










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.2 Pretoria Jun. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i2.1937
ARTICLE
The clinical spectrum of Staphylococcus aureus infections in children admitted to Chris Hani Baragwanath Academic Hospital, South Africa: A retrospective, descriptive study
P Raphulu (née Manenzhe)I, II; J WadulaIII, IV, V; D P MooreVI, VII; K L PetersenVIII, IX
IMB ChB, DCH (SA), FCPaed (SA), MMed (Paed), Cert Cardiology (SA) Paed; Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
IIMB ChB, DCH (SA), FCPaed (SA), MMed (Paed), Cert Cardiology (SA) Paed; Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMD, FC Path (SA) Micro, DTM & H, PIDC; Department of Clinical Microbiology & Infectious Diseases, National Health Laboratory Services, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
IVMD, FC Path (SA) Micro, DTM & H, PIDC; School of Pathology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VMD, FC Path (SA) Micro, DTM & H, PIDC; National Health Laboratory Services, Johannesburg, South Africa
VIMB BCh, FCPaed (SA), MMed (Paed), MPhil (Paed ID), Cert Paed ID (SA), PhD; Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
VIIMB BCh, FCPaed (SA), MMed (Paed), MPhil (Paed ID), Cert Paed ID (SA), PhD; Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
VIIIMB BCh, DCH (SA), MMed (Paed), FCPaed (SA), DTM & H, Cert Paed Neph (SA); Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
IXMB BCh, DCH (SA), MMed (Paed), FCPaed (SA), DTM & H, Cert Paed Neph (SA); Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
ABSTRACT
BACKGROUND. Staphylococcus aureus infection is associated with considerable morbidity and mortality. There are relatively few studies describing invasive S. aureus infections in children, particularly in low- and middle-income countries.
OBJECTIVES. To describe the clinical spectrum and outcomes associated with S. aureus infection in children <14 years of age hospitalised at Chris Hani Baragwanath Academic Hospital (CHBAH), South Africa, and to identify risk factors of invasive disease.
METHODS. A retrospective, descriptive study was conducted at CHBAH to define the spectrum of clinical presentation, risk factors, duration of treatment and outcomes of paediatric S. aureus infections for the period January through December 2013. Data were sought for all children <14 years of age.
RESULTS. Four hundred and twenty-two episodes of S. aureus infection were identified. Three hundred and forty-two (81%) infections were caused by methicillin-susceptible S. aureus (MSSA) and 80 (19%) by methicillin-resistant S. aureus (MRSA). Clinical data were obtained for 286 (67.8%) cases, on which all further analyses were based. Clinical presentations for MSSA bacteraemia included skin and soft tissue infection (45%), pneumonia (10%), meningitis (6%), bone/joint infections (5%) and urinary tract infections (3%). Five (8.3%) cases of MRSA were community-acquired. Admission to intensive care unit (ICU) was the only risk factor associated with MRSA infection (adjusted odds ratio (aOR) 125.55; 95% confidence interval (CI) 11.67 - 1 350.68). Hospital-acquired S. aureus infection was the only factor associated with mortality on multivariate analysis (aOR 8.70; 95% CI 1.55 - 48.77).
CONCLUSION. S. aureus is frequently isolated in paediatric bacterial infections. Closer attention to infection control would impact on MRSA and S. aureus mortality rates in our setting.
Staphylococcus aureus is a virulent pathogen, which is associated with considerable morbidity and mortality.[1] Among Gram-positive bacteraemias, S. aureus bacteraemia (SAB) is one of the infections most prevalent and difficult to treat.[2] Most studies have been performed on adults and little is known about bloodstream and other infections due to S. aureus in children, particularly in low- and middle-income countries (LMICs).[3]
Infections caused by S. aureus are often classified in terms of the clinical isolates antibiotic susceptibility to methicillin, as being either methicillin-susceptible (MSSA) or methicillin-resistant (MRSA). MRSA infection may be community-acquired (CA-MRSA) or hospital-acquired (HA-MRSA).[4] CA-MRSA is diagnosed within 48 hours of hospitalisation, in the absence of any medical devices or indwelling catheter, and no recent hospitalisation.[4
Paediatric S. aureus bacteraemia usually presents as bone and joint infection, followed by skin and soft tissue infections (SSTI),[5] although a study from New Zealand reported SSTI in two-thirds of children presenting with S. aureus infection.[6] Malnutrition and HIV infection have been identified as risk factors for SAB, and infection with MRSA.[3,7,8] Other comorbid conditions predisposing to MRSA infection include congenital heart disease and concurrent tuberculosis.[7]
There is a wide spectrum of disease severity in paediatric SAB, with C-reactive protein (CRP), duration of therapy, and length of stay greater in those with complex disease.[9] Most invasive S. aureus infections in paediatric patients are caused by methicillin-susceptible strains as reported in recent studies.[10,11] The epidemiology of MRSA and MSSA has changed in recent years, with an increased risk of paediatric intensive care unit admission, mechanical ventilation and inotropic support associated with MRSA in paediatric patients.[12-A recent study in Iran showed a high prevalence of MRSA of 42% among culture-positive cases of S. aureus. [13] The high prevalence of MRSA in Iranian children may be due to insufficient infection control measures in hospitals, inappropriate use of methicillin, inadequate staff training, and over-prescription of antibiotics.[13] There is wide variation in antibiotic prescription practices among clinicians, corresponding with escalating case complexity and persisting MRSA bacteraemia.[14] Hospital-acquired S. aureus bacteraemia has an increased long-term risk for mortality, particularly in children with chronic diseases.[15]
The aim of the present study was to describe the clinical spectrum and outcomes associated with S. aureus infection in children <14 years of age hospitalised at Chris Hani Baragwanath Academic Hospital (CHBAH), South Africa, and to identify risk factors of invasive disease.
Method
Study design
We conducted a retrospective, descriptive analysis of clinical records of children <14 years hospitalised at CHBAH during the 12-month period from January to the end of December 2013 from whom S. aureus was cultured on clinical specimens. The National Health Laboratory Service (NHLS) Central Data Warehouse was used to identify eligible patients, and case clinical data and demographics were obtained from the electronic patient registry of the Department of Paediatrics and Child Health at CHBAH. A review of clinical records was also undertaken, where possible.
Definitions
Staphylococcus aureus infection was defined as the isolation of S. aureus from clinical specimens, including blood, cerebrospinal fluid, pleural fluid, pericardial fluid, pus, tissue, synovial fluid and urine. In patients with multiple specimens positive for S. aureus, a single episode of S. aureus infection was defined if the organism was isolated within 21 days of a previous positive specimen.
MRSA was defined as S. aureus resistant to methicillin on laboratory testing.
Community-acquired MRSA was defined as MRSA isolated from a patient in the outpatient environment, or within 48 hours of hospitalisation, with no history of prior HA-MRSA infection, hospitalisation, indwelling device, or residence in a long-term care facility.
Hospital-acquired MRSA was defined as MRSA isolated from a patient beyond 48 hours into a hospitalisation episode; or MRSA isolated from admission blood cultures in children with a history of prior hospitalisation, indwelling devices, a prior history of HA-MRSA infection, or who were resident in long-term care facilities.
Malnutrition was classified according to the World Health Organization (WHO) growth standards. Moderate malnutrition was defined as weight-for-height between -2 and -3 standard deviations (SD) below the mean. Severe malnutrition was defined as weight-for-height less than -3 SD below the mean, or the presence of oedema.
HIV infection was confirmed by the presence of a positive HIV PCR in children <18 months of age, or a positive HIV ELISA in children >18 months of age.
Statistical analysis
Descriptive statistics presented continuous variables as means and standard deviations (SDs) for normally distributed data, and as medians with interquartile ranges (IQRs) for skewed data. Student's i-test was used to compare means, and the Mann-Whitney U test was used to compare medians. Risk factors for S. aureus infection were deduced by univariate and multivariate logistic regression analysis. Odds ratios and 95% confidence intervals (95% CIs) were used to describe risk factors. Two-sided p-values <0.05 were considered significant. Data were analysed using Stata version 12.0 (StataCorp, College Station, Texas).
Ethical considerations
Approval was obtained from the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (Ethics Clearance Certificate: M140729) and from the hospital.
Results
Between January and end-December 2013, 422 episodes of S. aureus infection were identified in children <14 years of age. Three hundred and forty-two (81%) infections were caused by MSSA and 80 (19%) by MRSA isolates. Demographic and clinical data were obtained for 286 (67.8%) patients. Subsequent analyses were done on the subset of children (n=286) in whom a record review was conducted, except for the descriptive analysis of antibiotic susceptibility profiles of the isolates (which were available for all 422 S. aureus infection episodes).
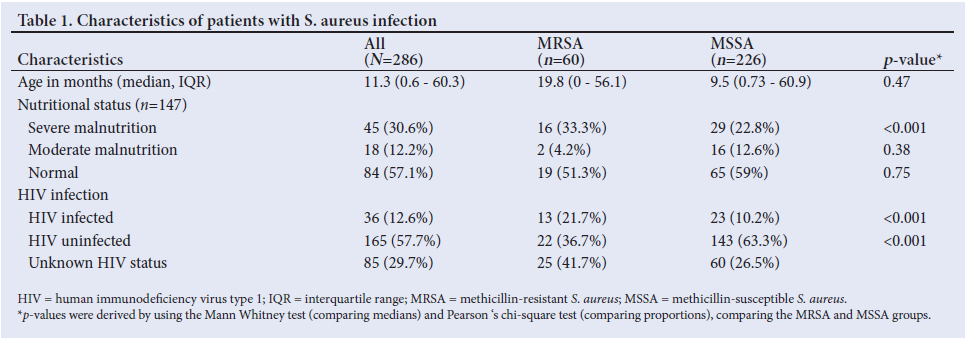
Characteristics of patients with S. aureus infection
The median age of patients from whom S. aureus was cultured, was 11.3 months (IQR 0.6 - 60.3 months). One hundred and sixty-five (57.7%) patients were HIV uninfected, and 36 (12.6%) were HIV infected (Table 1). HIV status was not documented for 85 (29.7%) children.
Nutritional status was determined for 147 (51.3%) patients and, of these, 84 (57.1%) had normal nutritional status, 18 (12.2%) were moderately malnourished and 45 (30.6%) were severely malnourished (Table 1).
Two hundred and fourteen (74.8%) of the 286 patients had community-acquired infections and72 (25.2%) had hospital-acquired infections. Of the 214 patients who had community-acquired infections, 209 (97.7%) cultured MSSA and 5 (2.3%) cultured MRSA. Clinical data were available for 3 of the 5 children with CA-MRSA. In the group with hospital-acquired infection (n=72 patients), 56 (77.8%) cultured MRSA and 16 (22.5%) cultured MSSA.
Spectrum of clinical presentation
MSSA was significantly associated with SSTI, whereas MRSA was associated with septic wounds.
Duration of hospital stay
The median duration of hospitalisation for all patients was 11 days (IQR, 5 - 24 days). The median duration of hospitalisation was significantly longer in children with MRSA (35 days; IQR 24 -65 days) compared with those with MSSA infection (8 days; IQR 4 - 18 days), p<0.001.
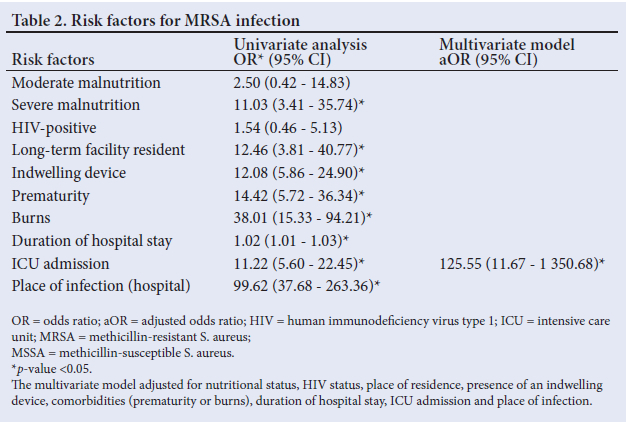
Risk factors for MRSA infection
Factors associated with MRSA infection on univariate analysis included severe malnutrition, residence in a long-term facility, presence of an indwelling device, prematurity, burns, prolonged hospitalisation, intensive care unit (ICU) admission and acquisition of infection in the hospital setting (Table 2). On multivariate analysis, only acquisition of infection during hospitalisation, specifically during an admission to ICU, retained significance as a risk factor for MRSA infection (Table 2).
Antibiotic susceptibility and management
Antimicrobial susceptibility patterns were available for all of the clinical isolates (N=422). MSSA episodes were susceptible to most antimicrobials against which they were tested, although 98.9% were resistant to penicillin. All of the MRSA isolates were susceptible to vancomycin.
Among the 286 children with clinical folders available for review, empiric antibiotics commonly used for community-acquired infections included cloxacillin (54.3%), amoxicillin-clavulanate (28.5%) and cefotaxime or ceftriaxone (14.5%). Vancomycin was used empirically for most hospital-acquired infections (53.1%). The median duration of treatment for all groups of S. aureus infections was 12 days (IQR 5 - 21 days). Twenty-seven (10.8%) patients, all of whom had S. aureus infection of septic wounds, did not receive any antibiotics. These patients were treated with antiseptic dressings only.
Duration of antibiotic therapy according to S. aureus syndrome
The duration of antibiotic treatment varied according to the clinical diagnosis. Patients with bone and joint infections (n=13) and infective endocarditis (n=1) were treated for a median of 6 weeks (IQR 3 - 8 weeks) of antibiotic therapy. Children with meningitis (n=17) were treated for a median of 3 weeks (IQR 2 - 6 weeks). All other groups of S. aureus infection were treated for a median duration of 12 days (IQR 5 - 21 days). Five patients with persistent SAB were treated with a combination of cloxacillin and fusidic acid, for a median of 14 days (IQR 13 - 20 days). In addition to antibiotic therapy, 2 patients who presented with empyema had intercostal drain insertion and subsequently underwent videoassisted thoracoscopic surgery.
Outcome
There were 22 (7.7%) deaths in total among the 286 children with available clinical records, of which 17 were due to HA-MRSA infections and 5 were community acquired. Four (18.2%) of the patients who died (3 with MRSA and 1with MSSA infection) were not initiated on appropriate antimicrobial therapy before time of death. The remaining 18 (18/22, 81.8%) patients who died were on appropriate antimicrobial therapy for a median duration of 6 days (IQR 5 - 14 days) before time of death. Children with community-acquired infections had a better outcome.
Of the 17 patients with HA-MRSA who died, 10 (58.8%) had septic burn wounds, 4 (23.5%) had bacteraemic pneumonia, 2 (11.8%) had bacteraemia without a focus and 1 (5.9%) had infective endocarditis.
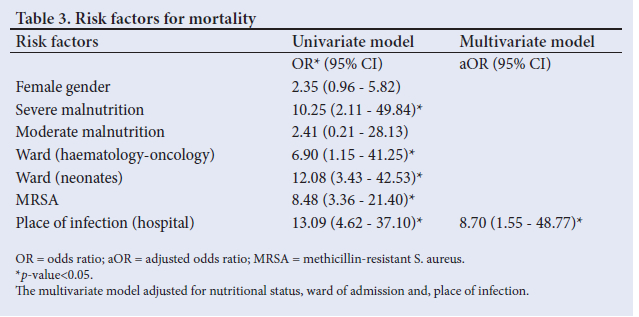
Risk factors for mortality
On univariate analysis, hospital-acquired infection, severe malnutrition, MRSA infection, children with haematology/oncology conditions and critically ill newborns were factors associated with mortality. However, on multivariate analysis, only acquisition of infection from the hospital setting were independently associated with mortality (Table 3).
Discussion
S. aureus is an important pathogen contributing to prolonged hospital stay and morbidity in paediatric patients. In this series of paediatric patients with S. aureus infection, hospitalised over a 12-month period, there was on average over one S. aureus episode diagnosed each day across neonatal, general paediatric and surgical disciplines. Most (81%) invasive S. aureus infections in our retrospective study were caused by methicillin-susceptible strains, although MRSA should be considered, particularly in the context of hospitalised patients. CA-MRSA infections appear to have been uncommon in our setting during the study period; however, more recent studies are required as MRSA epidemiology appears to be changing.
Two published South African studies have described the epidemiology of SAB in children in the 21st century to date. A retrospective study from Soweto identified 161 episodes of community-onset SAB over a 2-year period (January 2005 to December 2006), with an incidence of 26/100 000.[16] Sixty-three (39%) of the 161 isolates were identified as MRSA, with an incidence if 10/100 000.[16] A study from Cape Town reported 365 episodes of SAB over a 5-year period (January 2007 to December 2011).[7]
Rates of MRSA have been trending upwards in paediatric studies, ranging between 10% and 24%,[7,16-18] with an increasing incidence in nosocomial SAB described in Cape Town accounting for ~half of all cases of MRSA SAB in that study.[7] In both South Africa and the United Kingdom, MRSA was found to be the most significant risk factor associated with a high mortality rate among children with SAB.[7,19]
Paediatric S. aureus infections appear to affect different age groups, depending on the populations studied. South African studies show a predilection of S. aureus infections in the younger age groups.[7] whereas studies from Canada and New Zealand show that older children are more prone to S. aureus infections requiring hospitalisation.[5, 6] The reason for these age differences may be related to the social determinants of health, including malnutrition, overcrowding, poverty and lack of sanitation, which are prevalent in LMICs.
SSTIs (n=102/226, 45.1%) were the most common clinical presentation for children with MSSA in our study, and septic wounds (n=25/60, 41.7%) constituted the most common presenting condition in those with MRSA infection. That septic wounds were the most common clinical presentation in children with MRSA infection in our study speaks to inadequate attention to infection prevention and control practices in our setting. Pneumonia and bacteraemia without a focus occurred in 12% and 10% of children, respectively. Infective endocarditis was an uncommon clinical presentation of S. aureus infection in our study, similar to findings from other centres, but had a high case-fatality rate.[6,7]
Other South African studies have shown higher rates of MRSA in children who are HIV infected.[7, 816, 20] In our case series, 36.1% of HIV-infected patients had MRSA, whereas only 13.3% of the HIV-uninfected children had MRSA infections; however, on multivariate analysis, HIV infection status was not identified as being a risk factor for MRSA infection.
The problem of limited availability of cloxacillin has arisen as a major challenge to targeted therapy of MSSA infections in the past five years, and reflects a global shortage of supply of this key anti-staphylococcal agent. In children hospitalised with infectious syndromes, such as SSTI or bone and joint infections likely to be caused by S. aureus, alternative antibiotic agents with anti-staphylococcal activity, e.g. co-amoxiclav, cefazolin or ceftriaxone, is justified.
Children with hospital-acquired infections had 9 times greater adjusted odds of dying compared with those with community-acquired infections. The overall case fatality rate in the study was 7.7% - slightly lower in comparison with case fatality rates of 8.8% and 8.6% in Cape Town and New Zealand, respectively.[6, 7] The reason for the lower case fatality rate in our study is probably related to the inclusion of local cellulitis cases, and not only SAB cases as in the other studies. The substantially higher case fatality in patients with hospital-acquired infections observed in our study of 17/72 (23.6%) is similar to findings from other South African studies.[7,16]
The present retrospective analysis has limitations, foremost of which is the lack of availability of archived records, and by inconsistent or incomplete clinical documentation in those cases in which record review was possible. Nevertheless, the data presented in this study are important in improving the management and outcome of paediatric S. aureus infections at institutional, national and regional levels, particularly in low- to middle-income settings. The data presented in this study are from patients admitted in 2013, and may not reflect the current situation. However, this study contributes to a deeper understanding of the epidemiology of paediatric S. aureus infections in South Africa, and bridges the gap between older studies and studies which will be conducted in future.
Conclusion
Acquisition of infection in hospital was the only risk factor associated with MRSA infection and mortality in multivariate logistic regression analyses in our study. Efforts must be made to reinforce optimal infection prevention and control practice in order to prevent infection with hospital-acquired organisms. We would also support the use of empiric vancomycin for patients with clinical features indicative of HA-MRSA infection. Clinical syndrome, culture results and response to antibiotic therapy should guide duration of treatment. Surgical intervention should be sought timeously in cases with empyema, SSTI, bone or joint infections, or for source control in cases with persistently positive blood cultures.
Declaration. The research was done in fulfilment of the requirements for PR's Master of Medicine degree at the University of the Witwatersrand.
Acknowledgements. The authors acknowledge the support of the National Health Laboratory Services at the Chris Hani Baragwanath Academic Hospital during data collection.
Author contributions. PR and KLP conceptualised the study and study design. PR did the data collection. PR and DPM performed statistical analysis of the data. JW offered data collection support from the National Health Laboratory Services at Chris Hani Baragwanath Academic Hospital. All the authors (PR, JW, DPM and KLP) contributed to writing and reviewing the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Naber CK. Staphylococcus aureus bacteremia: Epidemiology, pathophysiology, and management strategies. Clin Infect Dis 2009;48(s4):S231-S237. [ Links ]
2. Eshwara VK, Munim F, Tellapragada C, et al. Staphylococcus aureus bacteremia in an Indian tertiary care hospital: Observational study on clinical epidemiology, resistance characteristics, and carriage of the Panton-Valentine leukocidin gene. Int J Infect Dis 2013;17(11):e1051-e1055. [ Links ]
3. Ladhani S, Konana OS, Mwarumba S, English MC. Bacteraemia due to Staphylococcus aureus. Arch Dis Child 2004;89(6):568-571. [ Links ]
4. So TY, Farrington E. Community-acquired Methicillin resistant Staphylococcus aureus infection in the paediatric population. J Pediatr Health Care 2008;22(4):211-217. [ Links ]
5. Vanderkooi OG, Kellner JD, Laupland KB. Staphylococcus aureus bloodstream infections in children: A population-based assessment. Paediatr Child Health 2011;16(5):276-280. [ Links ]
6. Miles F, Voss L, Segedin E, Anderson BJ. Review of Staphylococcus aureus infections requiring admission to a paediatric intensive care unit. Arch Dis Child 2005;90(12):1274-1278. [ Links ]
7. Naidoo R, Nuttall J, Whitelaw A, Eley B. Epidemiology of Staphylococcus aureus bacteraemia at a tertiary childrens hospital in Cape Town, South Africa. PLoS One 2013;8(10):e78396. [ Links ]
8. Fortuin-de Smidt MC, Singh-Moodley A, Badat R, et al. Staphylococcus aureus bacteraemia in Gauteng academic hospitals, South Africa. Int J Infect Dis 2015;30:41-48. [ Links ]
9. Kashif M, Ansari YI, Ekram T, Khan F, Nawab T, Abqari S. Clinical spectrum and resistance pattern of community-acquired invasive Staphylococcus aureus infection in children. J Patient Saf Infect Control 2018;6(2):33-37. [ Links ]
10. Munro A, Blyth C, Campbell AJ, Bowen AC. Infection characteristics and treatment of Staphylococcus aureus bacteraemia at a tertiary children's hospital. BMC Infect Dis 2018;18(1):387. [ Links ]
11. Crandall H, Kapusta A, Killpack J, et al. Clinical and molecular epidemiology of invasive Staphylococcus aureus infection in Utah children; continued dominance of MSSA over MRSA. PLoS One 2020;15(9):e0238991. http://doi.org/10.1371/journal.pone.0238991 [ Links ]
12. Camancho-Cruz J, Gutierrez IF, Brand-Lopez, et al. Differences between Methicillin-susceptible versus Methicillin-resistant Staphylococcus aureus infections in Pediatrics. Pediatr Infect Dis J 2022;41:12-19. [ Links ]
13. Sarrafzadeh F, Sohrevardi SM, Abousaidi H, Mirzaei H. Prevalence of methicillin-resistant Staphylococcus aureus in Iranian children: A systematic review and meta-analysis. Clin Exp Pediatr 2021;64(8):415-421. [ Links ]
14. Campbell AJ, Tong SYC, Bowen AC. Infectious diseases clinician's variation in the management of pediatric Staphylococcus aureus bacteraemia and equipoise for clinical trials. Front Pediatr 2019;7:249 http://doi.org/10.3389/fped.2019.00249 [ Links ]
15. Oren G, Matan J, Itai G, et al. Staphylococcus aureus bacteraemia in children: Antibiotic resistance and mortality. Pediatr Infect Dis J 2019;38(5):459-463. [ Links ]
16. Groome MJ, Albrich WC, Wadula J, Khoosal M, Madhi SA. Community-onset Staphylococcus aureus bacteraemia in hospitalised African children: High incidence in HIV-infected children and high prevalence of multidrug resistance. Paediatr Int Child Health 2012;32(3):140-146. [ Links ]
17. Denniston S, Andrew F, Riordan I. Staphylococcus aureus bacteraemia in children and neonates: A 10 year retrospective review. J Infect Dis 2006;53(6):387-393. [ Links ]
18. Britton PN, Andresen DN. Paediatric community-associated Staphylococcus aureus: A retrospective cohort study. J Paediatr Child Health 2013;49(9):754-759. [ Links ]
19. Adedeji A, Gray JW. MRSA at an English children's hospital from 1998 to 2003. Arch Dis Child 2005;90(7):720-723. [ Links ]
20. Jaspan HB, Huang LC, Cotton MF, Whitelaw A, Myer L. Bacterial disease and antimicrobial susceptibility patterns in HIV-infected, hospitalised children: A retrospective cohort study. PLoS One 2008;3(9):e3260. [ Links ]
 Correspondence:
Correspondence:
P Raphulu (née Manenzhe)
Phophi.Manenzhe@wits.ac.za
Accepted 7 February 2023


{kind=link}
{kind=link}
{kind=link}