










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.3 Pretoria Sep. 2023
http://dx.doi.org/10.7196/sajch.2023.v17i3.2002
RESEARCH
Losses of children's cognitive potential over time: A South African example
M J Rotheram-BorusI; J ChristodoulouII; E Rotheram-FullerIII; M TomlinsonIV, V
IPhD; Department of Psychiatry and Biobehavioral Sciences, Semel Institute, University of California, Los Angeles, California, USA
IIPhD; Department of Psychology, Palo Alto University, Palo Alto, California, USA
IIIPhD; Division of Educational Leadership and Innovation, Arizona State University, Tempe, Arizona
IVPhD; Institute for Life Course Health Research, Department of Global Health, Stellenbosch University, Cape Town, South Africa
VPhD; School of Nursing and Midwifery, Queens University, Belfast, UK
ABSTRACT
About 250 million children under the age of 5 years in low- and middle-income countries (LMICs) lose lifelong cognitive potential. However, the primary focus of interventions has been to increase survival and promote growth. All pregnant women in 24 non-contiguous, low-income areas in Cape Town, South Africa (N=1 238) were recruited between 2009 and 2010 and reassessed six times over 8 years post birth. Mothers in half of the 24 areas were randomised to receive home visits by community health workers, concentrated during the pregnancy and the first 6 months of life. At 18 months, the children's cognitive development was at the global norm, i.e a mean standard deviation (SD) value of 100 (15). By 5 years of age, the mean cognitive development fell to one SD below the global norm (<85; mean = 83) and 60% of children had scores below the global mean. By 8 years of age, cognitive development scores significantly fell again (mean = 73; 88% of children <85). The magnitude of the loss was substantial and warrants sustained interventions throughout childhood that support children's cognitive development in LMICs. The first 1 000 days of life are important, but insufficient to inoculate children against the negative consequences of poverty and coping with multiple, chronic community challenges (e.g. HIV, alcohol abuse, interpersonal violence).
Annually, approximately 250 million children under the age of 5 years in low- and middle-income countries (LMICs) lose life-long growth and cognitive potential.[1] To date, the primary focus of interventions has been to increase survival and promote growth.[2] These interventions have also been focused on the first 1 000 days of life;[3,4] however, lifelong productivity and engagement require far more to optimise development. The present study documents the apparent loss of cognitive potential over the first 8 years of life in South African (SA) children living in peri-urban, low-income areas.
The influence of poverty and adversity on child outcomes has been repeatedly documented in high-income countries.[1] These impacts are exacerbated by a lack of access to preschool and poor-quality primary school education. While survival, food insecurity and access to education have been emphasised in the World Health Organization's Sustainable Development Goals,[2] the gradual loss of cognitive potential over time has received less attention despite the fact that it will have long-term consequences for the individual, their family, and country. The present study documents this loss of cognitive potential over the first 8 years of life in SA children.
Ethics
The Institutional Review Boards of University of California Los Angeles (UCLA) and Stellenbosch University approved the study whose methods have previously been published.[5]
Methods
Participants
Twenty-four, non-contiguous geographical areas of ~450 to 600 low-income households were identified in the areas surrounding Cape Town, SA. Residents were black and the majority had immigrated from the Eastern Cape Province of SA at similar times. Each area was within 1 km of a healthcare clinic; with 4 to 5 alcohol bars within a 1 km radius (shebeens); with similar types of housing, access to electricity, water, and toilets. The Stellenbosch team trained recruiters (local women from adjoining geographical areas) to conduct house-to-house visits in each area from May 2009 to September 2010 to invite all pregnant mothers aged 18 years or older to participate; only 2% of women (n=25/1 262) refused participation [for details, see 5]. Neighbourhoods were matched into 12 pairs and one neighborhood in each pair was randomly assigned to receive a home-visiting intervention (n=644 mothers and children). Paired neighborhoods received standard care (SC) (n=594 mothers and children) from the public healthcare system.[5] We excluded mothers and their children for any of the following reasons: once the mother or child died (n=127; 10.2%); if the child was HIV-positive (excluded at the assessment after HIV acquisition (n=17; 1.3%)); or if the child was a twin or triplet (n=13; 1.1%). About one out of three children and, sometimes their mothers, moved to the Eastern Cape Province of SA; these children were also reassessed over time and were included in our analyses. Follow-up assessments were conducted for 98.6% at 2 weeks post birth, 94.0% at 6 months, 91.5% at 18 months, 84.9% at 3 years, 82.7% at 5 years, and 82% at 8 years.
Standard care and intervention
SC consisted of access to healthcare at government clinics and hospitals. During the intervention, mothers received home visits by trained community healthcare workers, in addition to the clinic-based standard care.[6]
Child measures
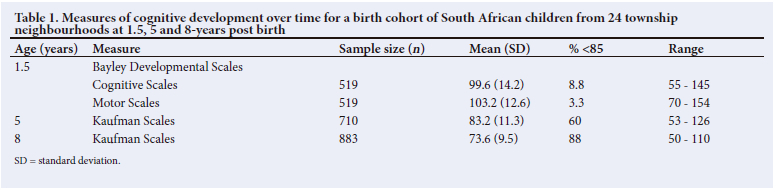
At 1.5 years of age, the Bayley Developmental Scales for Cognitive and Motor Performance,[7] a measure with a mean (SD) value of 100 (15) and a range of 40 - 160, were allocated to a random sample of about half the children (n=519). The Kaufman Developmental Scales were adapted for children in SA and administered to the entire cohort at 5 and 8 years of age. At 5 years and again at 8 years, the Kaufman Developmental Scales were administered, adapted for children in South Africa to the entire sample.[8-10] Each subscale has a mean score of 10; adding each subtest, the global mean was similar to the Bayley Scales, i.e. a mean (SD) value of 100 (15).
Results
At 18 months, the children's cognitive development on the Bayley Scales was normative, similar to the global mean score (Table 1).[7] Less than 10% of the babies had Bayley Scales <1 SD from the global norm, i.e. <85. By 5 years of age, the mean cognitive development was 1 SD below the global SD norm (<85) and 60% of children had scores below the global mean SD. By 8 years of age, cognitive development scores fell another 10 points, a statistically significant decline (controlling for neighborhood: estimate = -9.48; standard error = 0.39; 95% CI -8.16 - -0.15; JK0.001) and 88% of children fell below the norm (SD <85).
While mothers and children in half of the neighborhoods were randomised to receive a perinatal intervention, i.e. a home visit by a community health worker, there were no intervention effects on any child measures at any assessment beyond the 18-month follow-up assessment, and most benefits were evident during the first 6 months of life. Home visits did not impact children's cognitive development at any point. There were no differences in cognitive development based on living in rural areas or in peri-urban townships, or on the gender of the child. On examination of the subsample of children («=519) who received the Bayley Scales at 18 months, followed by the Kaufman Scale scores of those children at 5 and 8 years, the mean (SD) scores and overall results are very similar to the profile for the entire sample (available from the authors upon reasonable request).
Discussion
Donor agencies focus many of their resources on the first 1 000 days of life.[5,7] While this period is certainly crucial and foundational, the loss of children's cognitive potential continues at least through the age of 8 years, as demonstrated in the present study. It is critical that we begin to implement developmental^ linked interventions that can address the conditions leading to loss of potential. Any intervention would have to be implemented beyond the first 1 000 days, as the loss of cognitive potential appears to be more pronounced between the ages of 3 and 8 years.
Certainly, the measures utilised in monitoring children's cognitive development in the present study may be criticised. There are always issues of cultural adaptation when monitoring children's cognitive development and more comprehensive measures may be desirable.[11,12] In particular, SA has initiated the Thrive-by-Five initiative and created its own measure of cognitive development over time (e.g. the Early Learning Outcome Measure). In the present study, we used standardised measures to assess cognitive development, i.e. the Bayley Scales and the Kaufman measure.
Using these standardised measures, we found that children's cognitive development matched the global mean (SD) on the Bayley Scale at 18 months of age. However, among surviving children in a cohort reflecting 98% of all births in a 15-month period in 24 neighborhoods, there appears to be a consistent decline in cognitive developmental potential with age. Similar to the initial findings of the Thrive-by-Five Initiative (April 2022),[11] the magnitude of the loss is substantial and warrants increased focus on activities and interventions that can protect children in LMICs over time, throughout early childhood, as well as attention from policy leaders attempting to achieve the Sustainable Development Goals. Interventions cannot be focused on only the first 1 000 days of life - it has to be sustained during childhood in order to support and build child cognitive development over the life course.
Declaration. None.
Acknowledgements. None.
Author contributions. Equal contributions.
Funding. This work was funded by the U.S. National Institute on Alcohol Abuse and Alcoholism (NIAAA) R01AA017104 and supported by the U.S. National Institutes of Health (NIH) (grant no. MH58107, 5P30AI028697 and UL1TR000124), as well as the Center for HIV Identification, Prevention, and Treatment Services (CHIPTS) (grant no. P30MH58107). MT is supported by the National Research Foundation (SA) and is a lead investigator of the Centre of Excellence in Human Development, University of the Witwatersrand (SA). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Conflicts of interest. None.
References
1. Black MM, Walker SP, Fernald LCH, et al. Early childhood development coming of age: Science through the life course. Lancet 2017;389(10064):77-90. https://doi.org/10.1016/S0140-6736(16)31389-7 [ Links ]
2. World Health Organization. World health statistics overview 2019: Monitoring health for the SDGs (Sustainable Development Goals). Geneva: WHO, 2019. [ Links ]
3. Derbyshire E, Obeid R. Choline, neurological development and brain function: A systematic review focusing on the first 1 000 days. Nutrients 2020;12(6):1731. https://doi.org/10.3390/nu12061731 [ Links ]
4. Schwarzenberg SJ, Georgieff MK, Daniels S, et al. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 2018;141(2):X-X. https://doi.org/10.1542/peds.2017-3716 [ Links ]
5. Rotheram-Borus MJ, le Roux IM, Tomlinson M, et al. Philani Plus (+): A mentor mother community health worker home visiting program to improve maternal and infants' outcomes. Prev Sci 2011;12(4):372-388. https://doi.org/10.1007/s11121-011-0238-1 [ Links ]
6. Le Roux IM, Tomlinson M, Harwood JM, et al. Outcomes of home visits for pregnant mothers and their infants: A cluster randomised controlled trial. AIDS 2013;27(9):1461-1461. https://doi.org/10.1097/QAD.0b013e3283601b53 [ Links ]
7. Ballot DE, Ramdin T, Rakotsoane D, et al. Use of the Bayley Scales of Infant and Toddler Development to assess developmental outcome in infants and young children in an urban setting in South Africa. Int Sch Res Notices 2017;2017:1631760. https://doi.org/10.1155/2017/1631760 [ Links ]
8. Bangirana P, Seggane-Musisi P, Allebeck P, et al. A preliminary examination of the construct validity of the KABC-II in Ugandan children with a history of cerebral malaria. Afr Health Sci 2009;9(3):186-192. [ Links ]
9. Kaufman AS, Lichtenberger EO, Fletcher-Janzen E, Kaufman NL. Essentials of KABC-II assessment. New Jersey: John Wiley & Sons Inc., 2005. [ Links ]
10. Scheiber C, Kaufman AS. Which of the three KABC-II global scores is the least biased? J Pediatr Neuropsychol 2015;1(1):21-35. https://doi.org/10.1007/s40817-015-0004-6 [ Links ]
11. Thrive by Five. The Thrive by Five Index. https://www.thrivebyfive.co.za/ (accessed 25 July 2022). [ Links ]
12. Adebiyi BO, Goldschmidt T, Benjamin F, Sonn IK, Roman NV. Exploring the perspectives of South African parents and primary caregivers living in low-income communities on what children need to thrive within the first 1 000 days of life. Children 2021;8(6):483. https://doi.org/10.3390/children8060483 [ Links ]
 Correspondence:
Correspondence:
J Christodoulou
jchristodoulou@paloaltou.edu
Accepted 17 May 2023


{kind=link}