










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.17 no.3 Pretoria Set. 2023
http://dx.doi.org/10.7196/sajch.2023.v17i3.2022
RESEARCH
Cultural and linguistic applicability of the English PEDS tools in a low-income community: A caregiver perspective
M BotesI; D W SwanepoelI; M GrahamII; J van der LindeI
IPhD; Department of Speech-Language Pathology, University of Pretoria, South Africa
IIPhD; Department of Science, Mathematics and Technology Education, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Regular developmental surveillance using structured developmental screening tools is a proven way to effectively identify developmental delays and disabilities. Most screening tools are developed and standardised in high-income countries and then adapted and translated for low- and middle-income countries. However, cultural differences and viewpoints make it challenging to translate and adapt developmental screening tools for low-income communities
OBJECTIVES: To determine caregivers' perspectives on linguistic and cultural appropriateness of the Parents' Evaluation of Developmental Status (PEDS) and the PEDS: Developmental Milestones (DM) as a first step in the adaptation process for low-income communities in South Africa
METHOD: Participants (N=102) were selected using convenience sampling at an immunisation clinic. We employed a survey research design. Quantitative data were analysed using descriptive statistics and qualitative survey feedback survey was analysed using data-driven inductive methodology
RESULTS: On the PEDS questionnaire, 38.2% of participants indicated the term 'development' on question 1 was not suitable; and 51% preferred the phrase 'sometimes worry' more than the phrase 'have any concerns' for questions 2 - 9. On the PEDS:DM, 58 of the 124 questions were deemed difficult. Most questions were problematic owing to cultural or linguistic differences (49 questions), while 9 questions were too difficult for the child's age. The expressive language developmental domain had the most challenges
CONCLUSION: The present study relied on robust community participation, enabling community-led adaptation of the PEDS tools. Items on the tools were viewed solely from a community perspective, empowering the community to be 'experts' in this process, ensuring greater contextual relevance and applicability of the tools, as well as generalisability to similar low-income communities
Early identification of developmental delays or disabilities in children through developmental surveillance is often the entry point for early intervention services.[1] With early intervention, the impact of developmental delays and disabilities on children and families can be reduced.[2] Developmental surveillance also allows healthcare workers to continuously monitor a child's developmental and behavioural status.[1] Regular developmental surveillance during health visits, using structured developmental screening tools, is a successful way to identify developmental delays and disabilities in a timely manner.[3] Developmental surveillance is crucial in low- and middle-income countries (LMICs), where children are at increased risk of developmental delays with lifelong consequences.[1] The adverse effects of developmental delays and disabilities for children include failure at school, an increased risk of leaving school without graduating, as well as a higher risk of not attending school.[4] These children are prone to being unemployed, having low income-generating potential, high fertility statistics and being unable to provide adequate care for their children, which perpetuates the poverty cycle.[5] It is estimated that more than 350 million children in LMICs are at risk for developmental delays and disabilities, with the majority residing in South Asia and sub-Saharan Africa.[6] In 2018, Slemming and Bamford[7] estimated that up to 35% of children in South Africa (SA) under the age of 5 may suffer from developmental delays or disabilities.
Despite the need for early childhood development services, standardised and validated developmental screening tools are not readily available for children in LMICs.[8] Screening tools are typically developed, standardised and validated in high-income countries and then adapted and translated for low-income settings.[8] Modifying an existing tool for use in a new population is usually preferred, as it is more achievable and cost-effective.[9] Some popular developmental screening tools adapted and translated for use internationally include the Denver Developmental Screening Test, the Ages and Stages Questionnaire (ASQ) and the Parents' Evaluation of Developmental Status (PEDS).[10]
For most developmental screening tools (or diagnostic developmental tools), the adaptation process of a tool is part of the translation process and is done by experts in the field of development.[10] For instance, in the process of translating and adapting the Mullen Scales of Early Learning (a measure of cognitive functioning for infants and preschool-age children from birth through age 5.8 years (68 months)) and the Ages and Stages Questionnaire (ASQ) for the SA Afrikaans-speaking population, a review committee adapted the questions to make it culturally appropriate, e.g. the metric system of measurement was employed instead of the imperial system, and the word 'applesauce' was changed to 'jam'.[11] The translated and adapted tools were then evaluated by community members, specifically teachers, to determine cultural appropriateness.[11] In translating the ASQ for Hindi and isiZulu-speaking populations in SA, no cultural adaptations were mentioned for the Hindi translation but some content was changed by an expert panel to improve contextual relevance of the test items (e.g. last name changed to surname) for the isiZulu translation.[12,13] However, when the PEDS was translated into isiZulu and northern Sotho, no cultural adaptations were made.[14,15] Utilising translated developmental tools still ingrained with Western concepts may be laden with difficulties in African, low-income settings,[16] as African cultures, traditions and languages are very different from those in Western contexts.[11]
It is challenging to translate and adapt developmental screening tools as cultural differences influence parenting and child development.[9] Cultural views differ on when a child should learn specific skills, how they interact with other people and what is considered appropriate behaviour.[9,17] Cultural viewpoints on parenting will also influence the way people understand and answer questions about development.[18] Thus, cultural adaptation of a tool is critical to ensure the accuracy of the screening tools for a specific population. Often, cultural considerations do not receive the necessary attention during the translation and adaptation process of developmental screening tools. El-Behadli et al.[10] reported that cultural considerations were only taken into account in 44% (n/N=28/63) of identified developmental screening tools. A further concern is that the details of the methods employed to culturally adapt screening tools are rarely reported.[19] A comprehensive cultural adaptation process is required to appropriately modify an instrument for use in a new population,[18,20] because data collected for the developmental screening process are entirely dependent on the items' wording and how the questions are interpreted[9]
Limited research has been done on the community perspective of linguistic and cultural appropriateness of developmental screening tools, especially within a framework where caregivers and their broader community are seen as experts and their input is used as a first step in the adaptation and translation of a tool, as opposed to one of the last steps. DAprano et al.[21] followed a 5-step adaptation and translation process of the ASQ for indigenous Australians, where the community input was one of the first steps. This resulted in a tool that was accepted by the community to be culturally and linguistically appropriate.[21] Staff and caregivers expressed high levels of satisfaction.[22]
There is a widespread need for linguistically and culturally appropriate developmental screening tools in countries like SA that are proven to be appropriate across linguistic and cultural backgrounds. This implies that tools that are available in English should be adapted specifically for the SA population. The present study aimed to determine caregiver perspectives on linguistic and cultural appropriateness of the PEDS tools, and the applicability of the tools in a low-income community, as a first step in its contextual adaptation for SA.
Ethics
The survey study was approved by the Institutional Review Board (IRB) at the University of Pretoria before any data were collected (ref. no. HUM027/0819).
Methods
Setting
The present study was conducted at an immunisation clinic in a low-income and peri-urban community in Gauteng Province, SA. Mamelodi has a population of ~334 557 characterised by high levels of unemployment (24%), low levels of education (39% completed high school) and growing informal settlements (growth rate of 3%).[23] The community health clinic, where data were collected, offers a complete set of primary health services set of services, including a baby wellness clinic.
Participants
Participants were selected using convenience sampling. Parents or caregivers waiting in line at the baby wellness clinic, who could communicate in English and had a minimum education level of Grade 10, were invited to participate. The participants also had to be caregivers of an infant or child between age 0 and 8 years. All participants (N=102) were mothers (of the infants or children in question), with a mean (range) age of 30.4 (17 - 43) years. The mean (range) age of the children was 43.3 months (6 weeks - 7y11m). Sepedi was the most spoken first language among participants (n=49; 48.0%). More than two-thirds of the participants completed grade 12 (69%) and 24 (24%) had obtained a diploma or degree. However, 60 (59%) participants were unemployed and 89 (83%) were not married and not living with a partner.
Materials
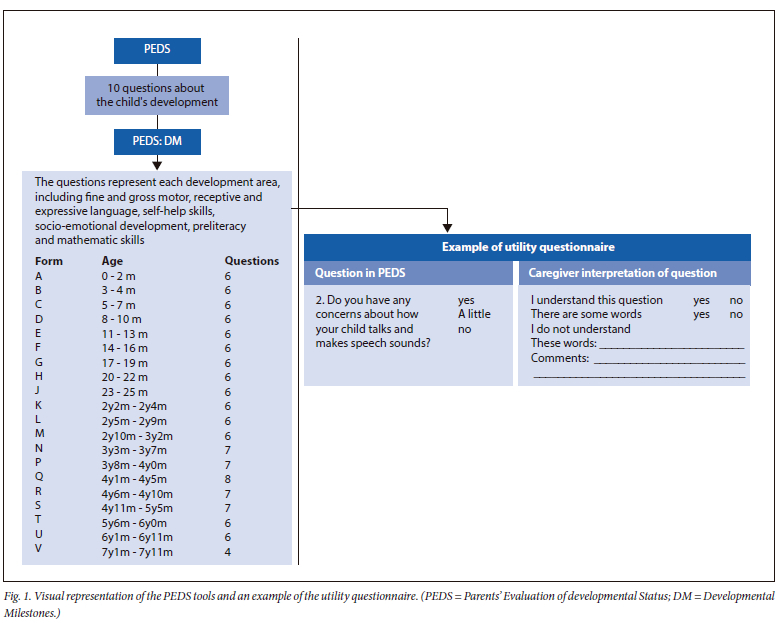
The PEDS tools, an English developmental screening tool, consist of the PEDS and the PEDS:DM. This developmental screening tool was designed to be parent-administered or administered by an interview - the PEDS consists of 10 questions about the general development of the followed infant or child (depending on the results of the PEDS) by the PEDS: Developmental Milestones (PEDS:DM). The PEDS:DM for ages 0 - 7 years 11 months consists of six to eight questions per age group about the child's development. The questions represent each developmental area, including fine and gross motor, receptive and expressive language, self-help skills, socio-emotional development, preliteracy and mathematics skills. The questions differ depending on the child's age and are subdivided into forms A to V corresponding to the child's age, with 124 questions in total (Fig. 1). The PEDS tools start with the PEDS, where pathway A signifies a fail, regardless of the PEDS:DM. In pathway B to E, the PEDS: DM results determined the pass or fail.[24] The benefits of the PEDS tools specifically for a low-income community are that it takes less than 5 minutes to complete and costs ~ZAR0.40.[25] The PEDS has also been adapted and translated into more than 20 languages and is used worldwide.
Data collection
After consent was obtained from each participant, they were asked to complete a background information questionnaire, the PEDS and PEDS:DM for their child. Participants also completed a self-developed utility questionnaire, asking caregivers about the ease of understanding the questions and the appropriateness of the items on the PEDS tools. Two closed-form type and a 'comments' section were included for each item on the PEDS tools (Fig. 1). Participants had to complete the utility questionnaire of the PEDS:DM on 4 to 5 forms close to their child's age. Each participant had to answer an average of 39 questions, including the 10 questions of the PEDS and an average of 29 questions on the PEDS:DM. For forms A - E, 18 participants completed the questionnaire, forms F - J 17 participants, forms K - P 17 participants and forms Q - V 50 participants, for a total of 102 participants (Supplementary Table 1; https://www.samedical.org/file/2098). PEDS:DM
Participants had problems with 58 of the 124 (47%) questions in the PEDS:DM.
Of the 124 questions in the PEDS:DM participants indicated that 31 questions (25%) were difficult to understand by marking the option 'I do not understand the question' on the questionnaire. Question 6 on form D was the most difficult ('Does your baby like to play peek-a-boo?'), with 89% of participants indicating that they had trouble understanding the question. More than three-quarters (76.5%) of the participants indicated that question 1 on form M ('Can your child scribble with a crayon or marker without going off the page much?') was difficult and 72% indicated that question 5 on form A ('Does your baby try to keep his or her head steady?') was problematic (Supplementary table: https://www.samedical.org/file/2098).
Participants indicated that 41 ofthe questions (33%) used unfamiliar words by choosing the option 'I do not understand the word' on the questionnaire and indicating which words were unfamiliar. None of the participants could interpret 'pacifier' (form A, question 2), 'scooting on his bottom' (form D, question 5), 'Busy Boxes and squeaking toys' (form E, question 6); and 'scribble' (forms H and J, question 1) (Supplementary tables: https://www.samedical.org/file/2098).
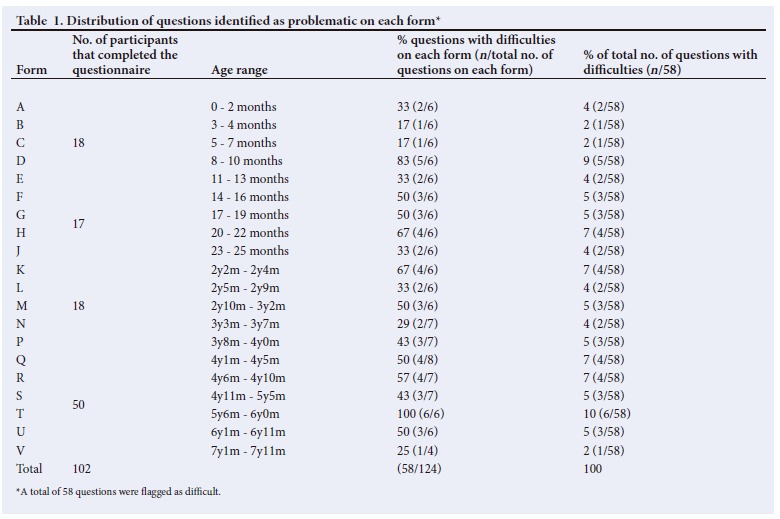
Participants felt that 9 of the questions (7%) were problematic because they were too difficult for the child's age (Supplementary table: https://www.samedical.org/file/2098), as mentioned by the participants in the comment section of the questionnaire. A little more than a third (35.0%) of the participants felt that question 1 on form R ('Can your child write any letters of the alphabet?') was too difficult for the age group 4y6m - 4y10m, and 27.0% indicated that questions 4 and 8 on form Q for age group 4y1m - 4y5m were also too difficult ('Does your child use words that tell about time like morning, afternoon, night, yesterday, or tomorrow?'; 'Point to the letters and ask, "Where's the A?... Where's the X... Where's the O?" Keep trying to see if he or she can point to two or three correctly. How did your child do?'). Table 1 summarises the number of questions on each form identified as difficult and the percentage of difficulty from the total number of questions with difficulty (n=58). Form T for ages 5y6m - 6y0m had the most questions with difficulties: all questions on the form were problematic; however, < 10% of participants had difficulty with 5 of the 6 questions. This represents 10% of the total number (n=58) of questions with difficulty in the PEDS: DM. On form D for ages 8 - 10 months, 5 out of the 6 questions (83%) were identified as problematic.
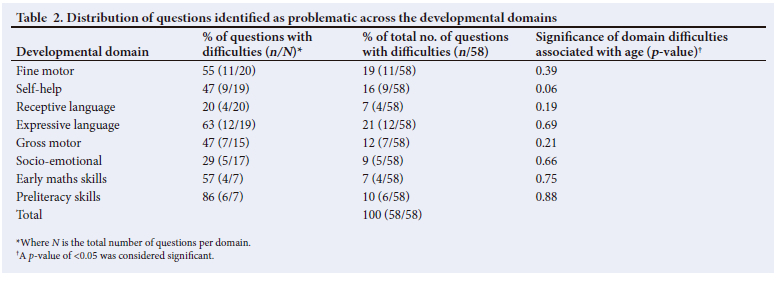
Table 2 illustrates the distribution of questions identified as problematic across the developmental domains. The expressive language developmental domain had the most challenges, with 12 out of a possible 19 questions flagged as difficult (63%), representing 21% of the total number (n=58) of questions with difficulty in the PEDS:DM. Receptive language had the least difficulty, with 4 out of a possible 20 questions being problematic (20%), representing 7% of the total number of questions with difficulty. No statistically significant differences were found for domain difficulties associated with age.
Discussion
The present study sought to obtain a systematic and thorough understanding of caregivers' perspectives on the cultural and linguistic appropriateness, as well as the applicability of the PEDS tools in a low-income community. This is a necessary step towards the adaptation of the PEDS tools for low-income communities in SA, as many items (10/10 items of the PEDS and 58/124 items on the PEDS: DM) were identified as needing cultural or linguistic adaptation for the population. The next step is to adapt the items identified by the community to create a version of the PEDS tools suitable for a low-income community.[26] Supplementary Fig. 1 (https://www.samedical.org/file/2097) outlines the steps for the cultural adaption of the PEDS tools and highlights the importance of the caregiver perspectives on the cultural and linguistic appropriateness of the tools. The guidelines for the translation of instruments as set out by the WHO[27] and the International Test Committee (ITC)[28] was used as a framework for these steps. In the present study, caregivers specified that they preferred to change the term 'concern' to a more understandable term 'worry about' on all of the questions on the PEDS. In the development of the PEDS, families did not respond appropriately to the word 'worry' or 'problem' because 'worries' might have been too strong-worded.[29] However, in Singapore, the PEDS was translated into Mandarin and Malay to screen children for developmental delays in a Southeast Asian context.[30] The results indicated that parents' understanding of the concept of 'concern' was different across languages and cultures.[30] A subsequent study[31] also translated the PEDS into Mandarin and noted that the word 'concern' directly translated in Mandarin meant 'do you care about' (i.e. do you care about your child?), which may offer an explanation for the results of the first study. However, rather than directly translating the text, the authors replaced the word with a word meaning 'a little worried'. The adapted version of the Mandarin PEDS indicated an incidence of developmental delay similar to the prevalence of delays in the rest of the country.[31] Participants in the present study also indicated that the word 'development' was problematic. This correlates with the findings in the development of the PEDS, where only ~50% of families understood the word 'development'.[29]
On the PEDS:DM, caregivers from the community perceived 58 of the 124 (47%) questions to have cultural or linguistic problems. A systematic adaptation process is lacking in the adaptation of developmental screening tools, as most studies only report on the type of adaptations made and not on the number of items that required adaptation.[19] Our study is one of a limited number of studies to describe the problematic items individually from a community perspective, as cultural or linguistic problems are typically identified and modified by an expert panel. In South West Ethiopia, 29% of the test items on the Denver II Developmental Screening Test were identified for adaptation by an expert panel.[32] In Sri Lanka, only 5 items on the Denver II were adapted by an expert panel.[32] In SA, the review committee only changed items with specific measuring systems, currency, climate-related questions or food-specific questions when adapting the ASQ and Mullen Scales of Early Learning.[11] In Australia, when adapting the ASQ for the indigenous community, specific coastal items were replaced with more general items that would be found in remote communities.[33] However, none of the studies reported the number of problematic items. While there are studies on the translation of the PEDS, there are no reports on the adaptation of the PEDS:DM for a target community. The PEDS has been translated into over 23 languages, but less than half the number was published.[10] In 2015, El-Behadli et al.[10] reported that cultural considerations were only taken into account in the Swahili translation of the PEDS. When adapting a developmental screening tool, a more meticulous approach that includes the cultural adaptations of items should be employed and reported on in future studies.
Most adaptations on developmental screening tools are in the socio-emotional domain, with the least adaptation in the gross motor domain.[8] Socio-emotional skills seem to be more prone to socio-cultural influences than gross motor skills.[32] However, on the PEDS: DM, the expressive language developmental domain was the most problematic, as the community found 63.2% of the questions in this domain to be culturally or linguistically inappropriate. In contrast, the socio-emotional domain was one of the domains that caregivers identified as needing the least adaptation. Concepts or wording of the items in the expressive language domain might not be familiar to the millions of people that use English in SA as lingua franca, a second or third language; and more common form of spoken English should be considered in the next steps in adapting the PEDS tools for SA.
The present study exemplifies robust community participation that enabled the community to lead the adaptation process. This process ensured that items on the tools were viewed solely from a community perspective, empowering the community to be 'experts' in the process. Future studies can compare the community's views on problematic items on developmental screening tools with the views of experts in the field.
Study strengths and limitations
A strength of the present study is that it is one of the first to undertake the testing of critical concepts and vocabulary within a community setting to ensure that interpretation, local culture and background be considered for the appropriate adaptation of the PEDS tools for the population. This research also sheds light on the cultural adaptation process that could encourage similar research endeavours to increase the rigour in adaptation methods of screening tools. A limitation of the current study was that it was carried out in a single setting, which limits its generalisability. We recommend duplication of the study in other low-income communities in SA and, further, that the next step be followed to culturally adapt the PEDS tools for low-income communities in SA (Supplementary Fig. 1; https://www.samedical.org/file/2097).
Conclusion
For optimal child development to happen, culturally appropriate early identification and intervention processes must be in place. In low-income communities, cross-cultural adaptation of existing developmental screening tools is critical. Caregiver perspectives in the adaptation of a screening tool can confirm a screening tool's linguistic and cultural appropriateness, ensuring acceptance of the tool by the target community to identify possible developmental delays and disabilities more efficiently. This adaptation method also highlights the gaps in research in making a developmental screening tool culturally appropriate. This method can guide future research on the necessary inclusion of community perspectives as a starting point to ensure culturally appropriate adaptations. Although the process can be intensive and time-consuming, the community perspectives on the cultural and linguistic appropriateness of developmental screening tools from high-income countries are important, to ensure that the tool is valid and relevant for low-income communities.
Declaration. None.
Acknowledgements. None.
Author contributions. Equal contributions.
Funding. None.
Conflicts of interest. None.
References
1. Rydz D, Shevell MI, Majnemer A, Oskoui M. Topical Review: Developmental Screening. J Child Neurol 2005;20(1):4-21. https://doi.org/10.1177/08830738050200010201 [ Links ]
2. Guralnick MJ. Early intervention for children with intellectual disabilities: An update. J Appl Res Intellect Disabil 2017;30(2):211-229. https://doi.org/10.1111/jar.12233 [ Links ]
3. Guevara JP, Gerdes M, Localio R, et al. Effectiveness of developmental screening in an urban setting. Pediatrics 2013;131(1):30-37. https://doi.org/10.1542/peds.2012-0765 [ Links ]
4. Engle PL, Black MM. The effect of poverty on child development and educational outcomes. Ann NY Acad Sci 2008;1136(1):243-256. https://doi.org/10.1196/annals.1425.023 [ Links ]
5. Grantham-McGregor S, Cheung YB, Cueto S, et al. Developmental potential in the first 5 years for children in developing countries. Lancet 2007;369(9555):60-70. https://doi.org/10.1016/S0140-6736(07)60032-4 [ Links ]
6. Olusanya BO, Davis AC, Wertlieb D, et al. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990 - 2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018;6(10):e1100-1121. https://doi.org/10.1016/S2214-109X(18)30309-7 [ Links ]
7. Slemming W, Bamford L. The new Road-to-Health Booklet demands a paradigm shift. S Afr J Chid Health 2018;12(3):86-87. https://doi.org/10.7196/SAJCH.2018.v12i3.1595 [ Links ]
8. Gladstone MJ, Lancaster GA, Jones AP, et al. Can Western developmental screening tools be modified for use in a rural Malawian setting? Arch Dis Child 2008;93(1):23-29. https://doi.org/10.1136/adc.2006.095471 [ Links ]
9. DuBay M, Watson LR. Translation and cultural adaptation of parent-report developmental assessments: Improving rigor in methodology. Res Autism Spectr Disord 2019;62:55-65. https://doi.org/10.1016/J.RASD.2019.02.005 [ Links ]
10. El-Behadli AF, Neger EN, Perrin EC, Sheldrick RC. Translations of developmental screening instruments: An evidence map of available research. J Dev Behav Pediatr 2015;36(6):471-483. https://doi.org/10.1097/DBP.0000000000000193 [ Links ]
11. Bornman J, Sevcik RA, Romski M, Pae HK. Successfully translating language and culture when adapting assessment measures: Translating assessment measures. J J Policy Pract 2010;7(2):111-118. https://doi.org/10.1111/j.1741-1130.2010.00254.x [ Links ]
12. Abdoola S. Translating tools for better parent-based assessment: An exploratory study. J Commun Disord 2015;62(1):1-12. https://doi.org/10.4102/sajcd.v62i1.73 [ Links ]
13. Hsiao C, Richter L, Makusha T, Matafwali B, van Heerden A, Mabaso M. Use of the ages and stages questionnaire adapted for South Africa and Zambia: Ages and stages questionnaire in southern Africa. Child Care Health Dev 2017;43(1):59-66. https://doi.org/10.1111/cch.12413 [ Links ]
14. Van der Merwe M, Cilliers M, Maré C, van der Linde J, le Roux M. Evaluation of a Zulu translation of the Parents' Evaluation of Developmental Status. Afr J Prim Health Care Fam 2017;9(1):a1365. https://doi.org/10.4102/phcfm.v9i1.1365 [ Links ]
15. Fyvie L, Anderson J, Kruger CJ, le Roux M , van der Linde J. The outcome of a developmental screening tool (PEDS) in English and Northern Sotho: A comparative study. Lang Matters 2016;47(3):415-426. https://doi.org/10.1080/10228195.2016.1196718 [ Links ]
16. Geiger M, Alant E. Child-rearing practices and children's communicative interactions in a village in Botswana. Early Years 2005;25(2):183-91. https://doi.org/10.1080/09575140500128079 [ Links ]
17. Van Widenfelt BM, Treffers PDA, de Beurs E, Siebelink BM, Koudijs E. Translation and cross-cultural adaptation of assessment instruments used in psychological research with children and families. Clin Child Fam Psychol Rev 2005;8(2):135-147. https://doi.org/10.1007/s10567-005-4752-1 [ Links ]
18. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000;25(24):3186-3191. https://doi.org/10.1097/00007632-200012150-00014 [ Links ]
19. Soto S, Linas K, Jacobstein D, Biel M, Migdal T, Anthony BJ. A review of cultural adaptations of screening tools for autism spectrum disorders. Autism 2015;19(6):646-661. https://doi.org/10.1177/1362361314541012 [ Links ]
20. Acquadro C, Conway K, Hareendran A, Aaronson N. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Health 2008;11(3):509-521. https://doi.org/10.1111/j.1524-4733.2007.00292.x [ Links ]
21. D'Aprano A, Silburn S, Johnston V, et al. Challenges in monitoring the development of young children in remote Aboriginal health services: Clinical audit findings and recommendations for improving practice. Rural Remote Health 2016;16(3):1-6. https://doi.org/10.22605/RRH3852 [ Links ]
22. Statistics South Africa. Census 2011: Census in brief. Pretoria: StatsSA, 2012. http://www.statssa.gov.za/census/census_2011/census_products/Census_2011_Census_in_brief.pdf (accessed 30 May 2022). [ Links ]
23. Simpson S, D'Aprano A, Tayler C, Toon Khoo S, Highfold R. Validation of a culturally adapted developmental screening tool for Australian Aboriginal children: Early findings and next steps. Early Human Dev 2016;103:91-95. https://doi.org/10.1016/j.earlhumdev.2016.08.005 [ Links ]
24. Van der Linde J, Swanepoel DW, Glascoe FP, Louw EM, Hugo JFM, Vinck B. Risks associated with communication delays in infants from underserved South African communities. Afr J Prim Health Care Fam Med 2015;7(1):a841. https://doi.org/10.4102/phcfm.v7i1.841 [ Links ]
25. Brothers KB, Glascoe FP, Robertshaw NS. PEDS: Developmental milestones: An accurate brief tool for surveillance and screening. Clin Pediatr 2008;47(3):271-279. https://doi.org/10.1177/0009922807309419 [ Links ]
26. Botes M, Van der Linde J, Swanepoel D. A multi-phase cultural and contextual adaptation of the Parents' Evaluation of Developmental Status tools for a low-income community: A South African case study. Child Care Health Dev 2022;49(4):716-724. https://doi.org/10.111/cch.13083 [ Links ]
27. World Health Organization. Process of translation and adaptation of instruments. Geneva: WHO, 2016. http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed 5 Feb 2022). [ Links ]
28. International Test Commission. ITC guidelines for translating and adapting tests (Second edition). Surrey: ITC, 2017. https://www.intestcom.org/files/guideline_test_adaptation_2ed.pdf (accessed 5 March 2022). [ Links ]
29. Glascoe FP. Collaborating with parents: Using Parents' Evaluation of Developmental Status to detect and address developmental and behavioral problems. Nolensville: Ellsworth & Vandermeer Press, 2013. [ Links ]
30. Kiing JSH, Low PS, Chan YH, Neihart M. Interpreting parents' concerns about their children's development with the Parents Evaluation of Developmental Status: Culture matters. J Dev Behav Pediatr 2012;33(2):179-183. https://doi.org/10.1097/DBP.0b013e31823f686e [ Links ]
31. Toh TH, Lim BC, Bujang MAB, Haniff J, Wong SC, Abdullah MR. Mandarin parents' evaluation of developmental status in the detection of delays. Pediatr Int 2017;59(8):861-868. https://doi.org/10.1111/ped.13325 [ Links ]
32. Abessa TG, Worku BN, Kibebew MW, et al. Adaptation and standardization of a Western tool for assessing child development in non-Western low-income context. BMC Public Health 2016;2016(16):652. https://doi.org/10.1186/s12889-016-3288-2 [ Links ]
33. DApranoA, Silburn S, Johnston V, Robinson G,OberklaidF,Squires J. Adaptation of the Ages and Stages Questionnaire for remote Aboriginal Australia. Qual Health Res 2016;26(5):613-625. https://doi.org/10.1177/1049732314562891 [ Links ]
 Correspondence:
Correspondence:
J van der Linde
jeannie.vanderlinde@up.ac.za
Accepted 9 January 2023


{kind=link}
{kind=link}
{kind=link}