










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.17 no.4 Pretoria Dez. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i4.1957
ARTICLE
Low birthweight and maternal smoking as predictors of infant lung function from a South African birth cohort within low socioeconomic communities
S MuttooI; P M JeenaII; M RöösliIII; A C OlinIV; H K CarlsenV; K AsharamVI; G NaidooVII; A A MitkuI, VIII; R N NaidooIX
IPhD; Discipline of Occupational and Environmental Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIMD, PhD; Discipline of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIPhD; Swiss Tropical and Public Health Institute, Basel, Switzerland
IVMD, PhD; Department of Occupational and Environmental Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden
VPhD; Department of Occupational and Environmental Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden
VIMSc; Discipline of Occupational and Environmental Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
VIIBTech; Discipline of Occupational and Environmental Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
VIIIPhD; Department of Statistics, College of Science, Bahir Dar University, Bahir Dar, Ethiopia
IXMD, PhD; Discipline of Occupational and Environmental Health, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Early assessment of infant lung function (ILF) is necessary to improve our understanding of factors that determine long-term respiratory health.
OBJECTIVE: To identify predictors of lung function among infants aged 6 weeks, 6, 12 and 24 months, from low socioeconomic settings, enrolled within the Mother and Child in the Environment (MACE) study.
METHODS: ILF tests were performed assessing multiple breath washout and tidal breathing during spontaneous sleep. Several risk factors, relating to infant growth, maternal and environmental exposures, were assessed cross-sectionally against the lung function parameters in multivariable models for each age group.
RESULTS: Maternal smoking during pregnancy affected the ratio of time to peak expiratory flow, showing a decline across the age groups, while being statistically significant (β (95% confidence interval (CI)) at 6 weeks (-24.6% (-43.92 -4.59)) and 12 months (-12.68 (-25.25 - -0.11)). Low birthweight was associated with a lower tidal volume at 6 weeks (-5.99 mL (-9.59 - -2.39)), 6 months (-15.02 mL (-22.48 -7.57)) and 12 months (-23.7 mL (-35.55 -11.85)), compared with those with normal birthweight. This was further observed for minute ventilation at 6 weeks (-157.78 mL/min (-338.95 - 23.38)), 6 months (-325.57 mL/min (-619.06 --32.08)) and 12 months (-527.58 mL/min (-947.85 - -107.32)), though less evident at 24 months.
CONCLUSION: Low birthweight was the main predictor for low tidal volumes and minute ventilation at 6 weeks, with smaller differences observed at 12 and 24 months. Lung function development early in life is primarily driven by infant size and postnatal growth factors, consistent with other studies.
The physiological development of infant lungs undergoes dynamic changes in the first few months of life and in early childhood. Parameters such as tidal volume (TV), respiratory rate (RR) and minute ventilation (MV), which define the functional characteristics of the lungs, change at different scales in relation to lung size. Measurements of functional residual capacity (FRC) performed in infants have been shown to be significantly associated with lung volume and infant anthropometry (weight and length). After birth, lung size increases proportionally with body size, and is affected by age and sex.'[1]
The association between early lung development and airway function is complex and is influenced by exposure to prenatal and post-natal risk factors. Inconsistencies among studies exploring the impacts of growth factors on lung function and risk of respiratory morbidity or mortality suggest that normal physiological growth and development patterns of the airways of infants are not fully understood.[2] Epidemiological studies measuring premorbid lung function in infancy indicate the importance of exposure to risk factors during fetal and early postnatal life.[3] In low- to middle-income settings, with a high burden of infant lower respiratory tract infections,[4] several environmental factors, including air pollutant exposure and environmental tobacco smoke exposure, as well as maternal factors, such as maternal smoking during pregnancy and maternal HIV status, and socioeconomic factors, require investigation for their effect on infant lung function.
Multiple breath washout (MBW) testing is useful in the early detection of structural alterations and a more sensitive measure of small airway functioning than conventional lung function tests,[5] with application successful among infants and children. Some studies have further demonstrated that school-aged children with asthma had increased ventilatory inhomogeneity even when spirometry results were reflected as normal.[6] The lung clearance index (LCI), as determined by MBW testing, has been identified as an important index reflecting ventilation inhomogeneity and small airway dysfunction and a valuable tool to detect disease progress in cystic fibrosis (CF).[7,8
Previous studies have shown that the LCI is reproducible and a more sensitive measure than forced expiratory ventilation (FEV1) in identifying early lung disease in children.[9] It has also been shown to be influenced by large changes in TV, RR or FRC.[7] Measures of FRC and LCI reflect lung size and ventilation homogeneity, respectively, as markers of growth and maturation. Tidal breathing measures are important markers of the control of breathing and airway mechanics which are determined by TV, breathing frequency and MV.[10] Studies have demonstrated that FRC and tidal flows (volume-dependent parameters), are important proxies of early lung health.[4,10-12}
This study aims to identify predictors of lung function among infants aged 6 weeks, 6, 12 and 24 months, from low socioeconomic settings, enrolled within the Mother and Child in the Environment (MACE) study.
Methods
Selection of study participants
Details on participant selection in the MACE cohort is described elsewhere.[13] Infant assessment within this cohort required testing at the ages of 6 weeks, 6, 12 and 24 months. Participants were subjected to standardised interviews, clinical evaluation and lung function testing. This study has been approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee (ref. no. BE431/17). Maternal or primary caregiver written consent was obtained prior to lung function testing. Data collection in the cohort entailed detailed questionnaire interviews at recruitment, at each trimester of pregnancy, early postnatal period, and at regular intervals during infancy.
All infant participants were pre-booked and scheduled to attend clinical visits at the age of 6 weeks, 6, 12 and 24 months. Participants had been pre-screened by simple questionnaire to determine if they were ill in the prior week, were on medication, recently vaccinated or currently teething (these factors were considered to affect either sleep state or success of the test). No appointment was scheduled if there were any positive responses to these enquiries.
Data collection
Data on maternal smoking during pregnancy, HIV status and income status (classified as low if annual income <USD2 000 and high if above this), and child's sex, gestational age, birthweight and length were obtained from questionnaires. Time-variant data such as age, weight, length (reported as postnatal weight and length gain) and self-reported wheezing were recorded at each test date. Low birthweight (LBW) (<2.5 kg) and pre-term birth (PTB) (gestational age <37 weeks) are defined as per the WHO guidelines.[14] Postnatal child weight and length gain were calculated as the difference between the absolute measures taken at the test occasion and time of birth. Environmental exposure data were obtained from recruitment questionnaires and included housing type (formal v. informal), environmental tobacco smoke exposure and residential proximity to the nearest road and industry. In addition to questionnaire data, clinical assessments evaluating growth and developmental milestones and detailed respiratory evaluation were undertaken at the 12 and 24 months visit.
Lung function measurements
Lung function measures were conducted over the period January 2017 to September 2019. Participants were clinically assessed on the day of the test to exclude respiratory infections which, if present, resulted in a rescheduling of the test within at least 1 week. Lung function measurements were performed in unsedated infants, by trained individuals, competent in testing and analysis. Tests were performed during quiet natural sleep in the supine position, using the Exhalyzer D with ultrasonic flow meter (Ecomedics AG, Switzerland) as per the European Respiratory Society/American Thoracic Society (ERS/ATS) standards,[15,16] and analysis using the software Wbreath v2.0 (Ndd Medizintechnik AG, Switzerland). For quality control blind analysis of test outputs was conducted and observations were compared to achieve high accuracy.
Tidal breathing measurements were assessed for 30 homogenous breaths during non-rapid eye-movement sleep from a 2-minute recording. Test outputs with sighs, apnoea, interruption in breathing pattern, or leak detection, were excluded as part of the quality control.[15,16] The main outcome parameters measured included TV, RR, MV, mean tidal inspiratory flow (MTIF), mean tidal expiratory flow (MTEF) and time to peak tidal expiratory flow over total expiratory time (tPTEF/tE).
MBW measurements were performed using 4% sulphur hexafluoride (SF6) tracer gas and ultrasonic flowmeter (Spiroson, Ecomedics, Switzerland), of which three consecutive tests were performed. Acceptability was based on FRC means within 25% across three successful tests or 10% for two successful tests and LCI within one turnover of each other. Additional quality checks for MBW tests included five homogenous breaths before wash in, a 10-breath plateau before commencement of washout and 10 breaths after washout, as the SF6 returns to baseline.[17]
Statistical analysis
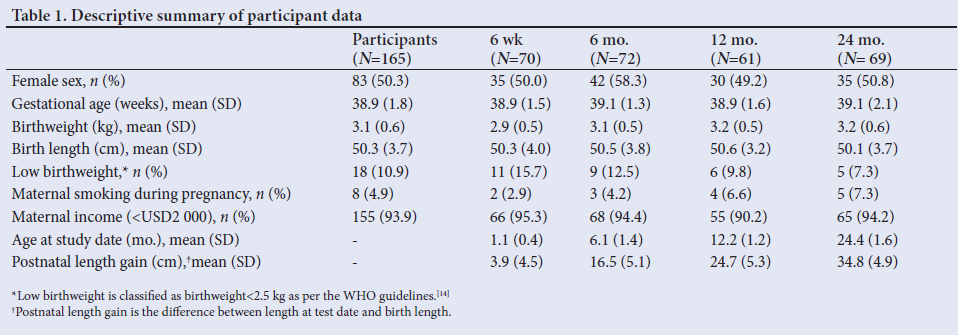
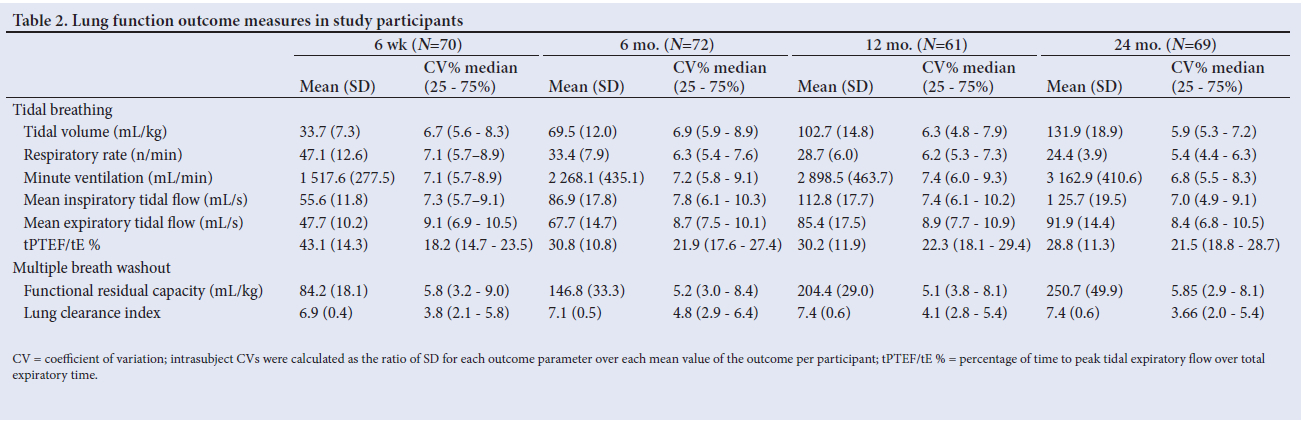
Descriptive statistics and regression analyses were performed using STATA 15 for Windows (STATACorp., USA) (Table 1). The intra-subject coefficient of variation was calculated to determine the consistency of multiple testing across the different age groups, for each participant and for each measurement parameter, and is presented for all outcomes (Table 2).
Because of the novelty of the research, there are few reports for the parameters of interest, with similar population characteristics and risk factors for precise sample size determination. As a result, we used the Bern Infant Lung Development Study (BILD)[12] and Drakenstein Child Lung Health Study (DCHLS)[4] to represent exposed and unexposed groups, respectively. The sample size calculations indicated that 89 per exposure group were necessary at the baseline of 6 weeks old. As we intended to address several additional covariates, we targeted a sample of 100 in each exposure group.
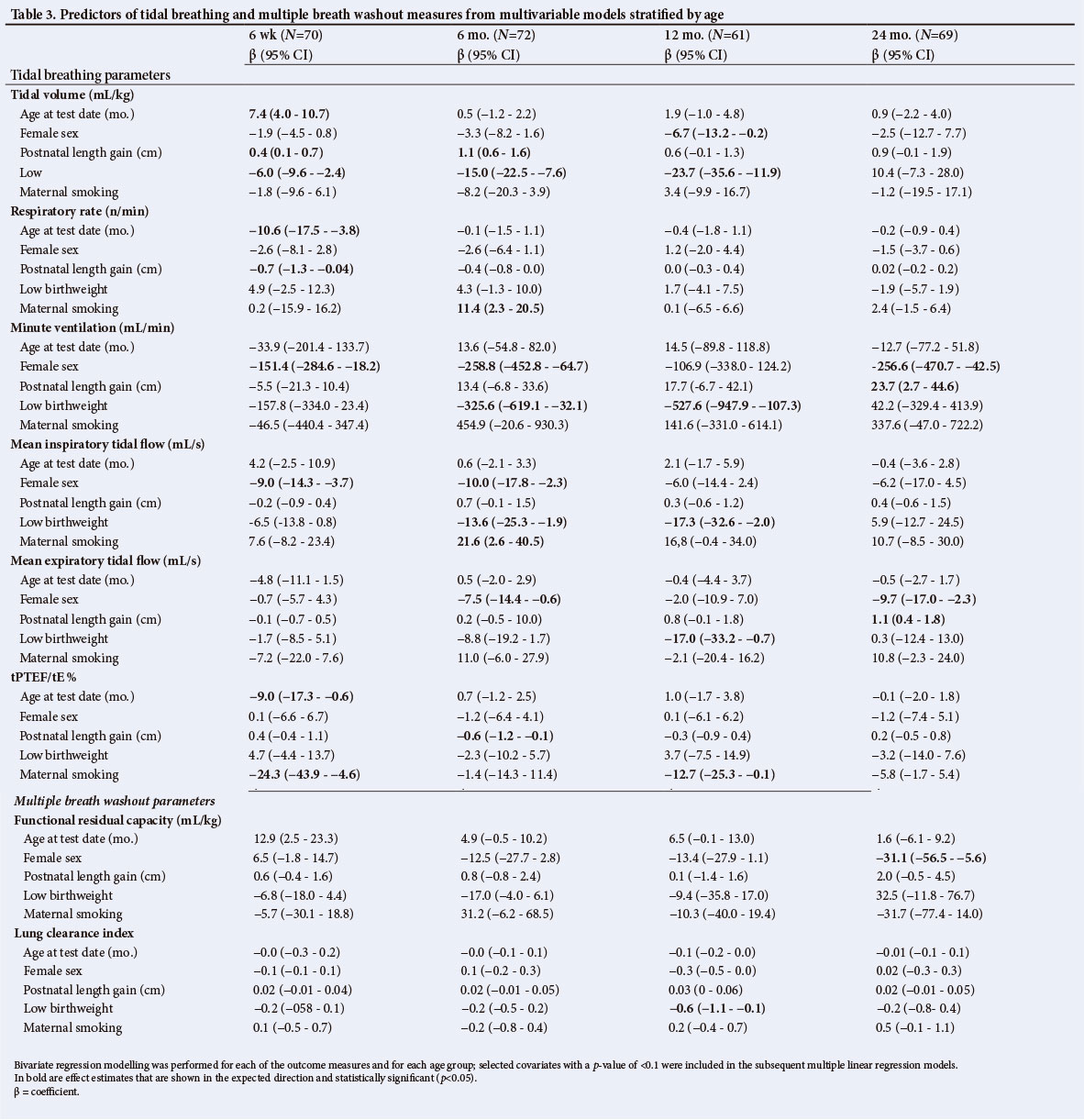
Although some participants contributed to more than one time point, no longitudinal analyses were performed. Cross-sectional multivariable linear regression models are presented by individual age groups (6 weeks, 6, 12 and 24 months) and by individual outcomes (TV, RR, MV, MTIF, MTEF, tPTEF/tE %, FRC and LCI) per age group. The normality of data was tested by Q-Q plots per outcome measure for each age group. The candidate predictors included in the bivariate analyses were selected based on their association with lung function outcomes as reported in the literature.[4] These included anthropometric measures, PTB, LBW, infant wheezing, maternal smoking during pregnancy, maternal HIV (all treated as dichotomous variables), socioeconomic status and environmental exposures. Inclusion of variables in the final multivariable linear regression models was focused on growth variables (age, sex and length gain), and statistical significance (p<0.1). In the bivariate analyses, LBW and maternal smoking were consistently significant across measurement parameters, and were thus included in the models. Models were further tested for collinearity, and a variance inflation factor <5 was considered acceptable.
A strong correlation was observed between the growth variables e.g. birthweight and weight at test date and birth length and length at test date. Therefore, these variables were not entered simultaneously into regression models. Though birthweight is an important physiological predictor of infant lung function, we wanted to assess the effects of LBW as a risk factor for lung function. While maternal smoking was consistent, other risk factors (e.g. housing type, maternal income, etc.) appeared sporadically statistically significant. The variables included in our final models included age at test date, sex, length gain, LBW, and maternal smoking.
Ethics approval
Research ethics approval was obtained from the the University of KwaZulu-Natal Biomedical Research Ethics Committee (ref. no. BE431/17). Written informed consent was obtained from the parent or guardian of all infant participants at enrolment.
Results
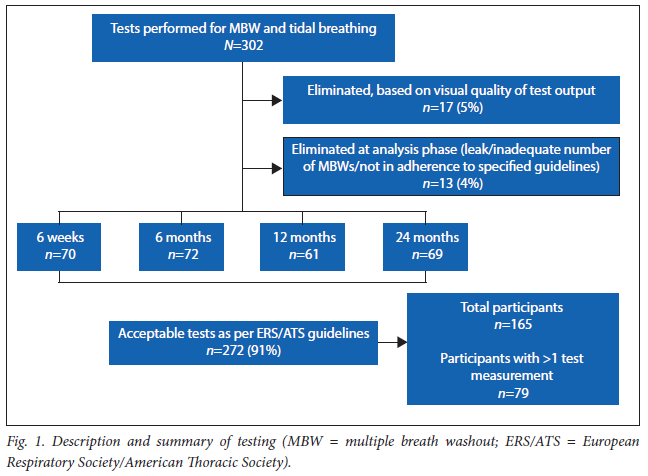
Of the 302 MBW and tidal breath assessments performed across varying age groups of 6 weeks, 6, 12 and 24 months, 272 tests (Fig. 1) were accepted, based on the visual quality of the test output and adherence to acceptability criteria as per the ERS/ATS guidelines.[15-16]
The overall mean (SD) birthweight of participants was 3.1 (0.6) kg, while birth length was 50.3 (3.65) cm, with equal sex distribution among participants (Table 1). None of the infants was HIV-infected even though 33% of mothers were HIVpositive (data not shown). There was a low prevalence of maternal smoking during pregnancy (5%). Most participants lived in formal housing (89%) and used electricity as their primary energy source (98%) (data not shown), with the overwhelming majority of mothers (94%) having a low annual income (USD <2 000). A not insubstantial number of participants were of LBW (10.9%), and the numbers presenting with this health status at different time points varied from 7.3% at 24 months to 15.7% at 6 weeks.
The tPTEF/tE parameter showed a large coefficient of variation (CV), implying a lower level of confidence in this test outcome (Table 2). The mean LCI was <7.4, consistent with a healthy cohort. The LCI provides a measure of an internally adjusted outcome (akin to the FEV1/ forced vital capacity (FVC) ratio in normal spirometry).
The Q-Q plots showed that the distribution of measured lung function data was approximately normal and appropriate for inclusion into linear models (data not shown). The association between measures of tidal breathing, MBW and potential predictors for variance in lung function parameters is presented in Table 3 for the respective age groups. Age at test date was statistically significant in the 6-week age group for TV, RR and tPTEF/tE. Females had consistently lower TV, MV, MTIF, and MTEF among all age groups though this was statistically significant for only certain age groups. The effect of postnatal length gain was inconsistent across age groups.
LBW was shown to have a consistent effect on tidal breathing parameters (TV, MV and flows), at 6 weeks, 6 months and 12 months, though not statistically significant across age groups (Table 3). LBW and maternal smoking effects were less evident at 24 months, though LBW was statistically significant at 12 months, and showed a consistent increase in effect, in the expected direction. Maternal smoking emerged as a consistent predictor in the expected direction for tPTEF/tE %. Although it generally contributed to a decline in FRC (apart from at 6 months), this was not statistically significant across any age group.
Discussion
In this study of infants from low socioeconomic communities in Durban, South Africa (SA), LBW and maternal smoking emerged as important predictors of infant lung function across different lung function parameters in various age groups. These losses were not insubstantial.
LBW was shown to be associated with lower FRC as well as TV, MV and tidal flows (MTEF and MTIF) at 6 weeks, and 6 and 12 months. However this was statistically significant at certain time points only. Though the impact of LBW on lung function is well documented'11 for older children, comparison between studies can be difficult because of heterogeneity in lung function, differences in exposures and outcome measures assessed.'31 There are no studies that have focused specifically on LBW and the outcome measures reported here. However, infant size, postnatal length gain and birthweight are known sources of variability in lung function. Lodrup Carlson et al.[19] found a decline in tidal breathing (TV and flows) measures with birthweight among 803 infants shortly after birth. Dezateux et al.[20]demonstrated that LBW for gestational age among 98 participants with a mean (SD) age of 6.6 (2.5) weeks was associated with reduced lung function when measured in early infancy prior to the onset of lower respiratory illness. This study further reported on reductions in forced expiratory flows or volumes as independent of postnatal weight or length. This supports evidence that impaired airway function in infants with LBW for gestational age is not only related or attributed to growth factors, but may also be due to intrauterine exposure factors. Intrauterine growth restrictions in fetal weight have been reported to affect the growth of the lungs and airways. [1] Our finding of reduced FRC (β -6.79 (95% CI -18.03 - 4.44 mL/kg)) in LBW infants, who are subject to increased risk for structural changes and premorbid lung function, further supports this. This novel finding suggests that infants with LBW are likely to have compromised respiratory function during the first 24 months of life, predisposing them to more severe consequences of acute respiratory infections.
Maternal smoking did not emerge as a consistent predictor of low lung function in our sample, unlike other studies, but this is likely due to the low prevalence of maternal smoking during pregnancy (4.9%) in our study. However, maternal smoking was associated with a decline in tPTEF/tE, a measure of airway conductance,[15] across age groups. In a study in Oslo, Norway, infants with a mean age of 2.7 days, exposed to maternal smoking in utero were shown to have an estimated -0.0021% change in tPTEF/tE (p=0.03) per unit increase in daily smoking, compared with non-exposed children.[19] Studies have demonstrated tPTEF/tE as an important predictor of respiratory morbidity in early childhood,[21] reduced tPTEF/tE precedes and predicts important childhood pulmonary outcomes, including wheeze and lung function.[22] It has also been shown that exposure to tobacco smoke has been linked to lung function in airway responsiveness (an indicator for asthma development)[6] and risk of wheezing in early life.[23]
We explored several socioeconomic and demographic factors associated with low-income communities, but were unable to relate these to the observed measures in tidal breathing and MBW measures. This could be attributed to the fact that most households had a low income (94%), and our sample lacked sufficient variability in socioeconomic status to investigate this variable. Even though 33% of infants were HIV-exposed, all HIV-positive mothers received antenatal antiretroviral treatment, and none of the infants were HIV-positive, which probably explained the absence of HIV-related findings.
Few studies report on infant lung function under non-sedation using similar testing methods and the same analytic software, limiting our ability for comparison.[11,17,24,25] The BILD study tested infants at 5 weeks, providing normative and reference values for a white Middle European population. [24] Similarly, a European and Australian multicentre study conducted lung function assessment in non-sedated infants aged 4 - 8 weeks, stratified by level of prematurity,[11] including 'full-term controls. The DCLHS cohort assessed lung function in healthy SA infants, aged 5 - 11 weeks,[17] from a low socioeconomic community, with the aim of providing reference data for tidal breathing and MBW measures. Compared with our findings, the mean (SD) TV at 6 weeks was lower in BILD and the European/Australian multicentre study, reporting 29.7 (5.9) mL/kg[24] and 32.4 (5.5) mL/ kg,[11] respectively, compared with our values and that reported by the DCLHS, of 33.7 (7.3) mL and 34.9 (6.9) mL/kg,[17] respectively.
Respiratory rate was on average within 1 SD across studies, whereas MV was higher in SA infants[24] from both studies in comparison with the European and multicentre studies.[11,17]
For the MBW measures in the 6-week age group, mean (SD) FRC was on average higher in the BILD study at 102 (16) mL.[24] Our findings (84.2 (18.1) mL) were closer to the range reported by the multicentre study (79.6 (14.5) mL) and the DCLHS (77.9 (17.0) mL).[17] Mean (SD) LCIs across all studies were within 1 SD of each other (BILD 6.75 (0.6);[24] MACE 6.91 (0.4); DCHS 7.2 (0.4);[17] and the European/Australian study 7.2 (0.5)).[11] Lung function is known to be dependent on specific population characteristics; therefore we observe similarities with the DCHLS study, but note some differences with BILD, which may be attributed to unmeasured sociodemographic differences. When comparing the data for the 12-month age group with the DCHLS study, on average our values were within 1 SD for TV, FRC and LCI.[25] Such differences may be attributed to anthropometric differences between studies, e.g. the infants from our study were on average taller by 2 cm and heavier by 1 kg, with a similar mean (SD) age of 2.2 (1.2) months in comparison with the DCHLS study, with a mean (SD) age of 12.6 (1.0) months, respectively.
A major strength of our study was the use of state-of-the-art measures in infant lung function assessment in a low-income setting. We were further able to undertake assessments at varying age groups (6 weeks, 6, 12 and 24 months), overcoming challenges in sleep and behavioural patterns between age groups. Lung function assessment without sedation among these age groups is a costly and timeintensive process, and we were able to achieve a high success rate on testing, further ensuring quality control in the test outputs through blind analyses.
Among the study limitations were the small sample size and distribution of the sample across age ranges, which requires cautious interpretation of the results. The characteristics of our study population and the lung function parameter results were comparable to prior studies for selected age groups.[4,17,24] The assessment of lung function in infancy and our understanding and interpretation of these outcome measures still requires further technical optimisation, as even in studies with larger sample numbers and with longer observation periods, the observed inter-individual variability of identified outcome measures was not adequately explained.
In conclusion, our study adds to the growing body of knowledge on infant lung function generally, and our key finding of LBW and its effect on several lung function parameters is particularly relevant in low socioeconomic communities.
Declaration. Lung function testing in infant participants was performed without sedation and in compliance with the principles of the Declaration of Helsinki and applicable ethical guidelines on research involving human participants.
Acknowledgements. The authors thank all the participants who kindly consented for their children to be involved in our study and the MACE study team for their efforts in data collection. We wish to thank Prof. Peter Sly and the DCLHS team, namely Prof. Heather Zar, Dr Diane Gray, Ms Lauren Willemse and Mr Carven Jacobs, for their assistance inthe initial training of our team in the early developmental phase of our study, and provision of the necessary standard operating procedures and support when required, enabling us to smoothly conduct our testing in a standardised manner.
Author contributions. SM, RN and PMJ conceptualised the study aims, objectives and methods. SM, RN, PMJ and KA were responsible for study implementation. MR and ACO provided intellectual contributions on the methods and interpretation of results. HKC and AAM contributed to the statistical methods and analysis. SM, KA and GN were responsible for lung function testing and data acquisition. All authors contributed towards the interpretation of the data and have read and approved the final manuscript.
Funding. This study was supported by the MACE project finders, the National Research Foundation (Grant 90550), the South African Medical Research Council (SAMRC), AstraZeneca Trust and the University of KwaZulu-Natal's Flagship funding. We further acknowledge the support of the Swiss-African Research Cooperation (SARECO) for a fellowship award (to SM) and the SAMRC Researcher Development Grant (to SM).
Conflicts of interest. None.
References
1. Hoo A-F, Stocks J, Lum S, et al. Development of lung function in early life: Influence of birth weight in infants of nonsmokers. Am J Respir Crit Care Med 2004;170(5):527-533. https://doi.org/10.1164/rccm.200311-1552OC [ Links ]
2. Goldizen FC, Sly PD, Knibbs LD. Respiratory effects of air pollution on children. Pediatr Pulmonol 2016;51(1):94-108. https://doi.org/10.1002/ppul.23262 [ Links ]
3. Korten I, Ramsey K, Latzin P. Air pollution during pregnancy and lung development in the child. Paediatr Respir Rev 2017;21(1):38-46. https://doi.org/10.1016/j.prrv.2016.08.008 [ Links ]
4. Gray D, Willemse L, Visagie A, et al. Determinants of early-life lung function in African infants. Thorax 2017;72(5):445-450. https://doi.org/10.1136/thoraxjnl-2015-207401. [ Links ]
5. Horsley A. Lung clearance index in the assessment of airways disease. Respir Med 2009;103(6):793-799. https://doi.org/10.1016/j.rmed.2009.01.025 [ Links ]
6. Macleod KA, Horsley AR, Bell NJ, Greening AP, Innes JA, Cunningham S. Ventilation heterogeneity in children with well controlled asthma with normal spirometry indicates residual airways disease. Thorax 2009;64(1):33-37. https://doi.org/10.1136/thx.2007.095018. [ Links ]
7. Horsley AR, Gustafsson PM, Macleod KA, et al. Lung clearance index is a sensitive, repeatable and practical measure of airways disease in adults with cystic fibrosis. Thorax 2008;63(2):135-140. https://doi.org/10.1136/thx.2007.082628 [ Links ]
8. Aurora P, Bush A, Gustafsson P, et al. Multiple-breath washout as a marker of lung disease in preschool children with cystic fibrosis. Am J Respir Crit Care Med 2005;171(3):249-256. https://doi.org/10.1164/rccm.200407-895OC [ Links ]
9. Gustafsson PM, Aurora P, Lindblad A. Evaluation of ventilation maldistribution as an early indicator of lung disease in children with cystic fibrosis. Eur Respir J 2003;22(6):972-979. https://doi.org/10.1183/09031936.03.00049502 [ Links ]
10. Hülskamp G , Pillow JJ, Dinger J, Stocks J. Lung function tests in neonates and infants with chronic lung disease of infancy: Functional residual capacity. Pediatr Pulmonol 2006;41(1):1-22. https://doi.org/10.1002/ppul.20318 [ Links ]
11. Hülskamp G, Lum S, Stocks J, et al. Association of prematurity, lung disease and body size with lung volume and ventilation inhomogeneity in unsedated neonates: A multicentre study. Thorax 2009;64(3):240-245. https://doi.org/10.1136/thx.2008.101758 [ Links ]
12. Latzin P, Roosli M, Huss A, Kuehni CE, Frey U. Air pollution during pregnancy and lung function in newborns: A birth cohort study. Eur Respir J 2009;33(3):594-603. https://dx.doi.org/10.1183/09031936.00084008 [ Links ]
13. Jeena PM, Asharam K, Mitku AA, Naidoo P, Naidoo RN. Maternal demographic and antenatal factors, low birth weight and preterm birth: Findings from the Mother and Child in the Environment (MACE) birth Durban, South Africa. BMC Pregnancy Childbirth 2020;20(1):628. https://doi.org/10.1186/s12884-020-03328-6 [ Links ]
14. World Health Organization. Child growth standards. WHO Multicentre Growth Reference Study Group. https://www.who.int/tools/child-growth-standards/who-multicentre-growth-reference-study (accessed 29 September 2023). [ Links ]
15. Bates J, Schmalisch G, Filbrun D, Stocks J. Tidal breath analysis for infant pulmonary function testing. ERS/ATS Task Force on Standards for Infant Respiratory Function Testing. European Respiratory Society/ American Thoracic Society. Eur Respir J 2000;16(6):1180-1192. https://doi.org/10.1034/j.1399-3003.2000.16f26.x [ Links ]
16. Robinson PD, Latzin P, Verbanck S, et al. Consensus statement for inert gas washout measurement using multiple- and single- breath tests. Eur Respir J 2013;41:507-522. https://doi.org/10.1183/09031936.00069712 [ Links ]
17. Gray D, Willemse L, Visagie A, et al. Lung function and exhaled nitric oxide in healthy unsedated African infants. Respirology 2015;20(7):1108-1114. https://doi.org/10.1111/resp.12579 [ Links ]
18. World Health Organization. Global Nutrition Targets 2025: Low Birth Weight Policy Brief. Geneva: WHO, 2014. [ Links ]
19. Lodrup Carlsen K, Jaakkola J, Nafstad P, Carlsen K. In utero exposure to cigarette smoking influences lung function at birth. Eur Respir J 1997;10(8):1774-1779. https://doi.org/10.1183/09031936.97.10081774 [ Links ]
20. Dezateux C, Lum S, Hoo AF, Hawdon J, Costeloe K, Stocks J. Low birth weight for gestation and airway function in infancy: Exploring the fetal origins hypothesis. Thorax 2004;59(1):60-66. https://doi.org/10.1136/thx.2003.awjan [ Links ]
21. Yuksel B, Greenough A, Giffin F, Nicolaides KH. Tidal breathing parameters in the first week of life and subsequent cough and wheeze. Thorax 1996;51(8):815-818. https://doi.org/10.1136/thx.51.8.815 [ Links ]
22. Young S, Arnott J, O'Keeffe P, le Souef P, Landau L. The association between early life lung function and wheezing during the first 2 years of life. Eur Respir J 2000;15(1):151-157. https://doi.org/10.1183/09031936.00.15115100 [ Links ]
23. Dezateux C, Stocks J, Dundas I, Fletcher ME. Impaired airway function and wheezing in infancy. Am J Respir Crit Care Med 1999;159(2):403-410. https://doi.org/10.1164/ajrccm.159.2.9712029 [ Links ]
24. Fuchs O, Latzin P, Thamrin C, et al. Normative data for lung function and exhaled nitric oxide in unsedated healthy infants. Eur Respir J 2011;37(5):1208-1216. https://doi.org/10.1183/09031936.00125510 [ Links ]
25. Gray DM, Turkovic L, Willemse L, et al. Lung function in African infants in the Drakenstein Child Health Study: Impact of lower respiratory tract illness. Am J Respir Crit Care Med 2017;195(2):212-220. https://doi.org/10.1164/rccm.201601-0188OC [ Links ]
 Correspondence:
Correspondence:
S Muttoo
sheena.muttoo@gmail.com
Accepted 3 August 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}