










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.4 Pretoria Dec. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i4.1922
ARTICLE
The impact of hypothermia in a tertiary hospital neonatal unit
R M TshehlaI; M CoetzeeII; J BeckerIII
IFCPaed(SA), MMed(Paed); Division of Neonatology, Department of Paediatrics and Child Health, Steve Biko Academic Hospital and Faculty of Health Sciences, University of Pretoria, South Africa
IIMMed(Paed), MPhil (Neonatology); Division of Neonatology, Department of Paediatrics and Child Health, Steve Biko Academic Hospital and Faculty of Health Sciences, University of Pretoria, South Africa
IIIMSc, PhD Research Office, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Neonatal hypothermia, defined as a body temperature <36.5°C, is a known contributor to neonatal morbidity and mortality. The admission temperature is an important predictor of neonatal outcomes, and a measure of quality of care.
OBJECTIVES: This study aims to determine the incidence of and factors associated with hypothermia on admission to the neonatal unit at Steve Biko Academic Hospital (SBAH), a public tertiary hospital in South Africa.
METHODS: A retrospective, cross-sectional study of infants admitted to the neonatal unit from September 2019 to February 2020 using data from patient records.
RESULTS: The overall incidence of hypothermia on admission was 66% (mild 25%, moderate to severe 41%), with a mean (standard deviation (SD)) admission temperature of 35.1 (4.7)°C, and 82% (mild 19%, moderate to severe 62%) in very-low-birthweight infants. Infants remained hypothermic for a mean (SD) of 4.1 (3.9) hours post admission. Birthweight <1 500 g (odds ratio (OR) 1.87; p=0.019), admission to the neonatal intensive care unit (OR 1.97; p<0.0001), and admission from the delivery room within the first 60 minutes of life (OR 3.06; p=0.026) were independent risk factors for hypothermia. Hypothermia was associated with increased duration of respiratory support (mean 3.2 (5.6) v. 1.7 (4.5) days; p<0.0001), and longer length of hospital stay (mean 17.9 (18.8) v. 10.9 (12.6) days; p<0.0001).
CONCLUSION: The incidence of hypothermia on admission to the unit is significantly high, and hypothermic infants take a significant length of time to regain normothermia. A standardised protocol for the prevention and management of hypothermia needs to be introduced in the unit.
Neonatal hypothermia is defined as a body temperature <36.5°C. The World Health Organization (WHO) classifies it into three grades of severity: mild (36.0 - 36.4°C), moderate (32.0 - 35.9°C), and severe (<32.0°C).[1] The incidence of neonatal hypothermia varies widely. The adoption of strategies to prevent hypothermia has led to a decrease in its incidence. Data from the Vermont Oxford Network showed an improvement in hypothermia on admission of very-low-birthweight (VLBW) infants from 52.6% in 2009, to 38.5% in 2016.[2] However, the incidence remains significantly high in low-resource settings.[3,4]
The admission temperature is an important predictor of neonatal outcomes, as well as a measure of quality of care.[5,6] Neonatal hypothermia is an independent risk factor for neonatal death, and is associated with neonatal morbidities and a prolonged hospital stay.[4,7-12] The reported case-fatality rate globally ranges from 8.8% to 52%.[13] The risk of mortality is significantly higher in preterm and VLBW infants.[8,11,12]
The risk of mortality increases with the severity of hypothermia. A European study found a 15% decrease in mortality for every 1°C increase in admission temperature in VLBW infants.[12] A large community-based study in Nepal reported a 75% increase in the risk of death for every 1°C decrease in temperature, with the risk of death increasing 1.46 and 3.12 times in infants with mild and moderate hypothermia, respectively.[11]
A study conducted at the Steve Biko Academic Hospital (SBAH), Pretoria, in 2017 on the morbidity and mortality of VLBW and extremely-low-birthweight (ELBW) infants found a high incidence of hypothermia, with over three-quarters of the infants being hypothermic on admission.[14] This prompted a need for more comprehensive study into the incidence and impact of hypothermia in the unit. The aim of this study was to determine the incidence of and risk factors for hypothermia on admission to the neonatal unit, and its impact on neonatal outcomes.
Methods
Study design and setting
This retrospective, cross-sectional study was done at the SBAH, a tertiary academic public hospital in South Africa. Data were collected from patient records of infants admitted to the SBAH neonatal unit from 1 September 2019 to 29 February 2020.
Study population
All infants admitted to the neonatal unit in the first 28 days of life were included in the study, including those born at another facility and transferred into the unit. Infants with hyperthermia (temperature >37.5°C) on admission were excluded. Infants admitted for therapeutic hypothermia were also excluded as it could not be determined whether they may have undergone passive cooling during the admission period. Infants with an expected poor outcome who were admitted for palliative care were included in the analysis of the incidence of hypothermia as they would be expected to receive the same thermal care as other infants. However, they were excluded from the analysis of risk factors and outcomes related to hypothermia. These included: infants with severe congenital or chromosomal abnormalities, and infants with a birthweight <750 g who did not receive active management.
Study procedure and analysis
Infants admitted to the neonatal unit during the specified period were identified using the ward admission statistics and data were collected from patient records. Blood culture results were accessed from the National Health Laboratory Service (NHLS) database, and cranial ultrasound reports were accessed on the hospital's computerised radiology system (XeroViewer).
During the study period, infants had their temperature recorded on admission, then every 2 hours in the neonatal intensive care unit (NICU), or every 3 hours in the high-care ward. The body temperatures were recorded using a temperature skin probe (minimum temperature 35.0°C), a disposable thermometer strip (minimum temperature 35.5°C), or digital thermometers with variable minimum readings. For this reason, temperatures below 35°C could not be accurately stratified and data were summarised into normal, mild, and moderate-to-severe hypothermia. Infants were classified based on the temperature recorded on admission. For infants with a subnormal temperature, the first subsequent normal temperature was used to determine the length of time taken to achieve normothermia at admission.
The incidence of hypothermia was assessed both as a binary outcome (present/absent) and as a multinomial outcome (absent, mild, and moderate-severe). A sample size of 400 neonates was estimated to assess the incidence as a binary outcome with 95% confidence to an accuracy within 0.05, when assuming a conservative scenario of an expected incidence of 0.5 (50%). A 6-month study period was therefore selected, based on expected number of admissions, allowing for missing patient records. When considered as a multinomial outcome, this sample would achieve a probability of at least 0.9 that the estimates of the multinomial proportions are within 0.05 of the population proportions. The sample size was also estimated to be adequate for the logistic/polytomous logistic regression analyses to determine factors associated with hypothermia (binary and multinomial) and the associations of hypothermia with neonatal outcomes. The pairwise comparisons were done using the Bonferroni adjustment. Testing was done at the 0.05 level of significance.
Definitions
Hypothermia was defined as a body temperature <36.5°C and classified according to the WHO definition: mild (36.0°C - 36.4°C), moderate (32.0°C - 35.9°C), and severe (<32.0°C).
Resuscitation at birth was defined as needing any intervention beyond routine neonatal care, including supplemental oxygen, positive-pressure ventilation, cardiac compressions, and the administration of adrenaline. Respiratory support was defined as invasive (mechanical ventilation) or non-invasive ventilation (nasal continuous positive airway pressure (nCPAP)), while days on oxygen were counted when infants received oxygen supplementation with respiratory support and/or via nasal canula.
Late-onset sepsis was defined as sepsis after 72 hours of life and subdivided into culture-proven and suspected sepsis (based on information in the patient record and laboratory findings). Hypoglycaemia was defined as a blood glucose <2.6 mmol/L on capillary blood glucose measurements and was assessed in the first 24 hours after admission. Intraventricular haemorrhage (IVH) was diagnosed on cranial ultrasound performed by a trained sonographer.
Ethics approval for this research was obtained from the Faculty of Health Sciences' Research Ethics Committee of the University of Pretoria (ref. no. 558/2020).
Results
Study cohort
There were 579 infants admitted to the neonatal unit between 1 September 2019 and 29 February 2020. A total of 77 infants were excluded from the study for the following reasons: missing patient records (n=36), no admission temperature found in the patient records (n=15) (this was in part due to incomplete patient records being retrieved), hyperthermia (n=5), infants admitted for therapeutic hypothermia (n=19), and infants admitted after 28 days of life (n=2). A total of 502 infants were included in the study. Seven infants were admitted for comfort care and were only included in the analysis of the incidence of hypothermia.
Infant and maternal characteristics
The mean (standard deviation (SD)) birthweight was 2 105 (863) g (range 602 - 5 380 g), and the mean (SD) gestation age was 34 (3.8) weeks (range 25 - 42 weeks). Most (348; 69%) were low-birthweight (LBW) infants, of whom 130 (26%) were VLBW infants, and 31% had a birthweight >2 500 g. The majority of infants were inborn (n=415; 83%), and most of the outborn infants (n=64; 85%) were transferred from facilities with a distance of <40 km from the hospital. Most infants (n=451; 90%) were admitted in the first 24 hours of life. Approximately half of the outborn infants (n=36; 49%) were admitted beyond the first day of life. Only 8 (10%) of the outborn infants were VLBW. Ten infants (2%) were born at home or in transit to hospital.
The mean (SD) maternal age was 28 (6.2) years (range 13 - 46 years). Half of the mothers had medical and/or pregnancy-related conditions. Only 60% received a complete course of antenatal corticosteroids when indicated (preterm delivery before 34 weeks' gestation). Most deliveries occurred by emergency caesarean section (n=278; 56%). Approximately one-third of infants required resuscitation or interventions in the delivery room above routine newborn care.
Incidence of hypothermia on admission
The incidence of hypothermia on admission in the study cohort was 67% (n=336). A quarter of infants had mild hypothermia (n=129) and 41% (n=207) had moderate-severe hypothermia. Five infants (1%) had hyperthermia (temperature >37.5°C). One in 10 infants had an admission temperature <35.0°C. Hypothermia on admission was present in 82% of VLBW infants (n=106), with 62% (n=81) having moderate-severe hypothermia and 25% (n=33) having an admission temperature <35.0°C. The first subsequent normal temperature was recorded at a mean of 4.1 (3.9) hours (range 2 - 36 hours) after an initial subnormal temperature recording on admission.
Risk factors for hypothermia
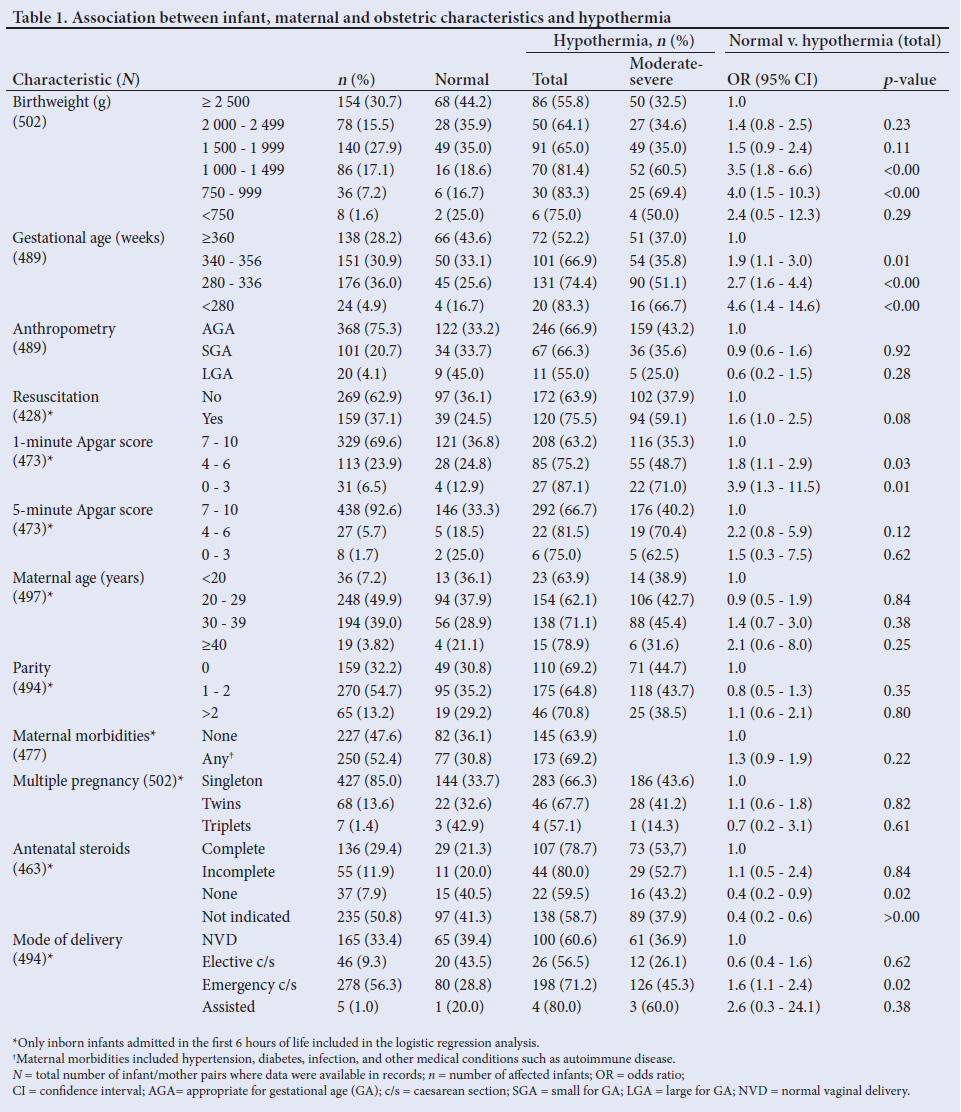
Birthweight was a significant risk factor for hypothermia on admission. The odds of hypothermia increased with decreasing birthweight and gestational age (Table 1). VLBW infants had 2 - 4 times increased odds of becoming hypothermic compared with infants with a birthweight >2 500 g. Infants with a gestation of 340-366 weeks, 280-336 weeks, and <280 weeks were 2, 3, and 5 times more likely to be hypothermic than infants with a gestational age >366 weeks."
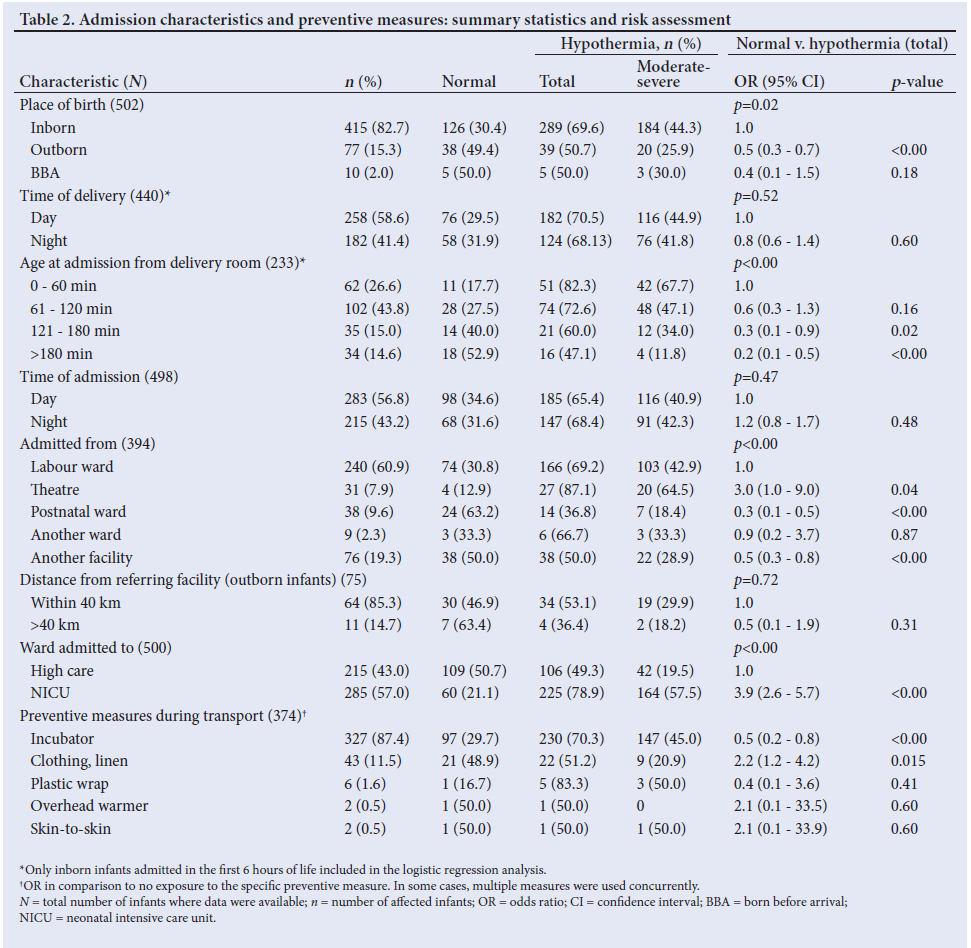
Outborn infants were less likely to be hypothermic on admission than inborn infants (odds ratio (OR) 0.45; 95% confidence interval (CI) 0.3 - 0.7). Among inborn infants, admission directly from theatre (OR 3.01; 95% CI 1.0 - 9.0), and delivery by emergency caesarean section (OR 1.61; 95% CI 1.1 - 2.4) were associated with increased risk for hypothermia. Receiving resuscitation in the delivery room did not significantly increase the risk of hypothermia (OR 1.6; 95% CI 1.0 - 2.5). However, infants who were hypothermic on admission had significantly lower Apgar scores at 1 minute than those who had a normal temperature (mean Apgar 8.5 v. 6.5; p<0.00). Hypothermia was more common in infants admitted to the NICU compared with those admitted to high care (OR 3.9; 95% CI 2.6 - 5.7). On multivariate analysis, the following were independent risk factors for hypothermia in this cohort: birthweight <1 500 g (OR 1.9; p=0.02), admission to NICU (OR 2.0; p<0.00), and admission from the delivery room within the first 60 minutes of life (OR 3.06; p=0.03).
Mothers of hypothermic infants were significantly older than mothers of normothermic infants (mean (SD) 29 (6.3) years v. 27 (5.6) years; p=0.04). Other maternal factors, anthropometry, time of delivery or admission (day or night), and distance from referring facility did not significantly affect the risk for hypothermia.
Owing to a shortage of beds, infants are occasionally nursed in a warmed incubator in the labour ward while awaiting admission to the neonatal unit. This includes infants delivered in theatre and the labour ward itself, as well as those born before arrival to hospital. There was a higher incidence and degree of severity of hypothermia on admission among inborn infants who arrived in the neonatal unit in the first 60 minutes of life (Table 2).
The majority of infants (87%) were transferred in closed incubators. However, 12 LBW (<2 500 g) infants, including 6 VLBW infants, were transferred wrapped in linen only without additional preventive measures. Only 8% of VLBW infants, and 15% of ELBW infants were wrapped in plastic. Being transferred in a closed incubator was the only intervention that significantly decreased the risk of hypothermia in all infants (OR 0.5; 95% CI 0.2 - 0.8). Infants who were transported covered in linen and/or clothed, without the use of additional preventive measures, such as plastic wrap or additional heat source, had a twofold increased risk of hypothermia (OR 2.2; 95% CI 1.2 - 4.2) (Table 2).
Hypothermia and neonatal outcomes
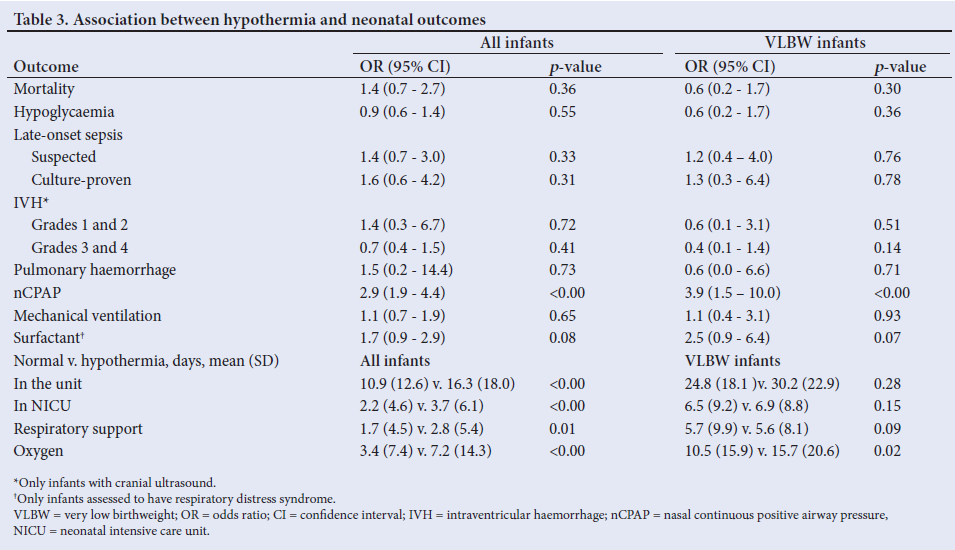
Hypothermia had a significant impact on length of stay and respiratory support (Table 3). Infants who were hypothermic on admission had a significantly longer stay in hospital (mean (SD) 16.5 (18.1) v. 10.9 (12.6) days; p<0.00), and in the NICU (mean (SD) 3.7 (6.2) v. 2.3 (4.6) days; p<0.00). They also required respiratory support for longer (mean (SD) 2.9 (5.4) v. 1.7 (4.5) days; p<0.00), and more days of oxygen therapy (mean (SD) 7.2 (14.4) v. 3.4 (7.4) days; p<0.0001). VLBW infants with admission hypothermia had a near fourfold increased need for nCPAP compared with their normothermic counterparts (OR 3.9; p<0.00).
Discussion
The incidence of hypothermia on admission in the SBAH neonatal unit is high (67%; moderate-severe 41%). The incidence of neonatal hypothermia reported in lower- and middle-income country hospitals ranges from 32 to 85%.[15] Similar studies done with infants admitted in the first 28 days of life reported an incidence of 32 - 62%.[8,15-17] In this study, 82% of VLBW infants were hypothermic on admission. This is similar to previous findings in the unit.[14] However, it is higher than the incidence reported in other units. A recent Johannesburg study reported an incidence of 46% in VLBW infants admitted in the first 24 hours of life,[18] and an incidence of 53% has been reported in infants of <32 weeks' gestation in Europe.[12]
Preterm and VLBW infants have the highest risk of hypothermia.[7,12,19] Similarly, in this study, the risk of hypothermia was inversely proportional to birthweight and gestational age, and VLBW was an independent risk factor for hypothermia. Delivery by emergency caesarean section, low 1-minute Apgar scores, admission from theatre, and admission to the NICU were associated with increased risk of becoming hypothermic. These are known risk factors from previous studies.[4,7-9,17,19,20] In this study, resuscitation was defined as any intervention above routine neonatal care, including the administration of free-flow oxygen. A more stringent definition may have led to results showing a significant association between hypothermia and the need for resuscitation. The results may indicate a lack of adequate thermoregulatory care in the immediate postnatal period. Postnatal care practices, such as low delivery room temperature and lack of skilled care at delivery have been reported as causes for hypothermia.[3,4,21] Underlying conditions and inherent physiology, which predispose to delayed transition and the need for procedures in the delivery room, may also contribute to the increased risk.
Admission from the delivery room in the first 60 minutes of life was an independent risk factor for hypothermia. Infants who were admitted (and therefore had a temperature recorded) in the first 60 minutes of life were 2 - 4 times more likely to be hypothermic than those admitted later. Owing to bed shortage, infants occasionally await admission in a closed heated incubator in the delivery room. Sicker or more unstable infants are more likely to be rushed to the NICU soon after delivery and their underlying conditions and inherent physiology which predispose to delayed transition and the need for procedures in the delivery room, may predispose them to hypothermia. However, current practices for thermoregulatory care in the period immediately after delivery need to be evaluated.
This study was designed as an overall assessment of neonatal hypothermia in the neonatal unit; therefore infants admitted in the first 28 days of life were included. A wide selection likely resulted in heterogeneity in the aetiology of hypothermia in the study population. The majority of infants (87%, n=415/477) were admitted in the first 24 hours (day 1) of life. Thermoregulatory capability improves with increasing postnatal age[20] and hypothermia was more common in infants admitted on day 1, with 71% (n=293) of these infants being hypothermic on admission, compared with 42% (n=26/62) of infants admitted after day 1. Further, VLBW made up a larger proportion of the infants admitted on day 1 (28%, n=118), compared with infants admitted later (6%, n=4/62) Other characteristics, such as anthropometry and maternal characteristics were similar in the two groups. Risk factors for hypothermia were assessed for infants admitted in the first 6 hours of life where applicable (Tables 2 and 3). Contrary to other studies, outborn infants were less likely to be hypothermic. This can in part be explained by a likely higher postnatal age compared with inborn infants. Also, fewer outborn infants had VLBW (10%). However, it also suggests adequate thermal care during stabilisation at referring centres and in transit.
Hypothermia is associated with hypoglycaemia, acidosis, respiratory distress and respiratory distress syndrome (RDS), pneumonia, late-onset sepsis, delayed transition to neonatal circulation, coagulopathy and haemorrhage, acute renal failure, and intraventricular haemorrhage (IVH).[7-9,20] Although there was a trend to worsening outcomes with lower body temperature, the assessment of the impact on mortality and morbidities was limited by the inability to distinguish between moderate and severe hypothermia.
Admission hypothermia was associated with an increased need for respiratory support, increased duration of hospital stay and the need for NICU admission, placing an added burden on a resource-limited neonatal unit. Although not all confounders were specifically addressed in this assessment, this trend was seen in the VLBW cohort of infants as well. Hypothermic infants have higher postnatal weight loss and take longer to regain their birthweight as a result of increased energy demand, associated feeding difficulties and morbidities.[9,21]
There is no standardised thermal care protocol in the unit. Infants are generally nursed under overhead radiant warmers in the delivery room and some await admission in a heated closed incubator in the labour ward. On admission, infants are generally nursed under overhead radiant warmers (mainly in the NICU), in closed incubators or clothed in cribs (bigger babies). In this study, hypothermia persisted for a significant period after admission, with hypothermic infants taking an average of 4 hours to record a first normal temperature. The use of preventive measures against hypothermia during transfer was evaluated to determine the current standard of care. It is disconcerting that several VLBW infants were transported without additional heat provided (either a closed incubator or overhead heater), and the majority were not wrapped in plastic.
Thermal care forms an important part of routine neonatal care. Strategies to prevent hypothermia using a combination of interventions targeting the different modes of heat loss are essential. In this study, transfer in a closed incubator decreased the risk of hypothermia on admission. Several other measures are known to protect against hypothermia during routine care, transport, and during procedures such as resuscitation. These include: other heat sources such as radiant warmers, thermal mattresses and heated pads, maintaining a neutral ambient temperature, the use of warm humidified gases, using preheated blankets, the use of polyethylene plastic wraps or bags, early skin-to-skin care, and early initiation of breastfeeding.[9, 10, 19, 20, 22, 23]
Study limitations
Limitations of this study include incomplete/missing data owing to the retrospective design of the study. Almost 10% of infants admitted in the study period were not included in the analysis because of missing hospital records. The incidence and impact of severe hypothermia could not be fully assessed as infants could not be categorised into mild, moderate, and severe hypothermia categories because of inadequate assessment of temperature on admission in infants with a body temperature <35.0°C.
Conclusion
We recommend the adoption of an evidence-based thermal care protocol in the neonatal unit. Several guidelines are available which can be adapted to include means which are readily available in the unit[1, 5, 6, 10, 13, 20, 23] Healthcare workers need regular training on the causes, consequences, prevention, and management of hypothermia. The method of recording body temperature in the unit also needs to be standardised.
Declaration. None.
Acknowledgements. None.
Author contributions. RMT: conception and design of the research project, data collection, analysis and interpretation, drafting the article. MC: supervision of the project, study design and execution, article revision. PB: Statistical planning and analysis, article revision.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization, Maternal and Newborn Health/Safe Motherhood Unit. Thermal Protection of the Newborn : A Practical Guide. Geneva: Maternal and Newborn Health/Safe Motherhood Unit, Division of Reproductive Health (Technical Support), WHO, 1997. [ Links ]
2. Vermont Oxford Network. Despite decreases, nearly 4 in 10 infants are cold when admitted to the NICU. NICU by the Numbers, 19/9/2017. https://public.vtoxford.org/nicu-by-the-numbers/despite-decreases-nearly-4-in-10-infants-are-cold-when-admitted-to-the-nicu/ (accessed 20 September 2017). [ Links ]
3. Carlo WA. Perinatal and neonatal care in developing countries. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant, 11th ed. Philadelphia: Mosby/ Elsevier, 2020:120-139. [ Links ]
4. Mullany LC, ed. Neonatal hypothermia in low-resource settings. Semin Perinatol 2010;34(6):426-433. https://doi.org/10.1053/j.semperi.2010.09.007 [ Links ]
5. Madar J, Roehr CC, Ainsworth S, et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021;161:291-326. https://doi.org/10.1016/j.resuscitation.2021.02.014 [ Links ]
6. Wyckoff MH, Aziz K, Escobedo MB, et al. Part 13: Neonatal resuscitation: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015;132(18 suppl 2):S543-S60. https://doi.org/10.1161/CIR.00000000000002677. [ Links ]
7 . Laptook AR, Salhab W, Bhaskar B. Admission temperature of low birth weight infants: Predictors and associated morbidities. Pediatrics 2007;119(3):e643-e649. https://doi.org/10.1542/peds.2006-0943 [ Links ]
8. Da Mota Silveira SM, de Mello MJG, de Arruda Vidal S, de Frias PG, Cattaneo A. Hypothermia on admission: A risk factor for death in newborns referred to the Pernambuco Institute of Mother and Child Health. J Trop Pediatrics 2003;49(2):115-120. https://doi.org/10.1093/tropej/49.2.115 [ Links ]
9. McCall EM, Alderdice F, Halliday HL, Vohra S, Johnston L. Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants. Cochrane Database Syst Rev 2018;2(2):CD004210. https://doi.org/10.1002/14651858.CD004210.pub5. [ Links ]
10. Bissinger RL, Annibale DJ. Thermoregulation in very low-birth-weight infants during the golden hour: Results and implications. Adv Neonatal Care 2010;10(5):230-238. https://doi.org/10.1097/ANC.0b013e3181f0ae63 [ Links ]
11. Mullany LC, Katz J, Khatry SK, LeClerq SC, Darmstadt GL, Tielsch JM. Risk of mortality associated with neonatal hypothermia in southern Nepal. Arch Pediatr Adolesc Med 2010;164(7):650-656. https://doi.org/10.1001/archpediatrics.2010.103 [ Links ]
12. Wilson E, Maier RF, Norman M, et al. Admission hypothermia in very preterm infants and neonatal mortality and morbidity. J Pediatr 2016;175:61-67.e4. https://doi.org/10.1016/j.jpeds.2016.04.01613. [ Links ]
13. Lunze K, Hamer D. Thermal protection of the newborn in resource-limited environments. J Perinatol 2012;32(5):317-324. https://doi.org/10.1038/jp.2012.11 [ Links ]
14. Tshehla RM, Coetzee M, Becker PJ. Mortality and morbidity of very low-birthweight and extremely low-birthweight infants in a tertiary hospital in Tshwane. S Afr J Child Health 2019;13(2):89-97. https://doi.org/10.7196/SAJCH.2019.v13i2.1582 [ Links ]
15. Lunze K, Bloom DE, Jamison DT, Hamer DH. The global burden of neonatal hypothermia: Systematic review of a major challenge for newborn survival. BMC Med 2013;11(1):1-11. https://doi.org/10.1186/1741-7015-11-24 [ Links ]
16. Ogunlesi TA, Ogunfowora OB, Adekanmbi FA, Fetuga BM, Olanrewaju DM. Point-of-admission hypothermia among high-risk Nigerian newborns. BMC Pediatr 2008;8(1):1-5. https://doi.org/10.1186/1471-2431-8-40 [ Links ]
17. Ukke GG, Diriba K. Prevalence and factors associated with neonatal hypothermia on admission to neonatal intensive care units in Southwest Ethiopia: A cross-sectional study. PloS ONE 2019;14(6):e0218020. https://doi.org/10.1371/journal.pone.0218020 [ Links ]
18. Ng'eny JC, Velaphi S. Hypothermia among neonates admitted to the neonatal unit at a tertiary hospital in South Africa. J Perinatol 2020;40(3):433-438. https://doi.org/10.1038/s41372-019-0539-y [ Links ]
19. Asakura H. Fetal and neonatal thermoregulation. J Nippon Med School 2004;71(6):360-70. https://doi.org/10.1272/jnms.71.360 [ Links ]
20. Ágren J. Thermal environment of the intensive care nursery. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 11th ed. Philadelphia: Mosby/Elsevier, 2020: 566-576. [ Links ]
21. Onalo R. Neonatal hypothermia in sub-Saharan Africa: A review. Nigerian J Clin Prac 2013;16(2):129-138. https://doi.org/10.4103/1119-3077.110120 [ Links ]
22. Oatley H, Blencowe H, Lawn J. The effect of coverings, including plastic bags and wraps, on mortality and morbidity in preterm and full-term neonates. J Perinatol 2016;36(1):S83-S89. https://doi.org/10.1038/jp.2016.35 [ Links ]
23. Pinheiro JM, Furdon SA, Boynton S, Dugan R, Reu-Donlon C, Jensen S. Decreasing hypothermia during delivery room stabilisation of preterm neonates. Pediatrics 2014;133(1):218-226. https://doi.org/10.1542/peds.2013-1293 [ Links ]
 Correspondence:
Correspondence:
R Tshehla
rosine.tshehla@up.ac.za
Accepted 3 August 2023


{kind=link}
{kind=link}
{kind=link}