










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.3 Pretoria Sep. 2023
http://dx.doi.org/10.7196/sajch.2023.v17i3.1915
RESEARCH
Iodine status, including breastmilk iodine content, of lactating mothers and their infants aged 0 to 6 months in Vhembe and Mopani districts of the Limpopo province, South Africa
S C HlakoI; L F MushaphiII; N S MabapaII; J BaumgartnerIII
IMSc; Department of Life and Consumer Sciences, College of Agriculture and Environmental Sciences, University of South Africa, Johannesburg, South Africa
IIPhD; Department of Nutrition, Faculty of Health Sciences, University of Venda, Thohoyandou, South Africa
IIMSc; Department of Nutrition, Faculty of Health Sciences, University of Venda, Thohoyandou, South Africa
IIIPhD; Department of Nutritional Sciences, Faculty of Life Sciences and Medicine, King's College London, United Kingdom
ABSTRACT
BACKGROUND: Both iodine deficiency and excess may affect lactating women and their infants. In Limpopo Province, South Africa (SA), there are no data on the iodine status of individuals in these vulnerable groups
OBJECTIVE: To determine the iodine status, including breastmilk iodine content, of lactating mothers and their infants aged 0 - 6 months in Vhembe and Mopani districts, Limpopo, SA
METHODS: A cross-sectional descriptive study in the quantitative domain was undertaken in Vhembe and Mopani districts. Mother-infant pairs were randomly selected. Breastmilk iodine content (BMIC), urinary iodine content (UIC) of infants, UIC of mothers, household (HH) salt iodine content (SIC) and water iodine content (WIC). The iodine nutrition knowledge of mothers was determined
RESULTS: The median (interquartile range (IQR)) of BMIC among lactating mothers in Vhembe and Mopani was 102 (62 - 179.7) µg/L and 150.4 (89.4 - 201.7) µg/L, respectively. The median (IQR) UIC of mothers in Vhembe and Mopani was 96.3 (54.8 - 154.8) µg/L and 137.9 (72 - 212.4) µg/L, respectively. The median UIC of infants was 217.7 (107.1 - 409.9) and 339.8 (162.9 - 490.3) µg/L in Vhembe and Mopani, respectively. There was a significant difference between SIC of coarse and fine salt in both districts. Lactating mothers in both areas had limited iodine nutrition knowledge
CONCLUSION: The results suggest that iodised salt is a major contributor to iodine status in lactating mothers and their infants. Our results also show that the salt iodisation programme in SA supplies sufficient iodine for children, women of reproductive age, lactating mothers and breastfed infants
Dietary iodine is essential for the synthesis of thyroid hormones (thyroxine and triiodothyronine) and is required for normal brain development, growth and metabolism. [1] Both low and high iodine intake can lead to thyroid dysfunction.[2] Infants may be vulnerable to iodine deficiency and iodine excess because the fetal and newborn thyroid has limited iodine stores and adapts poorly to high levels of iodine.[3] Excess iodine may result in hypothyroidism in newborns.[4] Little is known about the effects of high iodine intake on thyroid function in breastfed infants.
In South Africa (SA), 77% of households are using adequately iodised salt.[5] It evident that the salt iodisation programmes have made remarkable progress in improving iodine status in the country and worldwide. Pearce et al.[1] points out that if salt iodine fortification is poorly monitored, the iodine intake may be excessive. In SA, house and retail salt should be iodised at a concentration of 35 - 65 ppm at the production site.[6] The legislation does not involve fortification of agricultural salt. Mabapa et al.[7] has reported that local people from Vhembe District in Limpopo Province, SA, prefer agricultural salt because it is cheaper to buy.
The mandatory salt iodisation programme in SA remarkably improved the iodine status of women of reproductive age and school children. In 2005, the SA Food Based National Food
Consumption survey (NFCS-FB-I) reported a median urinary iodine concentration of 215 µg/L in school children and 177 µg/L in women of reproductive age signifying adequate iodine intake.[8] Recent data on iodine status of pregnant women and school children reported a maternal median UIC of 164 µg/L and UIC of 386 µg/L for school children.[9] There is still a gap in iodine nutrition, as a third of South Africans do not have access to adequately iodised salt.[10] Furthermore, few studies exist on iodine status of lactating women and infants.
Breastfed infants depend solely on iodine from breastmilk for the synthesis of thyroid hormones and to build up iodine stores.[11] BMIC are determined by the maternal iodine intake. Osei et al.[12] reported a median (interquartile range (IQR)) BMIC of 179 µg/L (126 - 269 µg/L) from mothers residing in SA townships, i.e. Ikageng and Promosa in the Kenneth Kaunda District municipality, Northwest Province, SA.
A median UIC of <100µg/L indicates insufficient iodine intake in lactating women and in children <2 years.[6] To date, few studies have been conducted to assess the iodine status of lactating mothers and their breastfed infants. The present study assessed the BMIC, iodine status of mothers and breastfed infants in Vhembe and Mopani districts, Limpopo Province, SA. Potential predictors of UIC and BMIC were explored.
Methods
The present study included 300 mother-infant pairs from clinics in Vhembe and Mopani districts from a total of 15 clinics: 10 clinics in Vhembe (with the highest number of mother-infant pairs attending growth monitoring) and 5 in Mopani were randomly selected. The study commenced in March 2018 and was completed in September 2018. A validated questionnaire was administered to obtain demographic data, salt consumption patterns and iodine nutrition knowledge. The contents of the questionnaire included the following: maternal age, whether the infant was exclusively breastfed or not, the type of salt used and the frequency of salt consumption. A single-spot urine sample from lactating mothers (n=232) and infants (n=203), breastmilk (n=237), household (HH) salt (n=219) and drinking water (n=218) were collected from taps in the HH. Urine samples were used to determine UIC, breastmilk was used to determine BMIC, drinking water was used to determine WIC and salt was used to assess household SIC. UIC and iodine content of water was determined by the ammonium persulfate digestion microplate method using the Sandell-Kolthoff reaction.[13] SIC was determined by the iCheck method at the North-West University (NWU) in Potchefstroom.[14] BMIC was analysed at the Laboratory of Human Nutrition of ETH Zurich, Switzerland. Iodine was extracted from the samples using a modified tetramethylammonium hydroxide (TMAH) extraction procedure.[15] The iodine content in filtered TMAH extracts was measured using multicollector-inductively coupled plasma mass spectrometer (MC-ICP-MS) (ThermoFisher Scientific, USA).
Ethics
Participating lactating mothers gave written informed consent for themselves and their infants. The Research and Ethics Committee of the University of Venda approved the study, and an ethics certificate (ref. no. SHS/17/NUT/05/1108) was issued. Permission to conduct the study was also obtained from the Limpopo Provincial Health Department.
Statistical analysis
Data were analysed using SPSS version 26.0 (IBM Corp., USA). Data were checked for normality using Q-Q plots and the Shapiro-Wilk test. Normally distributed data were presented as means with standard deviation (SD). Non-normally distributed data were presented as median values with interquartile ranges (IQRs). Categorical data were expressed as frequencies. The Mann-Whitney (7-test was used to determine differences between groups. Multiple linear regression analyses were used to explore whether household SIC, UIC of mothers, age of infants, and area (Vhembe or Mopani) were predictors of BMIC and UIC of infants (dependent variables), and whether household SIC, age of infants, BMIC, UIC of mothers and area were predictors of UIC of infants (dependent variable) were predictors of BMIC and UIC of infants. Spearman correlations were performed to determine associations between variables. A p-value <0.05 was considered significant. The strength of the correlation was determined by the Spearman correlation coefficient (r). A strong correlation was r >0.70 or r <-0.70, moderate correlation was r >0.30 to 0.70 or r <-0.30 to -0.70 and weak correlation was r = 0.00 to 0.30 or r = 0.00 to -0.30. Associations were deemed to be significant at p<0.05 .
Results
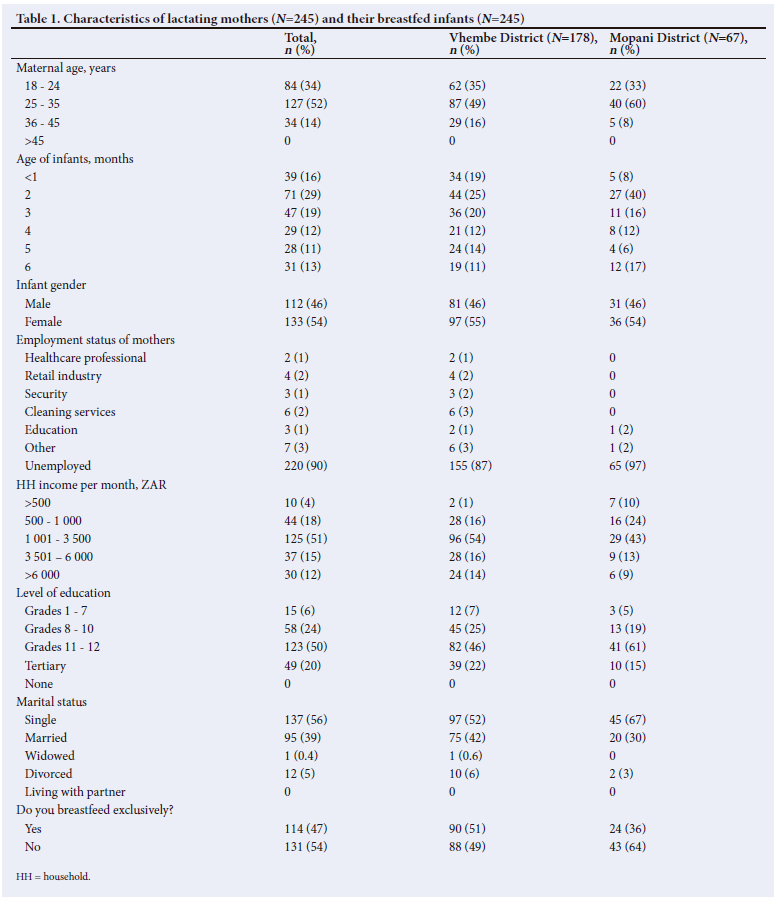
Characteristics of the study participants are shown in Table 1. More than half of the infants were girls. Of all the infants, 54% were not exclusively breastfed and 47% were predominantly breastfed.
Breastmilk iodine content of lactating mothers
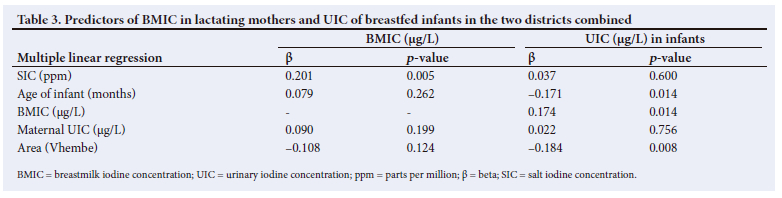
The median (IQR) BMIC of lactating women in Vhembe was 102 (62.0 - 179.7) µg/L and in Mopani it was 150.4 (89.4 - 201.7) µg/L (Table 2). Although the median BMIC was >75 µg/L in both groups, 14% and 8% of mothers in Vhembe and Mopani, respectively, had BMIC levels <75 µg/L, which was indicative of iodine insufficiency. HHSIC was a positive predictor of BMIC (Table 3). There were no further significant differences between the districts or predictors of BMIC.
Urinary iodine content of lactating mothers
The median UIC of mothers was <100 µg/L in Vhembe District and >100 µg/L in Mopani District. More than half of the mothers in Vhembe (52%) and 37% of in Mopani district had UIC <100 µg/L which signifies iodine insufficiency (Table 2). The UIC of mothers was positively correlated with the UIC of infants in Vhembe (r=0.354; p=0.000) and Mopani (r=0.376; p=0.008) districts.
Urinary iodine content of infants
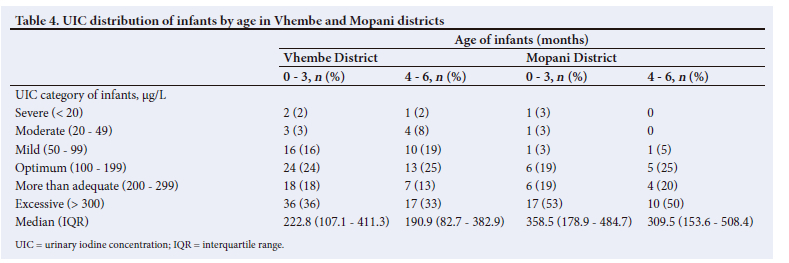
The median UIC of infants fell in the more-than-adequate range in Vhembe and in the excessive range in Mopani (Table 2). The UIC of infants in Mopani was significantly higher than that of infants in Vhembe (p<0.005). Almost a quarter of the infants in Vhembe (24%) and 7.6% in Mopani had a UIC <100 µg/L, while 34% and 52%, respectively, had a UIC in the excessive range. A decrease in UIC was evident as infants grow (Table 4). This was also evident from the negative correlation between infant age and their UIC.
Predictors of UIC in infants were age (negative), BMIC (positive) and the district where they resided (Vhembe - negative) (Table 3).
Household salt iodine content
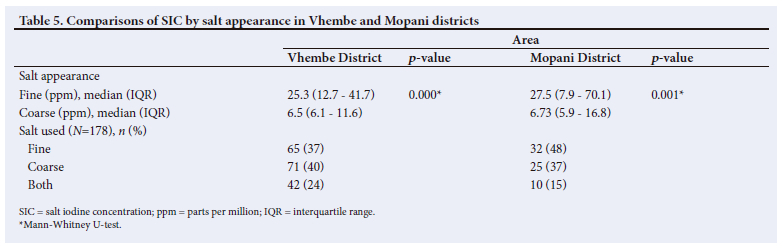
The SIC for all salt samples combined (coarse and fine) was 14.7 ppm in Vhembe District and 16.8 ppm in Mopani District, which was in the inadequate range. Half of the salt samples in HHs in both districts were inadequately iodised. (Table 2). In Vhembe, 37% of the HHs were using fine salt, 40% were using coarse salt and the remaining HHs used both. In Mopani almost half (48%) of the HHs were using fine salt, whereas 37% used coarse salt (Table 5) There was a significant difference between fine and coarse salt iodine content within Vhembe (p<0.05) and Mopani (p<0.05) districts (Table 5).
Water iodine content
The median (IQR) water iodine concentration (WIC) was 12.6 (3.4 - 23.9) µg/L in Vhembe District and 45.8 (14.9 - 72.1) µg/L in Mopani District, which was in the insufficient range. Only 15% of water samples from Vhembe and 47% percent of samples from Mopani fell in the sufficient iodine content range (Table 2).
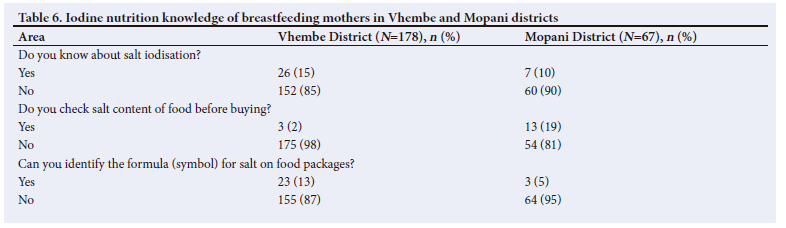
Iodine nutrition knowledge
When participants were asked if they know about salt iodisation, the majority in both districts reported that they had no knowledge of the iodisation process. Most participants in both districts could not identify the symbol for salt on food packages and did not check the salt content of food before buying it (Table 6).
Discussion
The aim of the present study was to determine the iodine status, including breastmilk iodine content, of lactating mothers and their infants aged 0 - 6 months in Vhembe and Mopani districts, Limpopo Province, SA. An exact BMIC cut-off point that reflects a sufficient level has not yet been specified, however, studies[12] have shown that breastmilk with iodine concentrations >75 µg/L may be considered as an index of sufficient iodine intake. Most lactating mothers in the present study had BMIC levels >75 µg/L. The median BMIC in Vhembe (101.4 |ig/L) and Mopani (154 µg/L) was lower than that found in Potchefstroom in the Kenneth Kaunda District.[12] Although BMIC has not been specified at a national level, the findings also suggest that interventions such as salt fortification may be reaching lactating mothers in rural areas, resulting in improved BMIC levels. On the other hand, some participants in Vhembe are still using agricultural coarse salt, which is uniodised in SA, and it may be implicated in their low BMIC levels, i.e. <75µg/L. Mabapa et al.[7] previously reported the use of agricultural coarse salt in Vhembe district.
Based on a BMIC of 101.4||g/L and breastmilk consumption rate of 0.78L/day at 2 - 5 months,[19] infants from Vhembe District consumed 79 µg of iodine daily, whereas infants in Mopani District consumed[19] 120.4 µg iodine per day. The results show that in Vhembe district, infants consumed <90 µg and 110 µg recommended by IOM and WHO, respectively, for infants below 6 months of age;[19] however, infants in Mopani District consumed 120 µg iodine daily which was above the recommended daily intake. The results suggest a variation in BMIC in Vhembe and Mopani districts. Iodine levels also vary based on maternal intake, i.e. BMIC can be increased by increasing maternal iodine intake.[20]
According to Untoro et al.,[21] a median UIC >100 µg/L in lactating mothers is regarded as sufficient. In the present study, the median UIC of lactating mothers in Vhembe District showed iodine deficiency, while the median UIC of mothers in Mopani District was indicative of iodine sufficiency. The UIC of mothers in Vhembe was lower than the 111µg/L reported by Osei et al.[12] in Potchefstroom. Salt fortification may be the reason for iodine sufficiency in Mopani District. UIC is a well-accepted, cost-effective and easily obtainable indicator for iodine status,[5] since most iodine absorbed by the body is excreted in urine.[22]
The UIC of infants in the current study was significantly different (p=0.004) between the two districts. The results suggest that infants consumed more than adequate amounts of iodine in Vhembe and excess amounts iodine in Mopani. The UIC of infants was higher than that of their mothers. This finding may be attributed to the
fact that thyroid and renal functions in infants are not mature and therefore excess iodine cannot be retained. In addition, lactating mothers may lose iodine in breastmilk.[23] Most studies[12] tracking the UICs of mother-infant pairs have reported findings similar to those in the present study. Excessive iodine intake is an emerging problem, and to the best of our knowledge there are no SA studies exploring the consequences of excessive iodine intake. It is evident that the strategies used in SA to eradicate iodine deficiency disorders are effective, since recent studies [8,12] report excessive iodine in infants and schoolchildren. A higher-than-normal iodine intake can affect thyroid gland function, leading to autoimmune disease, goitre, hypothyroidism, iodine-induced thyrotoxicosis or thyroid cancer.[24]
Confirming the decrease of BMIC on the iodine status of breastfed infants,[25] the results show that the UIC of breastfed infants decreased from a higher concentration to a lower concentration in the 0 - 3 months and 4 - 6 months, respectively, although the UIC remained within the adequate range. The results of the regression analysis showed a negative association between the age of infants and their UIC, thereby a decrease in BMIC as the infant grows.
In the present study, HH salt in Vhembe District was inadequately iodised, while HH salt in Mopani was adequately iodised. In Vhembe, 43% of HHs were using adequately iodised salt, compared with almost a third of HHs in Mopani District. These values were lower than the national coverage of 77% and the international goal of 90% coverage.[26]
Mabasa et al.[9] also found that 52.5% of households in Mopani used adequately iodised salt, with an iodine concentration of >15 ppm. It was concerning that almost half of household salt in the present study and the study conducted by Mabasa et al.[9] were inadequately iodised. It is noteworthy to mention that the salt samples with inadequate iodine were coarse in the current study. It can be assumed that salt producers iodising salt at a concentration of more than 20 ppm contributes to the elimination of iodine deficiency.[27] However, a proportion of the salt examined in this study was clearly not iodised in accordance with the legal requirement. A potential reason for not iodising salt in accordance with legal requirements may be that monitoring and evaluation is not done properly at production sites therefore some salt producers may over- or under-iodise.
In the present study, the WIC was 12.6 µg/L and 45.8 µg/L in the Vhembe and Mopani districts, respectively. The possible reason for the discrepancy in WIC levels may be the geographical location. Vhembe District is mountainous whereas Mopani is situated on flat terrain. The WIC in Vhembe was lower than that of 46.2µg/L found by Mabasa et al.[9] in Mopani District, while the WIC in Mopani was almost the same as the WIC levels reported by Mabasa et al. [9] The WIC in the two studies was lower than the 117 µg/L found in the Northern Cape Province by the NFCS.[28] The results of the present study suggest that iodine levels in drinking water is sufficient in Mopani District and insufficient in Vhembe District. Iodine in drinking water may serve as an indication of the amount of iodine occurring naturally in the environment.[7] However, the limited contribution of iodine in water to the total daily iodine intake would usually be considered inadequate for the nutritional requirements of children and pregnant women.[8]Many of the study participants had limited iodine nutrition knowledge. Most of the participants did not know anything about salt iodisation and could not identify the symbol for salt on food packaging. Jooste et al.'291 drew similar conclusions in a study done among the SA adult population and suggested that the education and promotion aspects of the iodised salt intervention are seriously lacking.
Conclusion
Our findings suggest that iodised salt is a major contributor to iodine status in lactating mothers and their infants. The results also show that the salt iodisation programme in SA supplies sufficient iodine for children and women of reproductive age and for lactating mothers and breastfed infants. However, there are areas where agricultural salt is used for human consumption. In addition, some of the salt samples (agricultural coarse salt) have low or no iodine at all. Communities should be taught about the adverse effects of iodine deficiency that may result secondary to the use of uniodised salt. Iodine levels appear to be poorly monitored at production sites - there is an urgent need for ongoing monitoring of salt fortification at production site, to avoid under and over-iodisation of salt.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the SCH's Master of Public Nutrition degree.
Acknowledgements. The authors thank the mothers and infants who participated in the study, the Department of Health, Professor AKA Amey for advanced statistical analysis, ETH (Zurich) for assisting with sample analysis and the field worker, Tshilidzi Ndou.
Author contributions. SCH: the principal investigator and student, study conceptualisation, data collection, developed the manuscript. LFM: guidance with conceptualisation, data collection and in development and finalisation of the manuscript. NSM: data analysis, assistance with development and finalisation, cosupervisor. JB: guidance with conceptualisation, proposal development, statistical training, supplied equipment for data collection, cosupervisor. All authors read and contributed to finalisation of the manuscript.
Funding. The authors wish to thank the University of Venda for financial support.
Conflicts of interest. None.
References
1. Pearce EN, Andersson M, Zimmermann MB. Global iodine nutrition: Where do we stand in 2013? Thyroid 2013;23(5):523-528. https://doi.org/10.1089/thy.2013.0128 [ Links ]
2. Zimmermann MB, Boelaert K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol 2015;3(4):286-295. https://doi.org/10.1016/s2213-8587(14)70225-6 [ Links ]
3. Andersson M, Karumbunathan V, Zimmermann MB. Global iodine status in 2011 and trends over the past decade. J Nutr 2012;142(4):744-750. https://doi.org/10.3945/jn.111.149393 [ Links ]
4. Thaker VV, Leung AM, Braverman LE, Brown RS, Levine B. Iodine-induced hypothyroidism in full-term infants with congenital heart disease: More common than currently appreciated? J Clin Endocrinol Metab 2014;99(10):3521-3526. https://doi.org/10.1210/jc.2014-1956 [ Links ]
5. Jooste P. South Africa: Leading the way with 60 years of salt iodization. IDD Newsletter 2013;41(4):3-4. https://ign.org/app/uploads/2023/04/nl_nov13_email.pdf (accessed 30 June 2023). [ Links ]
6. World Health Organization. Assessment of iodine deficiency disorders and monitoring their elimination: A guide for programme managers. Geneva: WHO, 2007. [ Links ]
7. Mabapa NS, Mbhenyane XG, Mamabolo RL, Amey AKA. Iodine Status of Rural School children in Vhembe District of Limpopo Province, South Africa. Curr Res Nutrition Food Sci J 2014;2(2):98-105. https://doi.org/10.12944/CRNFSJ.2.2.07 [ Links ]
8. Jooste PL, Labadarios D, Nel H. and Strydom E, 2005. Iodine content of household salt, drinking water and iodine status of women and children. National Food Consumption Survey-Fortification Baseline (NFCS-FB): South Africa. Pretoria: National Department of Health, 2007:387-408. [ Links ]
9. Mabasa E, Mabapa NS, Jooste PL, Mbhenyane XG. Iodine status of pregnant women and children age 6 to 12 years feeding from the same food basket in Mopani district, Limpopo province, South Africa. S Afr J Clin Nutrition 2018;32(3):76-82. [ Links ]
10. Charlton KE, Jooste PL, Steyn K, Levitt NS, Ghosh A. A lowered salt intake does not compromise iodine status in Cape Town, South Africa, where salt iodization is mandatory. Nutrition 2012;29(4):630-634. https://doi.org/10.1016/j.nut.2012.09.010 [ Links ]
11. Tazebay UH, Wapnir IL, Levy O, et al. The mammary gland iodide transporter is expressed during lactation and in breast cancer. Nat Med 2000;6(8):871-878. https://doi.org/10.1038/78630 [ Links ]
12. Osei J, Andersson M, van der Reijden O, Dold S, Smuts CM, Baumgartner J. Breast-milk iodine concentrations, iodine status, and thyroid function of breastfed infants aged 2 - 4 months and their mothers residing in a South African township. J Clin Res Pediatr Endocrinol 2016;8(4):381-391. https://doi.org/10.4274/jcrpe.2720 [ Links ]
13. Ohashi T, Yamaki M, Pandav CS, Karmarkar MG, Irie M. Simple microplate method for determination of urinary iodine. Clinical Chem 2000;46(4):529-536. [ Links ]
14. Rohner F, Garrett GS, Laillou A, et al. Validation of a user-friendly and rapid method for quantifying iodine content of salt. Food Nutrition Bull 2015;33(4 Suppl 3):S330-S335. [ Links ]
15. Andrey D, Zbinden P, Wah MK, Lee W. A routine quality control method for the determination of iodine in human and pet food by ICP-MS. Atomic Spectroscopy 2001;22(3):299-305. [ Links ]
16. Henjum S, Kjellevold M, Ulak M, et al. Iodine concentration in breastmilk and urine among lactating women of Bhaktapur, Nepal. Nutrients 2016;8(5):255. https://doi.org/10.3390%2Fnu8050255 [ Links ]
17. Kartono D, Atmarita A, Jahari AB, Soekirman S, Izwardy D. The situation of urinary iodine concentration (UIC) among school age children, women at reproductive age and pregnant women in Indonesia: The analysis of Riskesdas 2013. Gizi Indonesia 2017;39(1):49-58. [ Links ]
18. Liu P, Su X, Shen H, et al. National iodine deficiency disorders: An analysis of surveillance data in 2011. Chinese J Endemiol 2015(12):181-185. [ Links ]
19. Institute of Medicine. Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, molybdenum, nickel, silicon, vanadium and zinc. Washington: National Academy Press, 2001. [ Links ]
20. Zimmermann MB. The adverse effects of mild-to-moderate iodine deficiency during pregnancy and childhood: A review. Thyroid 2007;17(9):829-835. https://doi.org/10.1089/thy.2007.0108 [ Links ]
21. Untoro J, Mangasaryan N, de Benoist B. and Darnton-Hill, I, 2007. Reaching optimal iodine nutrition in pregnant and lactating women and young children: Programmatic recommendations. Public Health Nutr 10(12A):1527-1529. https://doi.org/10.1017/s1368980007705360 [ Links ]
22. Gibson RS. Principles of Nutritional Assessment. Oxford: Oxford University Press, 2005. [ Links ]
23. Fuse Y, Ohashi T, Yamaguchi S, Yamaguchi M, Shishiba Y, Irie M. Iodine status of pregnant and postpartum Japanese women: Effect of iodine intake on maternal and neonatal thyroid function in an iodine-sufficient area. J Clin Endocriol Metab 2011;96(12):3846-3854. https://doi.org/10.1210/jc.2011-2180 [ Links ]
24. Biban BG, Lichiardopol C. Iodine deficiency, still a global problem? Curr Health Sci J 2017;43(2):103-111. https://doi.org/10.12865/chsj.43.02.01 [ Links ]
25. Mulrine HM, Skeaff SA, Ferguson EL, Gray AR, Valeix P. Breast-milk iodine concentration declines over the first 6 mo postpartum in iodine-deficient women. Am J Clin Nutrition 2010;92(4):849-856. https://doi.org/10.3945/ajcn.2010.29630 [ Links ]
26. World Health Organization. Indicators for assessing iodine deficiency disorders and their control through salt iodization. Geneva: WHO, 1994. http://whqlibdoc.who.int/hq/1994/WHO_NUT_94.4.pdf (accessed 19 February 2003). [ Links ]
27. World Health Organization. Assessment of iodine deficiency disorders and monitoring their elimination: A guide for programme managers. Geneva: WHO, 2001. [ Links ]
28. Labadarios D, Steyn NP, Maunder E, et al. The National Food Consumption Survey (NFCS): South Africa, 1999. Public Health Nutr 2005;8(5):533-543. https://doi.org/10.1079/phn2005816 [ Links ]
29. Jooste PL, Upson N, Charlton KE. Knowledge of iodine nutrition in the South African adult population. Public Health Nutrition 2005;8(4):382-386. https://doi.org/10.1079/phn2004696 [ Links ]
 Correspondence:
Correspondence:
N S Mabapa
solomon.mabapa@univen.ac.za
Accepted 17 May 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}