










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.3 Pretoria Sep. 2023
http://dx.doi.org/10.7196/sajch.2023.v17i3.1911
RESEARCH
A baseline assessment of developmental delays among children under 5 years in a high-HIV-prevalence setting in the Cape Metropole
E ChademanaI; U MalulekeII; B van WykIII
IPhD; Programmes Director, One to One Africa Children's Fund, Cape Town South Africa
IIMA (Res Psychol); School of Public Health, Faculty of Community Health Sciences, University of the Western Cape, Cape Town South Africa
IIIDPhil; School of Public Health, Faculty of Community Health Sciences, University of the Western Cape, Cape Town South Africa
ABSTRACT
BACKGROUND: More than 200 million children globally are at risk of not achieving the full developmental potential owing to multiple factors. HIV exposure is of particular concern as evidence suggests that children born to mothers who are HIV-positive are likely to experience developmental delays. Furthermore, the psychosocial and economic impacts of HIV, such as parental illness, poor mental health, poverty and malnutrition, also affect children's development
OBJECTIVE: To assess and address the developmental challenges faced by children aged 2 - 5 years living in high-HIV prevalence settings through a toy-based rehabilitation intervention and to analyse the prevalence and nature of developmental delays observed in these children using the Ages and Stages Questionnaires (ASQ-3
METHODS: In response, the Bright Start programme was developed and implemented to target children living in high HIV-prevalence settings. In 2019, a pilot project was implemented with 90 caregiver-child dyads in Cape Town, South Africa. A baseline survey was conducted to assess developmental progression for all the children (N=141) in the care of the 90 caregivers using the Ages and Stages Questionnaires (ASQ-3) for children aged 24, 36, 48 and 60 months
RESULTS: Findings showed that 64% of children had delays in at least one domain and 37% had multiple delays. More than half of the children had developmental delays in fine motor skills (51%), while gross-motor and problem-solving delays were reported for 30% and 26% of children, respectively. Communication and personal-social domain delays were observed in 17% and 14% of children, respectively
CONCLUSION: The prevalence of developmental delays among children in the programme was alarmingly high. These findings indicate that developmental delay is a serious concern for children living in high-HIV-prevalence settings. Early identification and timeous referrals of children with developmental delays are critical and may enable children to reach their full developmental potential
Keywords: cognitive development; early stimulation; developmental delay; HIV; early childhood development; Ages and Stages Questionnaire.
The first years of a child's life are critical - it is at this stage that children develop the foundation of their cognitive, social, emotional and physical skills. Cognitive development is particularly important during the early years as 90% of a child's critical brain development happens by the age of 5 years. Children develop skills in attention, conceptualisation and memory, visual-motor, as well as logic and reasoning skills.[1] These skills are important for reading, learning, thinking and problem solving. Several studies link early childhood development to adult health and wellbeing.[2] Children who reach their full developmental potential are likely to have better educational outcomes and increased earnings in adulthood.[3] However, >200 million children globally are at risk of not achieving their full developmental potential owing to multiple factors, including poverty, poor health and access to healthcare, malnutrition, HIV and low levels of home stimulation.[1] Many of these children reside in South Africa (SA); according to recent statistics, half of children under 4 years (50.2%) in SA are not attending any early childhood development programme and therefore do not have access to adequate stimulation.[4] HIV infection and exposure are of particular concern as SA has the highest number of people living with HIV in the world, with an estimated 7.8 million people in SA living with HIV in 2020.[5] There is evidence to suggest that children born from mothers who are HIV-positive are likely to experience developmental delays in language, motor, and cognitive development.[6-10] A systematic review of studies on the effects of HIV on child development reported detrimental effects of HIV infection on neurocognitive development of children.[11] Developmental deficits were identified in the areas of cognition, fine and gross motor development as well as receptive and expressive language development. If not addressed, these developmental delays can persist throughout childhood into adulthood.
The Bright Start programme
The Bright Start programme was implemented in Crossroads, a peri-urban community outside Cape Town, where poverty, unemployment and HIV are rife. Caregivers of children exposed to HIV received training on how to play with specific toys and games with children (under 5 years) in their care to stimulate cognitive and motor skills development. The pilot project, which included caregiver training, took place between May and September 2019 over 8 sessions (every second week). The two-week period between sessions allowed time for caregivers to practice the play with their child/children with a specific toy before moving onto the next toy, which was introduced during the following session. The present paper reports on the baseline assessment of the participating caregivers' children's development relative to age, using the Ages and Stages Questionnaire 3 (ASQ-3).[12]
Methods
Participants
Caregivers of children between 2 and 5 years of age were recruited from the Crossroads Clinic. The clinic provides primary health care and includes a large paediatric HIV and antiretroviral therapy (ART) centre. Criteria for inclusion of caregivers as participants were: (i) had to be parents, relatives or any household member who spent time with/ looked after the child during the day; (ii) children had to be between the ages of 2 and 5 years; (iii) resident in the greater Nyanga area; (iv) access healthcare services at the Crossroads 2 clinic; and (v) be available and willing to attend all sessions.
Instrument
The ASQ-3 is a developmental screening tool for children between 2 and 60 months of age. The tool consists of 21 questionnaires, one for each age group from 2 months to 60 months and each questionnaire has 30 items to assess developmental milestones in five key domains, i.e. communication, gross-motor, fine-motor, problem-solving and personal-social developmental skills. The responses for items are 'yes', 'sometimes' and 'not yet' and scored as 10, 5, and 0, respectively. The maximum score for each domain is 60. The ASQ-3 has well-established psychometric properties as several studies have confirmed its test-retest reliability, validity, sensitivity and internal consistency.[12-15] Furthermore, the feasibility of the tool for use among South African children has been established.[13] It is a low-cost developmental screening tool designed for universal application.[14]
Ethics
Ethics approval for the study was obtained from the Biomedical Research Ethics Committee of the University of the Western Cape (ref. no. BM19/3/14). Written informed consent was obtained from all participants. Consent to recruit caregiver-child dyads was obtained from Crossroads 2 clinic and 90 caregiver-child dyads were recruited. Prior to commencement of toy sessions, a baseline survey was conducted using the ASQ-3 for children aged 24, 36, 48 and 60 months in May 2019. Similar to other studies in groups with low literacy levels,[15] trained facilitators supported the self-assessment. Facilitators explained the ASQ-3 step-by-step by talking the caregivers through each question.
Data analysis
Raw data were entered into Microsoft Excel (Microsoft Corporation, USA) and screened for errors and missing values. Domain scores were calculated using the ASQ-3 score key. Data were then coded into the intervals using the SA cut off scores. Developmental delay within age-appropriate categories (24, 36, 48 and 60 months) was analysed for each of the five domains. Descriptive analysis for all the domains was also conducted. Chi-square statistics were calculated for each domain using SPSS version 24 (IBM Corp., USA). A p-value <0.05 was considered statistically significant.
Results
Overall, 141 caregiver-child dyads participated in the survey, including 90 children in the programme and 51 siblings. After cleaning, 2 questionnaires were eliminated owing to errors. A total of 139 children were included in the study. Children were grouped into four age groups: (i) 24 months for children between 24 and 35 months; (ii) 36 months for children between 36 and 47 months; (iii) 48 months for children between 48 and 59 months; and ( iv) 60 months for children between 60 and 66 months. There were 40, 24, 41 and 34 children in the 24-, 36-, 48- and 60-months age groups, respectively.
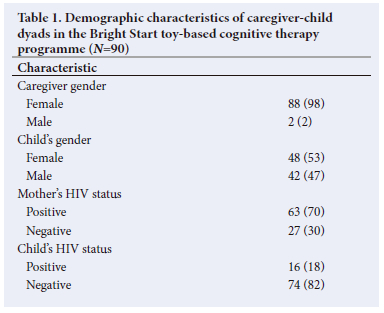
Table 1 presents the demographic characteristics of the 90 caregiver-child dyads. Only two caregivers were male; the remainder (98%) were female. The participating caregivers reported that 70% of the biological mothers of the children were HIV-positive. There was an equal distribution in sex of the index children in the study (females 53% and males 47%). Just under a fifth (18%) of index children were reported to be HIV-positive. However, in the subsequent administration of the assessment of children's development relative to age, the caregiver respondents reported for an additional 51 siblings who were in their care, as well as the index children for which they entered the programme, resulting in a total of 141 child responses.
Caregivers' responses to the ASQ-3 questionnaire are shown in Table 2.
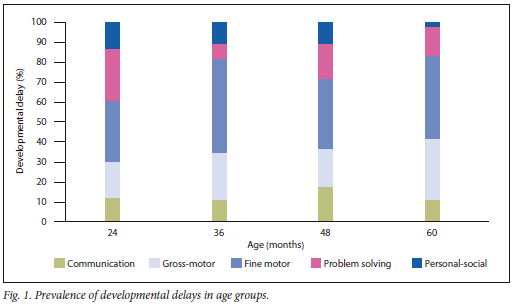
Almost two-thirds (64%) of children in the study were reported to have delays in at least one developmental area, as shown in Fig. 1. The most common delay across all age groups was in the development of fine-motor skills. In the 24 months age group, 46% and 40% of children had reported delays in the development of fine-motor and problem-solving skills, respectively. More than half of the children in the 36- and 48-months age groups had similar developmental delays, i.e. 58% and 56%, respectively, while 46% of children in the 60 months age group had delays in fine-motor skills development. Children who were 60 months old were mostly on track in the fine-motor skills domain. There were significant differences in developmental delays across the age groups in the problem-solving (p=0.001) and personal-social domains (p=0.043) (Table 2).
Communication
Overall, 82% of children had no communication concerns and only 18% of children were reported as having some communication concerns. Most (88%) children who were 60 months old were reported as having no communication delays; whereas 27% of children who were 48 months of age were reported as having delays in the development of communication skills.
Gross motor
Most participants indicated that there was 'no concern' regarding the gross-motor skills developmental area. More than two-thirds (70%) of all children in the study were reported as having no gross motor skills concerns. A third (34%) of children in the 60 months age group were reported as not having the appropriate gross motor functioning for their age.
Fine motor
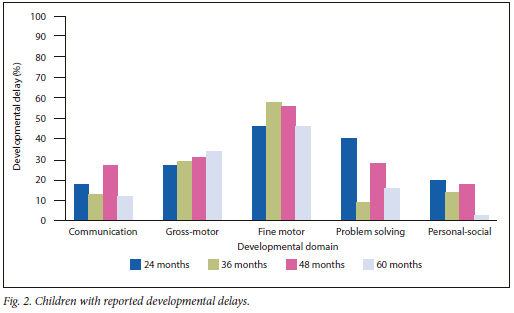
Fine-motor skills developmental delays were concerning as the number of children reported to have concerns increased compared with the aforementioned two domains. More than half of the participants (52%; n=67/130) were reported to have delayed finemotor skills development. This was particularly high in the 36-(58%) and 48-month (56%) age groups (Fig. 2). Sixty percent (60%) of children in the 24-month age group were unable to string beads, macaroni, and pasta onto a string/shoelace, while drawing was a difficult task for the 36-months and 48-months age group.
Problem solving
There were significant differences in development across the age categories in the problem-solving domain (p=0.001). Specifically, children at 36 months displayed a higher likelihood of being developmentally on track 91% (n=21/23). Conversely, children aged 24 months had the lowest performance, with only 60% (n=24/40) meeting the developmental criteria for this domain. Furthermore, 72% (n=28/39) of children aged 48 months and 84% (n=26/31) of children aged 60 months were found to be on track in their problem-solving abilities.
Personal-social
Overall, 86% (n=114/133) of the children were reported to have attained age-appropriate personal-social developmental skills. Almost all the children in the 60 months age group (97%; n=30/31) were reported as having no personal-social developmental concerns and were developmentally on track. There was, however, significant differences in development across the age groups (p=0.043). This is attributed to children in the 24 months (20%; n=8/40) and 48 months (18%; n=7/40) age groups who were reported to have delays in this domain (Fig. 2).
Discussion
The aim of the current study was to assess the developmental status of children recruited in the Bright Start programme prior to receiving any intervention. Our findings indicate that the number of children with suspected developmental delays was comparatively higher than their peers in similar contexts, with 64% having at least one delay and 37% displaying multiple delays. Consistent with other studies of children exposed to HIV, delays in the development of age-appropriate communication skills were reported for 25 out of 136 children and ranged between 12% and 27% across all age groups. In the Democratic Republic of the Congo (DRC), HIV-exposed children had higher levels of delays in language expression compared with HIV-unexposed children.[8] In comparison with other studies, it is noteworthy that HIV-unexposed children in our study also displayed elevated rates of developmental delays, suggesting the presence of additional contributing factors. [13,15-17] In Kerstjens et al'.s study[18] of 2-year-old preterm children, 8% were found to have communication delays and, in a more recent study by Zhang et al.,[19] only 4.3% had delays in this domain.
The fine-motor domain had the highest prevalence of developmental concerns among the age groups, ranging between 46% and 58%, and affecting 67 out of 130 children. These results are comparable with other studies of HIV-exposed children ranging between 53% and 85%.[7,9,20] In other studies[16,18,19] of HIV-unexposed children, delays in fine-motor skills development ranged from 5 to 10%. In the present study, suspected delays in gross-motor functioning ranged between 27% and 34 % (n=41/135). Gross- and fine-motor developmental delays in HIV-exposed children have been noted in several studies.[7,8,10,21] In SA in 2008, Baillieu and Potterton[9] reported gross-motor delays in 85% of their cohort. Similarly, a study in the DRC, reported that 28% of HIV-exposed children had severe delays in motor development.[8] In their SA study, Ferguson and Jelsma (2008)[10] found 66.6% of children with significant motor delays and 23.5% with mild delays. Delays in problem-solving skills development ranged between 9% and 40% across all age groups. Older children between 36 and 60 months old, did not have significant delays in their problem-solving skills. Children who were 24 months old were reported as having the most delays as 40% of the children were reported as having delays. This is comparably higher than the other studies that had 6% and 9.7% of children in the same age.[18-19] In a study in Ghana,[22] 10.6% of children in the study had delays and a further 10% were reported as being at-risk of delay. In our study, 3 -20% of children had delays in the personal-social domain. Most children (n=114/133) displayed age-appropriate personal-social development. Almost all children who were 60 months old (97%) had no developmental concerns. In the Ghanaian study,[22] 12.4% of children had delays in the personal-social domain and 14.5% were at risk of delay.
Overall, we found more suspected developmental delays across all five domains in children who were 24 and 48 months old, indicating poorer development in these two age groups. The ASQ data confirm that HIV-exposed in this low-income community are at risk of poor developmental outcomes. Furthermore, 37% of children in our cohort were reported to have delays in more than one area, indicating global developmental delay (GDD), i.e. significant delays in two or more domains,[22] as opposed to isolated single-domain delays. This corroborates previous studies reporting high levels of developmental delay in HIV-exposed children.[6-7,19,23] With the implementation of prevention of mother-to-child transmission (PMTCT) of HIV interventions, the number of HIV-exposed and uninfected (HEU) children will increase. It is therefore imperative that HIV-exposed children receive clinical assessments to identify significant developmental delays early and are enrolled in ECD programmes. There is confounding evidence that early interventions incorporating brain stimulation and learning activities have the potential to rehabilitate delayed skills thereby enhancing children's developmental competence.[19]
These findings should be interpreted with caution, as the delays were reported by caregivers and no clinical assessments were conducted. We were not able to ascertain whether HIV infection was the confounding factor for developmental delay.
Study strengths and limitations
The strength of this study was that it helped to identify children with potential developmental challenges who required further assessment. The main limitation of the study was that we were unable to link the caregivers' and children's HIV status, owing to anonymity in completion of the ASQ assessments. Furthermore, the small sample size for each age group limited statistical analysis. Another limitation was that the survey responses were based on the caregivers' recollection and therefore, relied heavily on the caregivers' memory and on how well they knew their children. The responses were also based on their self-assessment of whether their child's development was of concern or not, which is subjective. It should be noted that the ASQ-3 is a screening instrument; therefore, there may be an overestimation of developmental delays. Our study does not explore factors contributing to developmental delays in children as the objective of the survey was to provide a descriptive overview of children recruited for the Bright Start programme.
Conclusion
Our findings indicate that developmental delay is a serious concern for HIV-exposed children in this community sample. The prevalence of delays among children in the programme was alarmingly high. Early identification and timeous referrals of children with developmental delays is critical and appropriate interventions may enable children to reach their full developmental potential. Furthermore, developmental interventions for children should target development of motor and problem-solving skills. The association between developmental delay and HIV exposure among HEU children, as well as the as the association between HIV status and developmental outcomes, needs further investigation. The next phase of the programme will assess the impact of the toy-based stimulation on children's developmental outcomes. Association between developmental outcomes, children's HIV exposure and caregiver demographics - HIV status, age, education, and household income, will be examined.
Declaration. None.
Acknowledgements. The authors would like to acknowledge the caregivers and their children who participated in the programme, the University of the Western Cape for its assistance in the study, as well as the One-to-One Africa Children's Fund Team for their support in implementation of the programme.
Author contributions. All authors participated in the development of this paper. The study's implementation was supervised by EC, BvW and UM. EC initiated the paper's initial draft, which received input and revisions from all authors. All authors collaborated on the study's design, execution, and interpretation of results. The final version of the paper was reviewed and approved for submission by all authors.
Funding. This study was made possible through the generous funding from One-to-One Children's Fund UK and their philanthropic flinders.
Conflicts of interest. None.
References
1. Black MM, Walker SP, Fernald LC, et al. Early childhood development coming of age: Science through the life course. Lancet 2017;389(10064):77-90. https://doi.org/10.1016%2Fs0140-6736%2816%2931389-7 [ Links ]
2. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B, International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007;369(9555):60-70. https://doi.org/10.1016%2Fs0140-6736%2807%2960032-4 [ Links ]
3. Hoddinott J, Maluccio JA, Behrman JR, Flores R, Martorell R. Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. Lancet 2008;371(9610):411-416. https://doi.org/10.1016%2Fs0140-6736%2808%2960205-6 [ Links ]
4. Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, Carter JA, International Child Development Steering Group. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007;369(9556):145-157.https://doi.org/10.1016%2Fs0140-6736%2807%2960076-2 [ Links ]
5. Statistics South Africa. General Household Survey 2019. Pretoria: StatsSA, 2021. http://www.statssa.gov.za/publications/P0318/P03182019.pdf (accessed 09 June 2021). [ Links ]
6. Sherr L, Hensels IS, Tomlinson M, Skeen S, Macedo A. Cognitive and physical development in HIV-positive children in South Africa and Malawi: A community-based follow-up comparison study. Child Care Health Dev 2018;44(1):89-98. https://doi.org/10.1111%2Fcch.12533 [ Links ]
7. Hutchings J, Potterton J. Developmental delay in HIV-exposed infants in Harare, Zimbabwe. Vulnerable Children Youth Studies 2014;9(1):43-55. https://doi.org/10.1080/17450128.2013.778440 [ Links ]
8. Van Rie A, Mupuala A, Dow A. Impact of the HIV/AIDS epidemic on the neurodevelopment of preschool-aged children in Kinshasa, Democratic Republic of the Congo. Pediatrics 2008;122(1):e123-e128. https://doi.org/10.1542%2Fpeds.2007-2558 [ Links ]
9. Baillieu N, Potterton J. The extent of delay of language, motor, and cognitive development in HIV-positive infants. J Neurol Physical Ther 2008;32(3):118-121. https://doi.org/10.1097%2Fnpt.0b013e3181846232 [ Links ]
10. Ferguson G, Jelsma J. The prevalence of motor delay among HIV infected children living in Cape Town, South Africa. Int J Rehab Res 2009;32(2):108-114. https://doi.org/10.1097%2Fmrr.0b013e3283013b34 [ Links ]
11. Sherr L, Mueller J, Varrall R. A systematic review of cognitive development and child human immunodeficiency virus infection. Psychol Health Med 2009;14(4):387-404. https://doi.org/10.1080%2F13548500903012897 [ Links ]
12. Squires J, Katzev A, Jenkins F. Early screening for developmental delays: use of parent-completed questionnaires in Oregon's Healthy Start Program. Early Child Dev Care 2015;172(3):275-282. https://doi.org/10.1080/03004430290030804 [ Links ]
13. Van Heerden A, Hsiao C, Matafwali B, Louw J, Richter L. Support for the feasibility of the ages and stages questionnaire as a developmental screening tool: A cross-sectional study of South African and Zambian children aged 2 - 60 months. BMC Pediatr 2017;17(55):1-9. https://doi.org/10.1186%2Fs12887-017-0802-3 [ Links ]
14. Small JW, Hix-Small H, Vargas-Baron E, Marks KP. Comparative use of the Ages and Stages Questionnaires in low-and middle-income countries. Dev Med Child Neurol 2019;61(4):431-443. https://doi.org/10.1111%2Fdmcn.13938 [ Links ]
15. Hsiao C, Richter L, Makusha T, Matafwali B, Heerden A, Mabaso M. Use of the ages and stages questionnaire adapted for South Africa and Zambia. Child: Care Health Dev 2016;43(1):59-66. https://doi.org/10.1111%2Fcch.12413 [ Links ]
16. Riou EM, Ghosh S, Francoeur E, Shevell MI. Global developmental delay and its relationship to cognitive skills. Dev Med Child Neurol 2009;51(8):600-606. https://doi.org/10.1111%2Fj.1469-8749.2008.03197.x [ Links ]
17. Catino E, Di Trani M, Giovannone F, et al. Screening for developmental disorders in 3- and 4-year-old Italian children: A preliminary study. Front Pediatr 2017;5(181):1-8 https://doi.org/10.3389%2Ffped.2017.00181 [ Links ]
18. Kerstjens JM, Nijhuis A, Hulzebos CV, et al. The Ages and Stages Questionnaire and neurodevelopmental Impairment in two-year-old preterm-born children. PLoS ONE 2015;10(7):1-14 e0133087. https://doi.org/10.1371%2Fjournal.pone.0133087 [ Links ]
19. Zhang J, Guo S, Li Y, et al. Factors influencing developmental delay among young children in poor rural China: A latent variable approach. BMJ Open 2018;8(8):1-9 e021628. https://doi.org/10.1136%2Fbmjopen-2018-021628 [ Links ]
20. Potterton J, Stewart A, Cooper P, Becker P. The effect of a basic home stimulation programme on the development of young children infected with HIV. Dev Med Child Neurol 2010;52(6):547-551. https://doi.org/10.1111%2Fj.1469-8749.2009.03534.x [ Links ]
21. Whitehead N, Potterton J, Coovadia A. The neurodevelopment of HIV-infected infants on HAART compared to HIV-exposed but uninfected infants. AIDS Care 2014;26(4):497-504. https://doi.org/10.1080%2F09540121.2013.841828 [ Links ]
22. Bello AI, Quartey JN, Appiah LA. Screening for developmental delay among children attending a rural community welfare clinic in Ghana. BMC Pediatr 2013;13(1):1-7 https://doi.org/10.1186%2F1471-2431-13-119 [ Links ]
23. Sherr L, Croome N, Castaneda KP, Bradshaw K, Romero RH. Developmental challenges in HIV-infected children: An updated systematic review. Children Youth Services Rev 2014;45(1):74-89. https://doi.org/10.1016%2Fj.childyouth.2014.03.040 [ Links ]
 Correspondence:
Correspondence:
E Chademana
emma.c@onetoonechildrensfund.org
Accepted 17 May 2023


{kind=link}