










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.17 no.4 Pretoria Dez. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i4.2007
ARTICLE
The prevalence and spectrum of thyroid dysfunction among children with Down syndrome attending the paediatric services at two tertiary hospitals in Pretoria, South Africa
S F MaphumuloI; E M HoneyII; N AbdelatifIII; M KarsasIV
IMB ChB, FCPaed (SA); Department of Paediatrics and Child Health, University of Pretoria, South Africa
IIMB ChB, MMed (Paed); Department of Biochemistry, Genetics and Microbiology, Faculty of Natural and Agricultural Sciences, University of Pretoria, South Africa
IIIMS Statistics; Biostatistics Research Unit, South African Medical Research Council, Cape Town, South Africa
IVMMed, Cert Paed Endocrinology and Metabolism (SA) Department of Paediatrics and Child Health, University of Pretoria, South Africa
ABSTRACT
BACKGROUND:Down syndrome (DS) is the most common chromosomal abnormality in the paediatric setting, and thyroid dysfunction is more commonly encountered in this population than among the general population. The literature shows that the most common type of thyroid dysfunction seen in these children is subclinical hypothyroidism.
OBJECTIVE:The purpose of this study was to establish the prevalence and spectrum of thyroid disease in this population, with the aim of establishing easy-to-follow protocols.
METHOD:A retrospective study was conducted in children with DS who were seen at the paediatric genetic clinic at two academic hospitals. Data were collected from the hospital files and the results were extracted from the National Health Laboratory Service database system.
RESULTS:A total of 158 children were recruited; 25 children were excluded as they had had no thyroid function tests done. From the total of 133 included children, 70 (52.6%) were male. Babies born in one of the two hospitals numbered 60 (45.1%), whereas 54.9% were born in the other hospital. A total of 77 (57.9%) were found to have thyroid dysfunction; 55.8% of these patients were male. The most common thyroid abnormality was subclinical hypothyroidism in n=66/133 (49.6%), accounting for 85.7% of the causes of the thyroid dysfunction. Most children (n=45/133 (33.8%)) had their first thyroid function test done before the age of 2 months, followed by the age group of 1 - 5 years (n=34/133 (25.56%)). The total number of children started on treatment for their thyroid dysfunction was n=5/77 (6.49%).
CONCLUSION:Thyroid dysfunction is seen more commonly in children with DS compared with the general population, which was very evident in the present study. A standardised protocol will have a significant impact on the early management of these children, to prevent further cognitive impairment, especially in developing countries and at any level of healthcare. The recommendations for thyroid dysfunction screening by the American Academy of Pediatrics can be adjusted and tailored for the South African population. Early diagnosis and referral of children with DS to a secondary- or tertiary-level facility is of utmost benefit for these children for screening and treatment of comorbidities and complications.
Down syndrome (DS) is the most common chromosomal abnormality in South Africa and the world at large. It occurs in approximately 1 in 800 live births worldwide.[1] In the majority of cases, DS is due to non-disjunction of chromosome 21 during meiosis, and the remainder of the cases are due to translocation or mosaicism. The diagnosis of DS is made on the clinical findings and on genetic testing karyotype for trisomy.[2] In most developing countries, karyotyping is not feasible for most cases and therefore a clinical diagnosis based on phenotypical features is made, with 88% accuracy.[3] DS is associated with an increased risk of medical problems. The most commonly encountered problems in this population include gastro-intestinal, cardiac, haematological, developmental and endocrine abnormalities.[4]
A common endocrine condition found in DS children is thyroid dysfunction and, if left untreated, can contribute immensely to the developmental and intellectual impairment of these children. The prevalence of thyroid dysfunction in children with DS is estimated to range between 4% and 19.5%.[5-7] The spectrum of dysfunction in children with DS ranges from overt disease that requires treatment to transient forms that require only observation and close monitoring.[4] The spectrum of thyroid dysfunction includes congenital hypothyroidism, subclinical hypothyroidism, acquired hypothyroidism (auto-immune and non-auto-immune) and hyperthyroidism.[4] The most common form of thyroid dysfunction in children with DS found in most studies worldwide is subclinical hypothyroidism.[8]
Thyroid hormones are essential for metabolism and development of a child.[8] Thyroid hormones specifically are essential for central nervous system development; they affect neuronal migration and differentiation, myelination, synthesis and secretion of neurotransmitters and activation of the sympathetic nervous system.[9] Therefore, the screening for thyroid dysfunction is essential, especially in a population that is known to be at higher risk, such as DS. Thyroid dysfunction, if left untreated, will result in worsening of psychomotor development, mental retardation and growth retardation.[9] These consequences are devastating to the developing brain of these children, and therefore early diagnosis and treatment initiation is imperative. In First-World countries, routine screening for thyroid dysfunction is mandatory. The American Academy of Pediatrics (AAP) recommends thyroid function screening in children with DS at birth, 6 months, 12 months and thereafter yearly.[10] In developing countries such as South Africa, this is not routinely done, and there have been few studies done in Africa at large.[11] There are no local South African nor African guidelines for thyroid screening of these children.
The purpose of the present study is to establish the spectrum of thyroid dysfunction in this population and the age of diagnosis of thyroid dysfunction. These data will in turn assist in establishing the crucial points or age range for screening in our setting.
Methods
A retrospective study was conducted in two academic hospitals based in Pretoria, Gauteng, South Africa, namely Kalafong Provincial Academic Hospital and Steve Biko Academic Hospital. These hospitals both have a genetic clinic run by the same consultant, once a week in each hospital. The data collected included all children with DS who followed up at these clinics from January 2015 to December 2019. Their thyroid function tests were obtained from clinical files and electronically from the National Health Laboratory Services (NHLS) Web Results Viewer (https:// trakcarelabwebview.nhls.ac.za).
Ethics approval was obtained from the University of Pretoria Research Ethics Committee (Ethics reference number: 88/2021) as well as the National Health Research Database (NHRD). A data collection tool was used in which information including the age, sex, age at diagnosis of DS, method of diagnosis of DS and age of first thyroid function with subsequent thyroid function tests was recorded. The presence of comorbidities, final diagnosis and whether or not the child was initiated on treatment was also recorded. Thyroid function test analysis was done using the Beckman Coulter Chemistry analyzer DxC600i. The reference ranges used by the NHLS for thyroid interpretation were obtained from the chemistry laboratories at Steve Biko Academic hospital and Kalafong Provincial Academic Hospital who use the cutoffs supplied by Abbott.
Definitions of terms
Down syndrome diagnosis
• Phenotypic DS: DS was diagnosed phenotypically by the presence of specific clinical features, namely a flat facial profile, up-slanting eyes, epicanthic folds, macroglossia, small and abnormally shaped ears, single palmar crease, sandal gap, hypotonia and often associated with a congenital heart defect.[12]
• Genetically confirmed DS: In some cases, DS was also diagnosed genetically, defined as the chromosomal defect on chromosome 21, as commonly referred to as trisomy 21 on QF-PCR or karyotype.[13]
Definitions of thyroid abnormalities[11]
• Congenital hypothyroidism: high TSH in the neonatal period with a low T4
• Subclinical hypothyroidism: high TSH with a normal T4 at diagnosis
• Overt hypothyroidism: high TSH with a low T4 at diagnosis
• Central hypothyroidism: low or normal TSH with a low T4 at diagnosis
• Hyperthyroidism: low TSH with a high T4 at diagnosis.
Normal reference ranges for thyroid function test in the National Health Laboratory services are provided according to age.
TSH levels were regarded as abnormal if outside the reference interval used at the NHLS (0.27 - 4.2 mlU/L) in adults or older children.[14]
Statistical analysis
The data were entered and analysed using Microsoft Excel and Stata 16 (StataCorp. 2019. Stata Statistical Software: Release 16. College Station). Data were summarised as frequencies along with percentages. Associations with final diagnosis were assessed using chi-square tests, i-tests for normally distributed variables and quantile regression for variables that were skewed. A p-value <0.05 was considered to be statistically significant.
Results
A total of 158 children were recruited for this study; 25 children were excluded as they had no thyroid function test (TFT) done. From the 133 included children, 70 (52.6%) were male and 60 (45.1%) were inborn. The diagnosis of DS was confirmed genetically in 55 (41.35%), while the remaining 78 (58.64%) were phenotypic DS. The median age at diagnosis of DS was one day with a range of one day to 72 months of age. All children included had at least one TFT done. In his study, 33 children had only one TFT done (22.55%), 30 (22.55%) had a TFT done twice, and the remaining 73 (54.9%) had three or more TFTs done. Most children had their first TFT done before the age of two months (as a neonate); 45 (33.8%), followed by the age group of 1 - 5 years; 34 (25.5%).
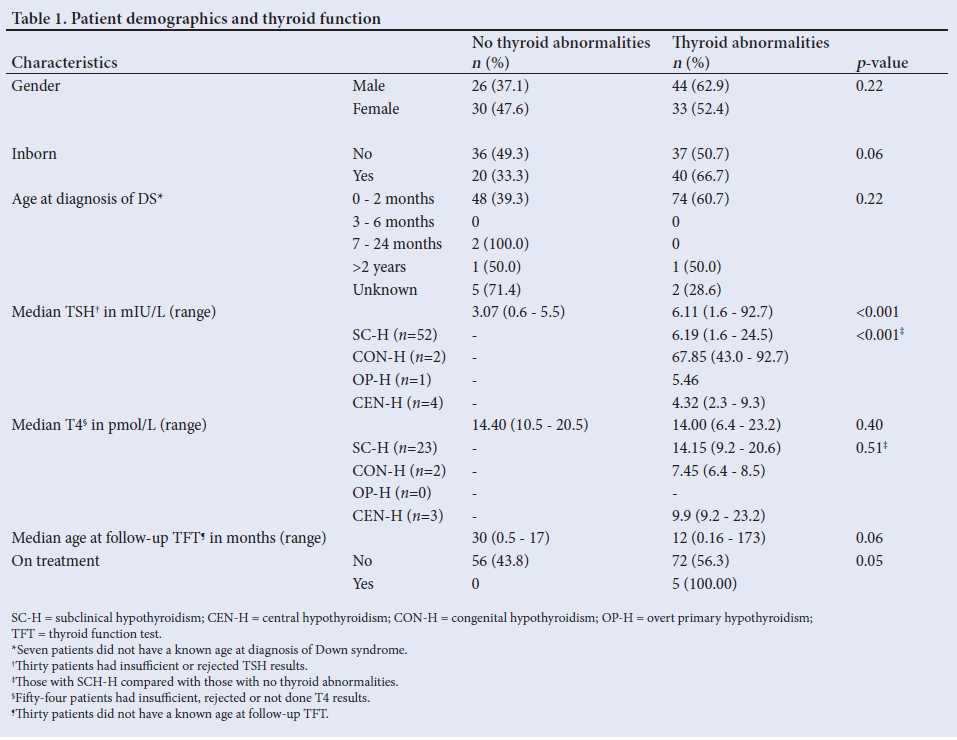
A total of 77 (57.9%) of the patients' TFT results were abnormal; 44 (57.1%) were male and 33 (42.9%) female. Analysis of the various thyroid abnormalities revealed 85.7% (n=66/77) to have subclinical hypothyroidism which was transient in 40.3% (n=31/77) ofpatients. In the transient group, thyroid functions normalised within an average of 6 - 12 months. Congenital hypothyroidism was found in 5.2% (n=4/77), overt primary hypothyroidism in 2.6% (n=2/77) and central hypothyroidism in 6.5% (n=5/77), the latter being transient in 3.9% (n=3/77) while the remaining 2.6% (n=2/77) did not receive a repeat TFT nor work-up. No patient with DS in this cohort was found to have hyperthyroidism. The mean age at diagnosis was 1 month (range 8 days - 2 months) in the congenital hypothyroidism group, 23 months (range 0.1 - 173 months) in the subclinical hypothyroidism group; 60 months (range 41 -79 months) in the overt primary hypothyroidism group, and 91.6 months (range 13 - 153 months) in the central hypothyroidism group. The median TSH at diagnosis was 67.85 IU/mL (range 42.95 - 92.74) in the congenital hypothyroidism group, 6.19 IU/mL (range 1.6 - 24.48 IU/mL) in the subclinical hypothyroidism group, 5 IU/mL in the overt primary hypothyroidism group, and 4.32 IU/mL (range 2.33 - 9.31) in the central hypothyroidism group. The median T4 at diagnosis was 7.45 pmol/L (range 6.4 - 8.5) in the congenital hypothyroidism group, 14.15 pmol/L (range 9.2 - 20.6) in the subclinical hypothyroidism group, none in the overt primary hypothyroidism group, and 9.9 pmol/L (range 9.2 - 23.2) in the central hypothyroidism group (Table 1).
The total number of children on treatment who had abnormal TFTs was n=5/77 (6.49%); 1 child had overt primary hypothyroidism and 4 children had congenital hypothyroidism. One child had mild overt primary hypothyroidism which recovered on subsequent testing without treatment and, in the 5 children with central hypothyroidism, 3 had transient dysfunction which resolved and 2 were lost to follow-up and therefore untreated. None of the children with subclinical hypothyroidism was treated in this study as there is currently no consensus with regard to the clinical significance, investigation nor treatment of subclinical hypothyroidism in national or international guidelines.[11]
The comorbidities established in this study population included cardiac defects predominantly (in 9.0%), followed by attention deficit hyperactivity disorder (2.25%), autism spectrum disorder (1.5%), epilepsy (1.5%), cystic fibrosis (1.5%), significant intellectual impairment (0.75%), stroke/cerebrovascular accident (0.75%) and hyperparathyroidism (0.75%).
Discussion
DS is one of the most common chromosomal abnormalities. Multisystemic involvement including thyroid dysfunction can cause significant morbidity if left untreated.[15] The thyroid hormone plays a vital role in metabolism, growth and development of children, especially in infancy.[16] The clinical presentation of hypothyroidism in an older child can be missed, as the signs and symptoms can overlap with that of DS.[17]
In the present study, a total of 77 (57.9%) DS patients had thyroid dysfunction. This was much higher than in the study previously done in Johannesburg, South Africa, that showed thyroid dysfunction in 34.5% and was also higher than a recent study in Ethiopia revealing thyroid dysfunction in 47.7%.[11] Our local prevalence was also higher than reported in other international studies in developed countries such as California, USA, which reported a prevalence of 32.5%.[9,11,18] It is important to note, however, that the inclusion of transient cases may have contributed to the higher total number of cases of thyroid dysfunction in this study as compared with the other studies. The current recommendation by the AAP suggests that children be tested at birth, 6 months, 12 months and then annually.[19] The study done in Ethiopia proposed that screening should include at least a test at 2 months, as they had a large number of children diagnosed between birth and 2 months.[20] Similarly, in this study, a significant number of children had thyroid abnormalities evident on testing done between birth and 6 months, with the highest number (33.8%) being between 0 and 2 months' age.
In the general population, thyroid dysfunction is seen more commonly in females than in males.[21] In contrast, in children with DS, more males than females have thyroid abnormalities.[18] In the present study, similar findings were observed even though the findings were not statistically significant (p-value 0.376). The most common cause of thyroid abnormalities in this small cohort was subclinical hypothyroidism (85.7%); however, in 40.3% it was transient, with subsequent normalisation of their thyroid functions. Similar findings have been observed in a number of studies done previously in other institutions. This phenomenon can be explained by the transient or temporary deficiency of the thyroid hormone which later recovers owing to improved thyroxine production.[22]
There are conflicting views on whether to treat DS children who have subclinical hypothyroidism. There are also different views over the cut-off point to be used to decide on treatment. Some authors have recommended not treating subclinical hypothyroidism in children with DS because it is benign and self-remitting in nature, while other authors argue that early treatment is potentially harmless and can improve growth and development including intellectual function in children with DS.[23] The recommendation suggests that treatment should be considered and confined to children with DS who have progressed from subclinical to overt hypothyroidism and those with a TSH >10 μU/mL. Treatment is also suggested in DS children who are symptomatic, including those with goitre and where antithyroid antibodies have been detected.[24] Thyroid hormone replacement therapy is not indicated in children with idiopathic subclinical hypothyroidism, mild subclinical hypothyroidism, negative antithyroid antibodies and no goitre with no ultrasound evidence of hypothyroidism. It is, however, evident that a small percentage of children with hypothyroidism may not have antithyroid antibodies. In a case where no therapeutic intervention is done, the clinical status and TFTs should be monitored periodically and each case be managed individually.[25]
It has been established that DS can affect practically any organ system in the human body. The appropriate management of comorbidities plays a significant role in the quality of life of these children.[26 Children enrolled in the present study had comorbidities of which the most common finding was congenital cardiac disease.[27] A child with DS should be seen at least once by a paediatrician for further evaluation in order to properly screen for all possible conditions associated with this syndrome.[28] In African countries, especially in the public sector, not every child will receive the opportunity to be seen by a specialist paediatrician as is recommended, which calls for an intervention in the form of increased awareness and established protocols that can be used at any healthcare level.
The main aim of the present study was to establish the spectrum of disease in the DS population with the aim of establishing an easy-to-follow protocol. In the South African population, owing to the general socio-economic status of patients, many children are lost to follow-up. Awareness of DS should be emphasised at primary healthcare level so that the transfer or referral to a secondary or tertiary level can be made timeously. The recommendation to add a thyroid screening protocol to local neonatal and paediatric clinical guidelines at secondary- and tertiary-level hospitals should be considered.
The study had several limitations. The population size was small, and it was a retrospective study based on hospital files which did not always have complete information. Some patients were also lost to follow-up and subsequently did not have repeat TFTs. The study also did not include a control group. Regarding strengths, this study was conducted in two different hospitals; however, further larger studies would be beneficial to fully assess the impact of thyroid dysfunction and the necessity for treatment of subclinical hypothyroidism in the population of children with DS.
Conclusion
Thyroid dysfunction is seen more commonly in children with DS than among the general population, which was very evident in the present study. A standardised local protocol will have a significant impact on the management of these children, especially in developing countries and at any level of healthcare. The recommendation by the AAP, which recommends thyroid function screening in children with DS at birth, 6 months, 12 months and thereafter annually, should be followed in the South African population. Possibly it may be tailored to our population with the addition of a further test at 2 months (if no thyroid function was done at birth) owing to the higher rates of thyroid dysfunction diagnosed in the neonatal period.
Owing to the multiple complications and comorbidities that occur in children with DS, it is recommended that children with DS should be recognised early (preferably in the neonatal period), diagnosed and referred to a secondary- or tertiary-level centre to be seen by a specialist paediatrician for adequate screening and monitoring.
Declaration. This article is submitted in partial fulfilment of the degree of Master of Medicine in the field of Paediatrics at the University of Pretoria by SFM.
Acknowledgements. None.
Author contributions. SFM: original draft writing, data collection, self funding. MK: original draft corrections, data interpretation and analysis. EMH: original draft analysis, data collection, interpretation and analysis. NA: statistical analysis and interpretation of results.
Funding. None.
Conflicts of interest. None.
References
1. Bull MJ. Down syndrome. N Eng J Med 2020;382(24):2344-2352. [ Links ]
2. Chandra N, Cyril C, Lakshminarayana P, et al. Cytogenetic evaluation of Down syndrome: A review of 1020 referral cases. Int J Human Genet 2010;10(1-3):87-93. [ Links ]
3. Devlin L, Morrison P. Accuracy of the clinical diagnosis of Down syndrome. Ulster Med J 2004;73(1):4-12. [ Links ]
4. Bull MJ, Trotter T, Santoro SL, Christensen C, Grout RW. Health supervision for children and adolescents with Down syndrome. Pediatrics 2022;149(5):1-24. [ Links ]
5. Iughetti L, Lucaccioni L, Fugetto F, Mason A, Predieri B. Thyroid function in Down syndrome. Expert Rev Endocrinol Metab 2015;10(5):525-532. [ Links ]
6. Murphy J, Philip M, Macken S, et al. Thyroid dysfunction in Down's syndrome and screening for hypothyroidism in children and adolescents using capillary TSH measurement. J Pediatric Endocrinol Metabol 2008;21(2):155-164. [ Links ]
7. Gibson P, Newton R, Selby K, Price D, Leyland K, Addison G. Longitudinal study of thyroid function in Down's syndrome in the first two decades. Arch Dis Childhood 2005;90(6):574-578. [ Links ]
8. Oliveira A, Longui CA, Calliari E, Ferone EdA, Kawaguti FS, Monte O. Evaluation of the hypothalamic-pituitary-thyroid axis in children with Down syndrome. J Pediatr (Rio J) 2002;78(4):295-300. [ Links ]
9. Purdy I, Singh N, Brown W, Vangala S, Devaskar U. Revisiting early hypothyroidism screening in infants with Down syndrome. J Perinatol 2014;34(12):936-940. [ Links ]
10. Bull MJ. Health supervision for children with Down syndrome. Pediatrics 2011;128(2):393-406. [ Links ]
11. Moosa S, Segal DG, Christianson AL, Gregersen NE. Thyroid dysfunction in a cohort of South African children with Down syndrome. S Afr Med J 2013;103(12):966-970. [ Links ]
12. Chapman RS, Hesketh LJ. Behavioral phenotype of individuals with Down syndrome. Ment Retard Dev Disabil Res Rev 2000;6(2):84-95. [ Links ]
13. Petersen M, Mikkelsen M. Nondisjunction in trisomy 21: Origin and mechanisms. Cytogen Genome Res 2000;91(1-4):199-203. [ Links ]
14. Kruger E, Coetzee A, Conradie M, Hoffmann M. An audit of thyroid function testing in acutely ill patients at a South African academic hospital. Southern Afr J Crit Care 2020;36(1):46-50. [ Links ]
15. Vadakedom SS, Krishnan DK, Mammen DS, Antony JM. Medical problems in children with Down syndrome. Int J Adv Med 2018;5(5):1290-1294. [ Links ]
16. MacGillivray MH, Aceto T, Frohman LA. Plasma growth hormone responses and growth retardation of hypothyroidism. Am J Dis Children 1968;115(2):273-276. [ Links ]
17. Karlsson B, Gustafsson J, Hedov G, Ivarsson S, Annerén G. Thyroid dysfunction in Down's syndrome: Relation to age and thyroid autoimmunity. Arch Dis Childhood 1998;79(3):242-245. [ Links ]
18. Pierce MJ, LaFranchi SH, Pinter JD. Characterisation of thyroid abnormalities in a large cohort of children with Down syndrome. Horm Res Paediatr 2017;87(3):170-178. [ Links ]
19. Fergeson MA, Mulvihill JJ, Schaefer GB, et al. Low adherence to national guidelines for thyroid screening in Down syndrome. Genetics Med 2009;11(7):548-551. [ Links ]
20. Mulu B, Fantahun B. Thyroid abnormalities in children with Down syndrome at St. Paul's Hospital Millennium Medical College, Ethiopia. Endocrinol Diabetes Metabol 2022;00:e337. [ Links ]
21. Del Ghianda S, Tonacchera M, Vitti P. Thyroid and menopause. Climacteric 2014;17(3):225-234. [ Links ]
22. Kanike N, Davis A, Shekhawat PS. Transient hypothyroidism in the newborn: To treat or not to treat. Translational Pediatrics 2017;6(4):349. [ Links ]
23. Metwalley KA, Farghaly HS. Endocrinal dysfunction in children with Down syndrome. Ann Pediatric Endocrinol Metabol 2022;27(1):15. [ Links ]
24. Amr NH. Thyroid disorders in subjects with Down syndrome: An update. Acta Bio Medica: Atenei Parmensis 2018;89(1):132. [ Links ]
25. Crisafulli G, Aversa T, Zirilli G, et al. Subclinical hypothyroidism in children: When a replacement hormonal treatment might be advisable. Front Endocrin 2019;10:109. [ Links ]
26. Bittles AH, Bower C, Hussain R, Glasson EJ. The four ages of Down syndrome. Eur J Public Health 2007;17(2):221-225. [ Links ]
27. Marder L, Tulloh R, Pascall E. Cardiac problems in Down syndrome. Paediatrics and Child Health 2015;25(1):23-29. [ Links ]
28. Charleton PM, Dennis J, Marder E. Medical management of children with Down syndrome. Paediatrics and Child Health 2010;20(7):331-337. [ Links ]
 Correspondence:
Correspondence:
msizakele@icloud.com
Accepted 31 October 2022


{kind=link}