, and Faculty of Health Sciences, University of the Witwatersrand, South Africa
IIIMFamMed; Department of Science and Technology/National Research Foundation: South African Research Chair in Vaccine Preventable Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVPhD; South African Medical Research Council Vaccines and Infectious Diseases Analytical Unit, and Faculty of Health Sciences, University of the Witwatersrand, South Africa
VPhD; Department of Science and Technology/National Research Foundation: South African Research Chair in Vaccine Preventable Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIPhD; Department of Paediatrics, Chris Hani Baragwanath Academic Hospital, and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIPhD; Perinatal HIV Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIIPhD; Paediatric Education and Research Ladder, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. In children, hypernatraemia occurs most commonly in infants (younger than 1 year). Although hypernatraemia is associated with high mortality and morbidity rates, it is variably defined in the paediatric literature as either serum sodium >150 mmol/L or serum sodium >145 mmol/L. In hospitalised adults, a serum sodium level >145 mmol/L but <150 mmol/L (called borderline hypernatraemia) has recently been identified as an independent risk factor for mortality. There are limited data about a potential association between borderline hypernatraemia and mortality in infants.
OBJECTIVES. To determine whether borderline hypernatraemia is associated with increased mortality in hospitalised infants.
METHODS. We conducted a single-centre, retrospective observational study of 8 343 infants admitted to a tertiary-level academic hospital in Johannesburg, South Africa, of whom 254 had borderline hypernatraemia, 376 had hypernatraemia (serum sodium >150 mmol/L), and 7 713 did not have hypernatraemia. Mortality rates were reported as odds ratios (ORs) with 95% confidence intervals (CIs).
RESULTS. In 254 infants with borderline hypernatraemia, 115 (45.3%) were neonates (<28 days old) and 140 (55.1%) were male. In 139 infants >28 days old with borderline hypernatraemia, the mortality rate (n=9/139; 6.5%) was significantly higher than the mortality rate observed in infants without hypernatraemia (n=194/5 857; 3.3%) (OR 2.02; 95% CI 1.03 - 3.98).
CONCLUSION. Borderline hypernatraemia may be a risk factor associated with higher mortality in hospitalised infants. Prospective studies are required to determine whether borderline hypernatraemia contributes independently to mortality risk in hospitalised infants.
Most paediatricians regard hypernatraemia as the most severe electrolyte abnormality that is associated with poor outcomes in hospitalised children. Although there are no clinical studies that assign a definitive contributory role for hypernatraemia in adverse childhood outcomes, high mortality (12 - 19%) and morbidity rates (50 - 55%) are reported in children with hypernatraemia.[5-7] In hospitalised children, hypernatraemia is most commonly detected in infants younger than 1 year of age.[1-8 However, hypernatraemia is generally uncommon; the best estimates suggest that it is present in 0.4% of hospitalised neonates and 0.04% in hospitalised infants.[9]
Hypernatraemia is further classified as community-acquired (i.e. present at the time of hospital admission) or hospital-acquired (i.e. hypernatraemia that develops during the infant's hospital stay). In hospitalised infants, community-acquired hypernatraemia is thought to develop as a result of reduced infant feeding in any of the following situations: an inability to establish breastfeeding; reduced appetite in infants with severe illness; diarrhoeal disease; and, uncommonly, secondary to the intake of hypertonic fluids.[1-8]
The current consensus view is that most adverse outcomes associated with hypernatraemia such as the development of cerebral oedema, intracerebral bleeds and death[5-13] develop as a consequence of overly rapid correction of serum sodium levels.[14] For paediatricians, the prompt recognition and appropriate treatment of hypernatraemia may therefore improve outcomes in infants with hypernatraemia. However, hypernatraemia is variably defined as either serum sodium >145 mmol/L,[14] or >150 mmol/L.[1-10] Furthermore, some investigators use the term borderline hypernatraemia (or mild hypernatraemia) to describe serum sodium levels >145 mmol/L but <150 mmol/L.[15] In hospitalised adults, several recent studies have shown that borderline hypernatraemia is an independent risk factor for mortality.[15-17] However, it is not known whether an association exists between borderline hypernatraemia and increased mortality in hospitalised infants, and we therefore undertook an observational study to test this hypothesis.
Ethics
Ethics approval for the study was obtained from the University of the Witwatersrand Human Research Ethics Committee (ref.no. M170672).
Methods
Study design and definitions
A retrospective study was undertaken to identify borderline community-acquired hypernatraemia in infants admitted to the Chris Hani Baragwanath Academic Hospital (CHBAH), Johannesburg, South Africa from 1 January 2015 to 31 December 2016. 'Borderline hypernatraemia' was defined as a serum sodium level >145 mmol/L but <150 mmol/L.[15] 'Definite hypernatraemia' was defined as serum sodium >150 mmol/L and 'community-acquired hypernatraemia' referred to the development of hypernatraemia prior to hospital admission.[18] Infants in the first 28 days of life were regarded as neonates, and infants beyond the neonatal period were older than 28 and younger than 365 days old.
Blood collection
At CHBAH, if indicated, clinicians obtain blood for testing immediately after clinical evaluation and prior to intravenous fluid or medical therapy. Serum sodium levels are measured by indirect ion-selective electrodes at the CHBAH National Health Laboratory Service (NHLS); the NHLS complies with the International Organization for Standardization requirements (ISO/ IEC 17043:2010) for serum electrolyte measurement and the normal serum sodium level reference range is 136 - 145 mmol/L.
Patient selection: Inclusion and exclusion criteria
Demographic, clinical and laboratory data were obtained by reconciling data from two electronic databases: (i) the NHLS Track-Care database, which records sodium results; and (ii) the Respiratory and Meningeal Pathogens Research Unit (RMPRU) administrative database which records all paediatric hospital admissions and outcomes.[19] After identifying infants with admission serum sodium values >145 mmol/L from the NHLS database, the following corresponding variables were extracted from the RMPRU database: age; gender; anthropometric parameters; HIV status; main or primary discharge diagnosis (as defined by an ICD-10 code); and outcome (death or discharge). In neonates, hypernatraemic cases were exclusively categorised according to one of the following most-coded primary diagnoses: (i) neonatal infection (representing either neonatal sepsis or possible serious bacterial infection); and (ii) neonatal jaundice (NNJ). All remaining neonatal cases without the aforementioned primary diagnoses were categorised as 'other neonatal diagnoses'. In infants beyond the neonatal period, hypernatraemic cases were exclusively categorised according to one ofthe following most-coded primary diagnoses: (i) acute gastroenteritis; (ii) lower respiratory tract infection; and (iii) other infant infections. All remaining cases without the aforementioned primary diagnoses were categorised as 'other infant diagnoses'. The following cases were excluded from the present study: (i) children with hospital-acquired hypernatraemia; (ii) those with underlying medical conditions predisposing to hypernatraemia, i.e. abnormalities of the central nervous system, meningitis, diabetes mellitus or diabetes insipidus, accidental ingestion of poisons or medication, and renal disease; and (iii) neonates who were admitted directly to the neonatal unit after birth, i.e. predominantly premature neonates and term neonates requiring immediate hospitalisation after birth. We used the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) criteria to account for missing data.[21]
Statistical analysis
The prevalence of community-acquired hypernatraemia in hospitalised infants was determined as a proportion of the total number of infant admissions. Anthropometric z-scores, based on the World Health Organization (WHO) growth references, were calculated using WHO AnthroPlus software V.1.0.4. Comparisons of mortality between infants with borderline hypernatraemia, no hypernatraemia, and definite hypernatraemia were undertaken using contingency tables. Analyses were performed using either the Chi-square or Fischer's exact test - p-values, odds ratios (ORs) and 95% confidence intervals (CIs) were reported. Data were analysed using STATA software (version 13.0; Stata Corp., USA).
Results
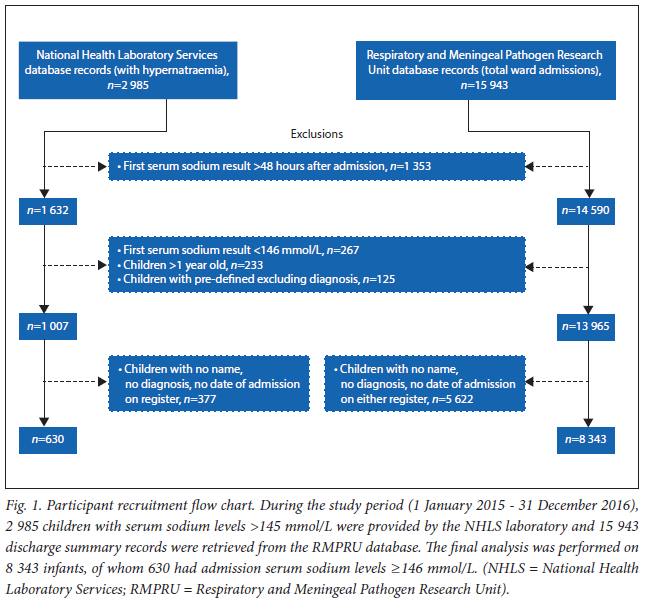
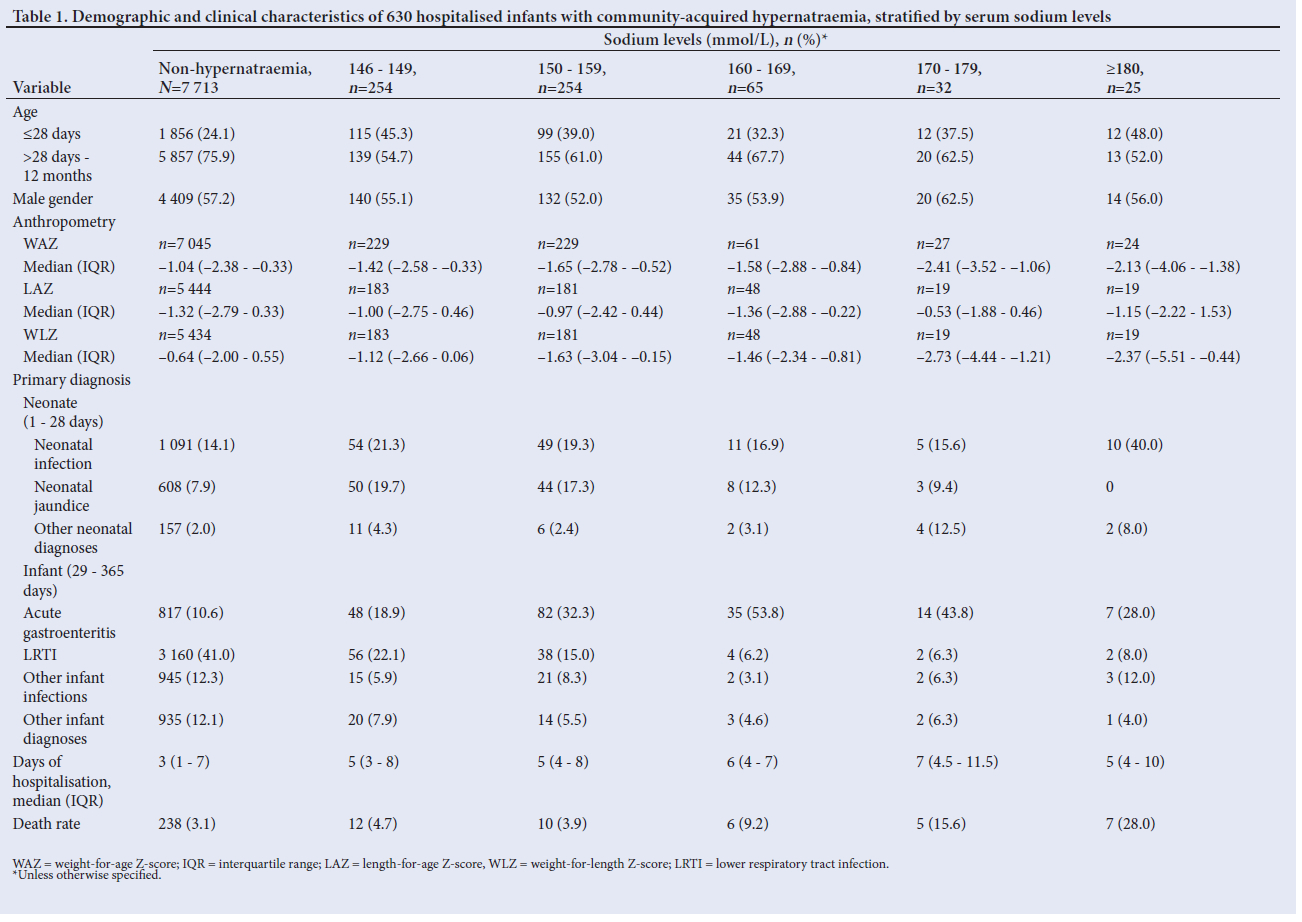
For the study period, 15 943 discharge summary records were retrieved from the RMPRU database and 2 985 results of children with serum sodium levels >145 mmol/L were provided by the NHLS laboratory . These databases were reconciled, and 8 343 infants were analysed (Fig. 1). Of 8 343 hospitalised infants, 254 (3.0%) had borderline hypernatraemia (Table 1). In infants with borderline hypernatraemia, 115 (45.3%) were neonates (<28 days of age) and 140 (55.1%) were male. In neonates with borderline hypernatraemia, the most common diagnoses were neonatal infections (n=54; 47.0%) and jaundice (n=50; 43.5%). In infants beyond the neonatal period (n=139), the most common diagnoses were lower respiratory tract infection (n=56; 40.3%) and acute gastroenteritis (n=48; 34.5%).
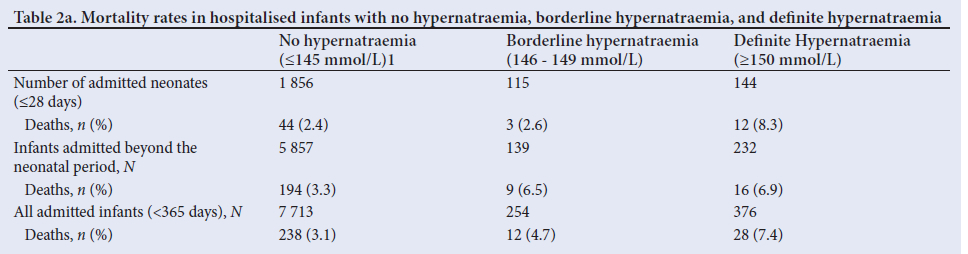
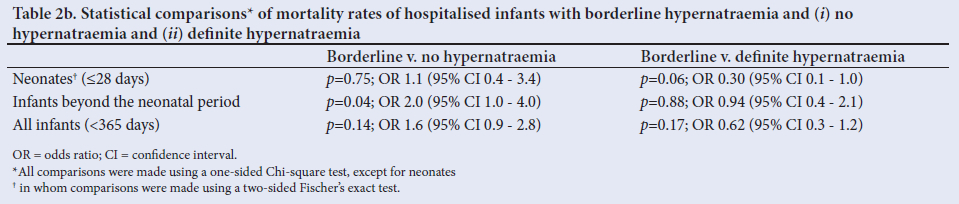
In neonates with borderline hypernatraemia, the mortality rate was 2.6% (n=3/115 cases). This mortality rate was comparable with neonates without hypernatraemia (2.4%; n=44/1 856; OR 1.10; 95% CI 0.36 - 3.41) but lower than the mortality rate in neonates with definite hypernatraemia (8.3%; n=12/144; OR 0.3; 95% CI 0.1 - 1.0) albeit not statistically significant (Tables 2a and 2b). In infants beyond the neonatal period, the odds of mortality were twice as high in infants with borderline hypernatraemia compared with infants without hypernatraemia (OR 2.0; 95% CI 1.0 - 4.0); mortality rates were similar in infants with borderline hypernatraemia (6.5%; n=9/139) and definite hypernatraemia (6.9%, n=16/232; OR 0.9; 95% CI 0.4 - 2.1).
Discussion
Our study shows that borderline hypernatraemia (serum sodium >145 mmol/L but <150 mmol/L) in hospitalised infants beyond the neonatal period is associated with higher mortality; this is in keeping with results showing an association between borderline hypernatraemia and mortality in adults.[14-16] Borderline hypernatraemia (serum sodium >145 mmol/L) was present in a significant proportion (40.3%) of all hypernatraemic cases. In our study, mortality rates were higher in infants with severe hypernatraemia - a trend described in other studies.[4-6,10] In our resource-limited setting, the overall mortality rate in hypernatraemic infants was high; we speculate that this could be due to: (i) lack of close monitoring of the rate at which intravenous fluids are administered; (ii) liberal prescription of fluid boluses and high infusate volumes to children presenting with sepsis or a 'sepsis-like' illness;[22] and (iii) difficulty in obtaining results timeously from our medical laboratory.
Study limitations
We cannot attribute a direct causal role implicating borderline hypernatraemia and mortality; the relatively low numbers (in comparison to adult studies) did not allow us to adjust for confounding variables that contribute independently to mortality, e.g. underlying diagnosis, duration of illness, nutritional status, as well as the rate and volume of intravenous fluid therapy. Compared with non-hypernatraemic infants, proportionately more children with hypernatraemia were underweight or had wasting; however, because admission weights are not a true reflection of the actual weight in dehydrated children, we cannot reliably infer potential associations with hypernatraemia. HIV-infected children may be at risk of hypernatraemia but we could not verify this association because of the small number of HIV-infected children in our study. In the present study, HIV-exposure is more reliably determined in under-6-month-olds, and in this group we did not find an association between HIV-exposure and case fatality rates (data not shown). We did not show a significantly higher mortality rate in neonates with borderline hypernatraemia but other investigators have reported lower fine motor scores (during later developmental assessments) in preterm infants whose serum sodium levels exceeded 145 mmol/L in the first week of life.[23]
Conclusion
Despite the limitations of an observational study, we analysed outcomes in a very large number of infants, and in keeping with adult findings, we found a significant association between borderline hypernatraemia and increased mortality in hospitalised infants. Borderline hypernatraemia may be a risk factor for increased mortality in hospitalised infants and we suggest that hypernatraemia in children be defined as serum sodium levels of >145 mmol/L rather than >150 mmol/L. Until evidence-based treatment guidelines are available, we recommend that clinicians avoid overly rapid correction of the serum sodium levels using intravascular fluids in infants with borderline hypernatraemia.
Declaration. This manuscript was submitted in partial fulfilment of the criteria for NN's MMed (Paeds) degree at the University of the Witwatersrand
Acknowledgements. None.
Author contributions. ZD and SGL: conceptualised and designed study; designed data collection instruments; analysed data, reviewed and revised manuscript (equal contributions). NN: designed data collection instruments, collected data and carried out initial analysis, drafted initial manuscript, reviewed and revised manuscript. FS, AI and SAM: maintained database employed in the study, critically reviewed the manuscript for important intellectual content. JMP: assisted with the study design and analysis, critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding. None.
Conflicts of interest. None.
References
1. Finberg L. Hypernatremic (hypertonic) dehydration in infants. N Engl J Med 1973;289(4):196-198. https://doi.org/10.1056/NEJM197307262890407 [ Links ]
2. Colle E, Ayoub E, Raile R. Hypertonic dehydration (hypernatremia): The role of feeding high in solutes. Pediatrics 1958;22:5-12. [ Links ]
3. Koklu E, Gunes T, Ozturk MA, Kose M, Kurtoglu S, Yuksel F. A review of 116 cases of breastfeeding-associated hypernatremia in rural area of central Turkey. J Trop Pediatr 2007;53(5):347-350. https://doi.org/10.1093/tropej/fmm026 [ Links ]
4. Ben-Shalom E, Toker O, Schwartz S. Hypernatremic dehydration in young children: Is there a solution? Isr Med Assoc J 2016;18:95-99. [ Links ]
5. Chisti MJ, Ahmed T, Ahmed AM, et al. Hypernatremia in children with diarrhea: Presenting features, management, outcome, and risk factors for death. Clin Pediatr 2016;55(7):654-663. https://doi.org/10.1177/0009922815627346 [ Links ]
6. Shahrin L, Chisti MJ, Huq S, et al. clinical manifestations of hyponatremia and hypernatremia in under-five diarrheal children in a diarrhea hospital. J Trop Pediatr 2016;62(3):206-212. https://doi.org/10.1093/tropej/fmv100 [ Links ]
7. Moritz M, Ayus J. The changing pattern of hypernatremia in hospitalised children. Pediatrics 1999;104(X):435-439. https://doi.org/10.1542/peds.104.3.435 [ Links ]
8. Moritz M, Manole M, Bogen D, Ayus JC. Breastfeeding-associated hypernatremia: Are we missing the diagnosis? Pediatrics 2005;116:e343-e347.https://doi.org/10.1542/peds.2004-2647 [ Links ]
9. Baumer JH, Coulthard M, Haycock G, McIntosh N, Ranmal R, Haines L. The Differential Diagnosis of Hypernatraemia in Children, with Particular Reference to Salt Poisoning. An evidence-based guideline. London: Royal College of Paediatrics and Child Health, 2009. [ Links ]
10. Fang C, Mao J, Dai Y, Xia Y, Fu H, Chen Y, et al. Fluid management of hypernatremic dehydration to prevent cerebral oedema: A retrospective case control study of 97 children in China. J Paediatr Child Health 2010;46(6):301-303. https://doi.org/10.1111/j.1440-1754.2010.01712.x [ Links ]
11. Ergenekon E, Unal S, Gücüyener K, et al. Hypernatremia in the newborn period and long-term follow up. Pediatr Int 2007;49(1):19-23. https://doi.org/10.1111/j.1442-200X.2007.02313.x [ Links ]
12. Boskabadi H, Akhondian J, Afarideh M, et al. Long-term neurodevelopmental outcome of neonates with hypernatremia. Breastfeed Med 2017;12:163-168. https://doi.org/10.1089/bfm.2016.0054 [ Links ]
13. Heydarian F, Rezaeian A. Relationship between changes in serum sodium level and seizures occurrence in children with hypernatremia. Iran J Child Neurol 2013;7(4):35-40. [ Links ]
14. Greenbaum LA. Deficit therapy. In: Kliegman RM, St Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. Philadelphia: Elsevier, 2020:429-432.e1. [ Links ]
15. Girardeau Y, Jannot AS, Chatellier G, Saint-Jean O. Association between borderline dysnatremia and mortality insight into a new data mining approach. BMC Med Inform Decis Mak 2017;17(1):152. https://doi.org/10.1186/s12911-017-0549-7 [ Links ]
16. Thongprayoon C, Cheungpasitporn W, Yap JQ, Qian Q. Increased mortality risk associated with serum sodium variations and borderline hypo- and hypernatremia in hospitalised adults. Nephrol Dial Transplant 2020;35(10):1746-1752. https://doi.org/10.1093/ndt/gfz098 [ Links ]
17. Darmon M, Diconne E, Souweine B, et al. Prognostic consequences of borderline dysnatremia: Pay attention to minimal serum sodium change. Crit Care 2013;17(1):R12. https://doi.org/10.1186/cc11937 [ Links ]
18. Jung WJ, Lee HJ, Park S, et al. Severity of community acquired hypernatremia is an independent predictor of mortality. Intern Emerg Med 2017;12(7):935-940. https://doi.org/10.1007/s11739-017-1673-1 [ Links ]
19. The Human Sciences Research Council (HSRC) Economic Performance and Development Programme (EPD). The City of Johannesburg (COJ) Economic Overview: 2013. A Review of the State of the Economy and other Key Indicators. Pretoria: HSRC, 2013. http://www.hsrc.ac.za/uploads/pageContent/4974/HSRC%20COJ%20ECONOMIC%20OVERVIEW%202013%20_Report.pdf (accessed 29 May 2020). [ Links ]
20. Singh S, Solomon F, Madhi SA, Dangor Z, Lala SG. An evaluation of the quality of discharge summaries from the general pediatric wards at Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa. S Afr Med J 2018;108(11):953-956. https://doi.org/10.7196/SAMJ.2018.v108i11.12966 [ Links ]
21. Von Elm E, Altman DG, Egger M, Pocock SJ, G0tzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med 2007;4(10):e296. https://doi.org/10.1371/journal.pmed.0040296 [ Links ]
22. Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2016. Intensive Care Med 2017;43(3):304-377. https://doi.org/10.1007/s00134-017-4683-6 [ Links ]
23. Howell HB, Lin M, Zaccario M, et al. The impact of hypernatremia in preterm infants on neurodevelopmental outcome at 18 months of corrected age. Am J Perinatol 2020;39(5):532-538. https://doi.org/10.1055/s-0040-1716845 [ Links ]
 Correspondence:
Correspondence:
S G Lala
sanjay.lala@wits.ac.za
Accepted 16 November 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}