










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.2 Pretoria Jun. 2023
http://dx.doi.org/10.7196/SAJCH.2023.v17i2.1954
ARTICLE
Accidental poison exposure among children in a regional hospital in northern KwaZulu-Natal before and during the COVID-19 pandemic
R VoslooI, II; U NaidooIII
IMB ChB, DCH (SA), FCPaed (SA), MMed (Paed); Department of Paediatrics and Child Health, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, DCH (SA), FCPaed (SA), MMed (Paed); Department of Paediatrics, Queen Nandi Regional Hospital, Empangeni, South Africa
IIIMB ChB, DCH (SA); Department of Paediatrics, Queen Nandi Regional Hospital, Empangeni, South Africa
ABSTRACT
BACKGROUND. Poisoning has been reported as the fifth most common cause of injury-related deaths in children younger than five years worldwide. Little is known about accidental poison exposure among children at regional hospital level. Regional hospitals generally provide more specialised support to primary care facilities over a larger area. During the COVID-19 pandemic, lockdown measures may have increased home-based unintentional poisoning.
OBJECTIVES. To determine the frequency, outcome and type of accidental poison exposure in children admitted to a regional hospital and compare cases before and during the COVID-19 pandemic.
METHODS. A review of admissions to Queen Nandi Regional Hospital in Empangeni was performed to document cases of accidental poison exposure over two years. Equal periods during 2019 and 2020 (April to December) were then compared. Children <13 years of age were included. Age, sex, date of admission, death or survival and type of poisoning were collected.
RESULTS. Cases of accidental poison exposure made up a small proportion of the total admissions over two years (n=252/5 071, 4.97%) with a low case fatality rate (0.40%). Boys made up the majority (n=132/252, 52.38%). Most were <five years old (n=220/252, 87.30%). Medicines (n=114/252, 45.24%), hydrocarbons (n=59/252, 23.41%) and pesticides (n=26/252, 10.32%) were the main types of poison. Domestic cleaner-, sanitiser- and disinfectant-related admissions were significantly increased during the pandemic (p=0.020).
CONCLUSION. Accidental poison exposure occurs commonly in younger children. Medicines, hydrocarbons and pesticides made up the majority of cases. Domestic cleaner, hand sanitiser and disinfectant ingestion increased in the pandemic. Future research should involve primary care facilities, and risk factors as well as clinical severity should be investigated.
Poisoning has been reported as the fifth most common cause of injury-related deaths in children younger than five years worldwide. [1] It occurs when cells are damaged or destroyed by the inhalation, ingestion, injection or absorption of a toxic substance.[2] Accidental poisoning commonly occurs in children <five years.[3] In South Africa (SA), paediatric poisoning is not well documented. Reporting is available from Poisons Helpline data and through hospital admissions. Although overall case fatalities from accidental poisoning in children are rare, there appears to be an increase in poisoning-related deaths in low-and-middle-income countries (LMICs). The case fatality rate for poisoning in children in the USA was 0.30 cases per 100 000 population while in LMICs in Africa the case fatality rate was 4 cases per 100 000 population in 2004.[2] Various community-based interventions to prevent poisoning in children have been implemented across the world, including SA. These have achieved limited success.[4]
There are few reported data on the indirect impact of COVID-19 on accidental poisoning in children in sub-Saharan Africa.[5] The national lockdown in SA was implemented in April 2020 with varying degrees of restrictions ranging from level 5 to level 1. Mitigating measures included the closure of childcare and early education facilities.[6] This limited adult supervision. The lack of contact with extended families may have also restricted family-based support.[5] Economic impacts of the pandemic and its control measures led to a decrease in household incomes.[7] These are significant risk factors for accidental poisoning in children.[8] An increase in certain types of poisoning may have been observed.[9]
Objectives
The present study aimed to determine the frequency, type and outcomes of children admitted with accidental poison exposure to Queen Nandi Regional Hospital (QNRH) and to compare cases before and during the COVID-19 pandemic.
Method
This was an observational retrospective study. The patient register was used to identify all admissions to paediatric wards and specify those with accidental poison exposure. Medical records of identified cases with missing data on the register were retrieved. The study included children <13 years of age, admitted from 1 January 2019 to 31 December 2020. Two equal periods were then compared to assess the effect of the COVID-19 pandemic. The period before the pandemic (before COVID-19) included April 2019 to December 2019. The period during the pandemic (during COVID-19) included April 2020 to December 2020. The study excluded children with non-accidental poison exposure such as intentional administration of traditional medicine, i.e. culturally specific remedies that may include a mixture of plants and other manufactured products. For children admitted with accidental poison exposure, age, sex, date of admission, type of substance and outcome (death or survival) were recorded. Data were stored on the principal investigator's password-protected computer. Patient confidentiality was maintained.
Setting
The hospital is situated in Empangeni in northern KwaZulu-Natal. It provides level 2 maternal, gynaecological and child health services while also delivering primary, and some tertiary, level services. The local district of King Cetshwayo is a mixed rural and urban setting. Two other districts, namely uMkhanyakude and Zululand, are classified as rural and also refer to QNRH.[10] The paediatrics department maintains three general paediatric wards, an outpatient department, and a six-bed paediatric intensive care unit (PICU). All cases of accidental poisoning are admitted.
Data analysis
Data were entered on an Excel spreadsheet and analysed using Stata version 14 (StataCorp, USA). Normally distributed data were described using means and standard deviations (SDs). Non-parametric data were described as medians and ranges. Total admissions and accidental poison exposure cases per month were normally distributed and compared using the Bonferroni analysis of variance (ANOVA). Age distribution was non-parametric and compared with time periods and different substances using the Kruskal-Wallis one-way ANOVA. Categorical variables were analysed using the χ2 test. A significance level p=0.05 was used.
Approval
Institutional and provincial department of health approval was sought. Ethics approval was granted by the hospital ethics committee and the University of KwaZulu-Natal's Biomedical Research Ethics Committee (BREC 00001916/2020).
Results
A total of 5 071 patients were admitted during the two-year period. Of these, 278 were admitted with accidental poison exposure. Twenty-six patients were excluded owing to incomplete or unavailable records.
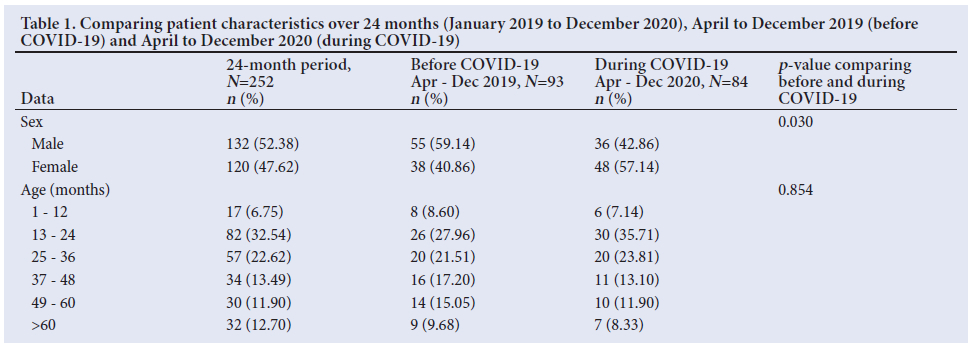
More than half (n=132/252, 52.38%) of the admissions with accidental poison exposure were male (Table 1). There were significantly more boys admitted in the period before COVID-19 (n=55/93, 59.14%) with a larger percentage of girls admitted during COVID-19 (n=48/84, 57.14%)(p=0.030). There was no correlation observed between sex and type of poison (p=0.363).
Most patients were <5 years old (n=220/252, 87.30%), with half of the cases <3 years (median 31 months, range 7 months to 12 years). There was no difference observed in age between the periods (p=0.864). There was no overall difference in ages observed between boys and girls across both periods (p=0.056).
Most patients (n=251/252, 99.60%) were successfully discharged and there were no transfers to the referral centre. One death was observed: a 7-year-old boy who died after accidentally ingesting an unknown substance in 2019.
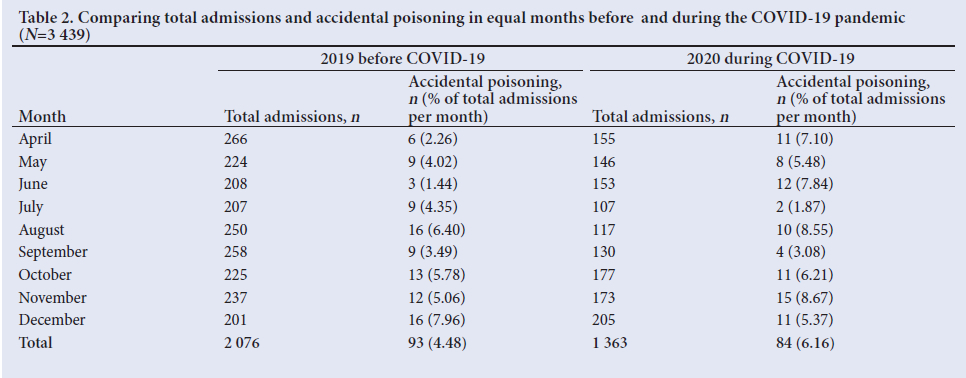
A marked reduction in monthly admissions was observed during COVID-19 (Table 2). The mean (SD) monthly admissions were 253 (32) before COVID-19, and 134 (19) during COVID-19 (p=0.000). Although there were more patients admitted with accidental poison exposure before COVID-19, this did not appear to be significant (p=0.311). During COVID-19, the relative proportion of cases were higher (n=84/1 363, 6.16%) than before COVID-19 (n=93/2 076, 4.48%). However, the relative increase was not significant (p=0.085). The period of hard lockdown (level 4 and 5: from 26 March to 31 May) also did not demonstrate a significant increase in cases of poisoning (p=0.445) or the relative proportion of cases of poison exposure to total admissions (p=0.119) when comparing 2020 and 2019. The less restrictive period (levels 1, 2 and 3: from 1 June to 31 December) also did not show an increase in cases of poison exposure (p=0.465) or the relative proportion of cases to total admissions (p=0.446).
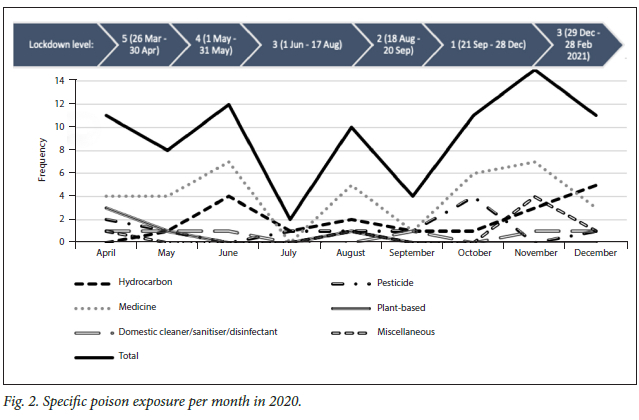
Figures 1 and 2 demonstrate the different categories of poison observed per month for each period. The period of hard lockdown and the less restrictive levels (i.e. levels 1, 2 and 3) were compared with equal periods in 2019. No significant difference in the type of poisoning was observed during levels 4 and 5 (p=0.301) or levels 1, 2 and 3 (p=0.443). However, relative trimodal peaks in medicine ingestions were seen across both years. Hydrocarbons also showed a slight peak in August 2019 and June 2020, with a marked increase towards the end of both years. Pesticides appeared to increase towards the end of both years and domestic cleaner, sanitiser and disinfectant ingestion appeared more common in the first few months during COVID-19, as well as September, November and December during COVID-19. Plant-based ingestions were seen in April and May of both years and a slight increase was observed in August of 2019. Miscellaneous ingestions appeared to peak in November of both years.
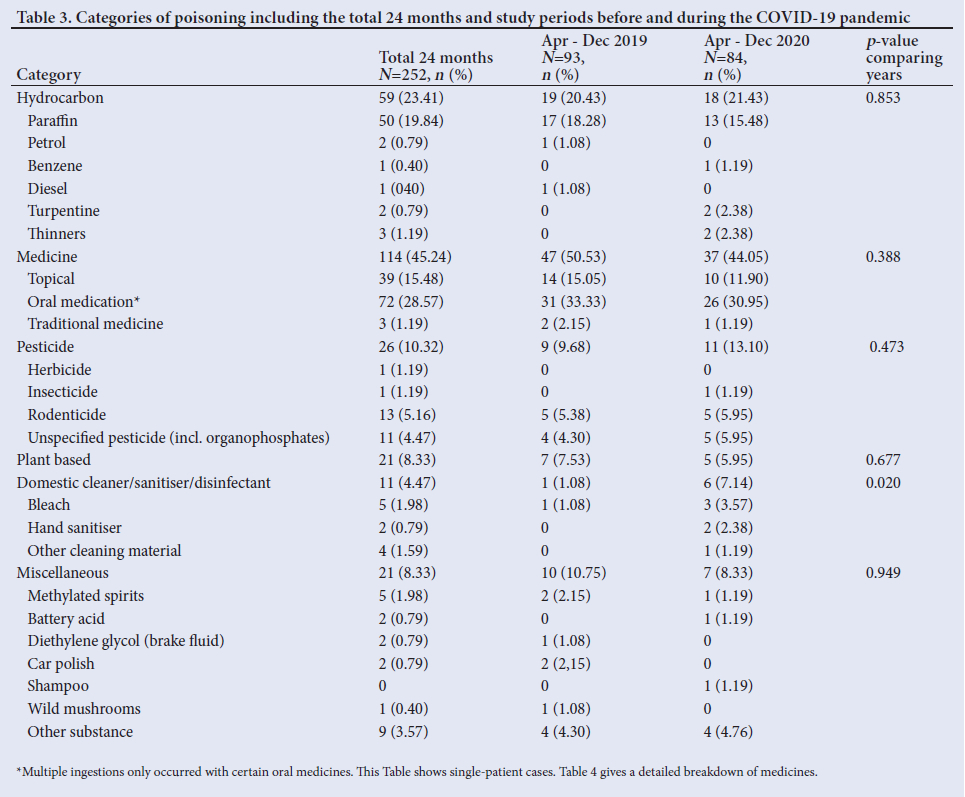
Table 3 describes the different substance categories. Although not significant, hydrocarbons were generally observed in younger children when comparing the ages of all other cases across 2019 and 2020 (median 26 months, range 11 to 128 months) (p=0.0816), while medicine-related ingestions (median 36 months, range 7 to 149 months) (p=0.016) and plant-based poisonings (median 45 months, range 10 to 102 months) (p=0.014) were seen in older children. There was no overall difference in poisoning substances between the two periods (p=0.205). However, there was a statistically significant increase in the number of domestic cleaner-, sanitiser- and disinfectant-related admissions during COVID‑19 (n=6/7, 85.71%) (p=0.020). Bleach was the most common type of domestic cleaner (n=3/6, 50.00%%) during COVID‑19. Hand sanitiser poisoning was only observed in 2020 (n=2/6, 33.33%). Other cleaning materials during COVID‑19 included one case of biocide ingestion (n=1/6, 16.67%).
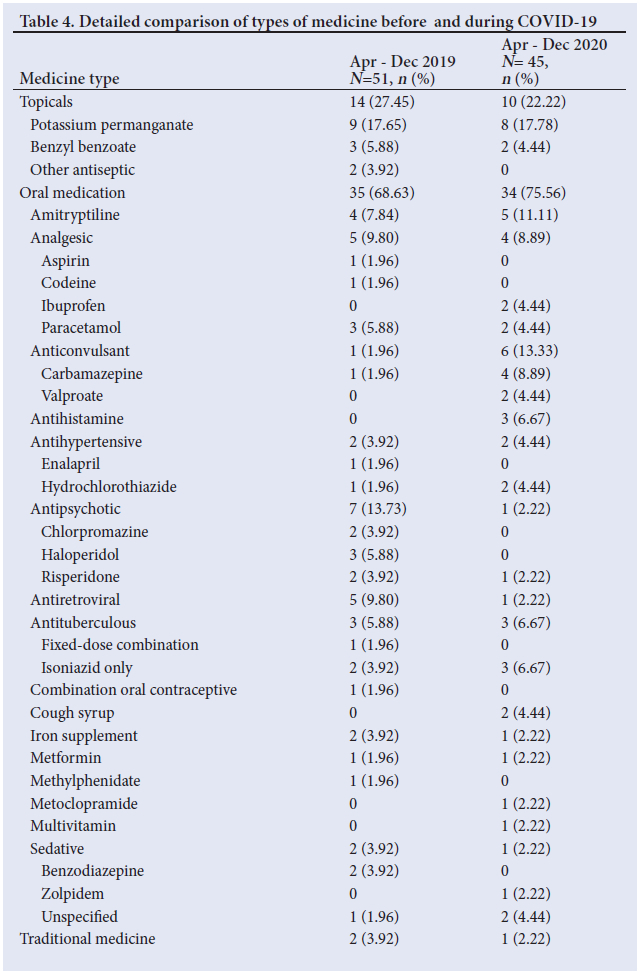
Medicines (including both allopathic medicine and traditional medicine) made up almost half of all cases (n=114/252, 45.24%). A detailed breakdown of medicines is shown in Table 4.
Among hydrocarbons, paraffin was the most prevalent (n=50/59, 84.76%). Pesticides were relatively common (n=26/252, 10.32%), with organophosphatebased pesticides (n=11/26, 42.31%) and rodenticides (n=13/26, 50.00%) comprising the majority. All unspecified pesticides were organophosphate-based, as per the presenting toxidrome.
Plant-based compounds did not represent a large proportion (n=21/252, 8.33%). Before COVID‑19, these included 3 cases of unspecified plant seed ingestion (n=3/7, 42.86%), 2 cases of unspecified wild plant fruit ingestion (n=2/7, 28.57%) and 2 cases of unspecified plant ingestion (n=2/7, 28.57%). During COVID‑19, the cases included 2 with unspecified wild plant fruit ingestion (n=3/5, 60.00%), 1 of wild plant flower ingestion (n=1/5, 10.00%), and 1 of unspecified plant ingestion (n=1/5, 10.00%).
There were 17 miscellaneous poison exposures with most seen in the period before COVID‑19. Other miscellaneous substances not noted in Table 3 include 1 ingestion of a 'liquid used to clean bananas' (n=1/10, 10.00%), 2 ingestions (n=2/10, 20.00%) of organic material including 'lizard faeces' and 'worm ingestion', and 1 ingestion of an unspecified poison (n=1/10, 10.00%) before COVID‑19. During COVID, 1 case of 'hair relaxer' ingestion (n=1/7, 14.29%), 1 case of unspecified corrosive poison (n=1/7, 14.29%), and 2 cases of accidental ingestion of 'chemicals used to burn grass' (n=2/7, 28.57%) were seen.
Discussion
In the present study, accidental poison exposure made up a relatively small number of the total paediatric admissions. However, proportionately more cases were seen during COVID-19. The low death rate reflects a good overall outcome.
Some studies have shown overall higher cases of accidental poisoning in males while others observe a larger proportion of females in older age groups.[3,8,11] Although male patients made up more than half of the cases in our study, it is unclear what could have contributed to the significantly higher number of females seen during COVID-19. Contemporary data have demonstrated that intentional poisoning is more common in older age groups and females.[3,11] However, as our study did not include intentional poisoning, this difference in sex distribution before and during COVID-19 should be interpreted with caution.
Younger children made up the majority of cases, as in other studies.[2,11,12] A bimodal peak in ages has been described elsewhere referring to an increased incidence in acute poisoning in children aged 3 years, coinciding with the explorative phase of psycho-emotional development, and a second peak around adolescence.[12] This second peak could be linked to intentional self-injury.[11] The absence of this peak in our study population is possibly related to the exclusion of non-accidental poisoning.
The significant reduction in total admissions during COVID-19 was in keeping with data from the rest of KwaZulu-Natal.[10] The monthly peaks in different substances across both years did not coincide with specific lockdown periods but could be related to other factors such as seasonal changes or school holidays (Figs 1 and 2).[13]
The relatively large number of cleaning compound-related admissions seen during 2020 is comparable to a study in the USA demonstrating an increase in cleaning and disinfectant chemical exposure and the increased use of these products during the pandemic.[9] Household cleaning products contributing to childhood poisoning have increased over the past two decades.[8] The National Poison Data System in the USA has reported a 36.70% increase in hand sanitiser poisoning.[9] We could be seeing more of this potentially harmful poisoning.
In a contemporary SA study, almost a quarter of accidental poisonings in children were medicine related.[14] In most countries, pharmaceuticals are the leading cause of poisoning;[11] this highlights the importance of safer storage practices in the home environment.[1]
Accidental traditional medicine ingestion was uncommon and only one case was observed during COVID-19. These culturally specific remedies may include a mixture of plants and other manufactured products. As the study only looked at accidental ingestion, intentional use including prescribed remedies from a traditional health practitioner (THP) was probably still common, although not included in the present study.
A study that explored potassium permanganate use by South African THPs demonstrated that this substance is commonly used for healing skin rashes and wounds, and relieving aches, pains and swellings and gastrointestinal aches and cramps.[15] Potassium permanganate use was equally common both before and during COVID-19. Most ingestions with potassium permanganate occur after the crystals are mixed with water, which has milder effects.[16] The specific formulation was not documented in our study population.
Overall, hydrocarbon exposure increased from October to November in both 2019 and 2020. In the domestic setting, hydrocarbons are often used in paints, varnishes, glues, lacquers and cleaning agents.[17] Paraffin poisoning was common, highlighting its continued use as a fuel for cooking and indoor lighting. On the other hand, petrol and diesel were less common during COVID-19; this could be due to limited accessibility under lockdown measures. A recent Australian study demonstrated a correlation between developmental age and type of poisoning. Younger children had significantly higher odds of experiencing non-medication-related poisoning.[18] This finding is in keeping with our study, showing an increase in hydrocarbon-related poisoning in younger children.
Rodenticides and organophosphate-based substances were the main pesticide observed and were almost equally common both before and during COVID-19. The commoner plant-based poisonings are expected in northern KwaZulu-Natal with its sub-tropical climate and abundant vegetation.[13] The generally older age in these poisonings (majority >3 years) alludes to greater mobility and outdoor exploration with increasing age.[19]
Study limitations and strengths
The retrospective observational nature of the study limits its generalisability. Incomplete data and difficulty in medical record retrieval led to the exclusion of some patients. The study period was relatively short and it did not compare the whole year before and during the COVID-19 pandemic. As many poisonings present to primary care, this study is most likely not fully representative of all cases of accidental paediatric poison exposure.
To our knowledge, this is the only study observing accidental poison exposure among children in a rural and semi-urban setting in recent years. It provides essential information on trends and outcomes of common accidental poisonings. Accidental poison exposure cases had a low case-fatality rate. However, length of stay, interventions required and complications were not analysed and conclusions on morbidity could not be drawn.
Conclusion and recommendations
Cases of accidental poison exposure in children are infrequent and demonstrate low case fatality in our setting. Although not significant, the relative proportion appeared to be larger during the COVID-19 pandemic.
Medication, hydrocarbons and pesticides were the most common forms of poison exposure. Domestic cleaner, hand sanitiser and disinfectant ingestion increased in the COVID-19 pandemic, and health practitioners should be aware of the management of common forms of poisoning and the changing profiles related to the impact of the pandemic. Accidental poisoning is more common in younger children, which emphasises the need for awareness of the risk of poisoning at home. Home safety education campaigns and active involvement of community caregivers to improve safe storage practices could be beneficial. Home safety devices and regulations for safe packaging of medicines and other potentially poisonous substances have been proven to reduce cases. More studies are needed to determine the effectiveness of these strategies in our setting.[4,19,20]
Future research could involve primary care facilities to investigate differences in poisoning profiles by area and different time periods. Risk factors and circumstances related to poisoning as well as clinical severity should be investigated.
Declaration. None.
Acknowledgements. The authors would like to thank Ms D Pearce for assisting in data collection.
Author contributions. RV initiated and oversaw the study and performed data analysis. UN performed data collection. Both RV and UN drafted the manuscript and approved the final form.
Funding. Self-funded.
Conflicts of interest. None.
References
1. Kendrick D, Young B, Mason-Jones AJ, et al. Home safety education and provision of safety equipment for injury prevention (Review). Evid Based Child Health 2013;8(3):761-939. https://doi.org/10.1002/ebch.1911. PMID: 23877910 [ Links ]
2. Peden M, Oyegbite K, Ozanne-Smith J, et al., editors. World Report on Child Injury Prevention. Geneva: World Health Organization; 2008. PMID: 26269872 (accessed 15 February 2021). [ Links ]
3. Veale DJH, Wium CA, Müller GJ. Toxicovigilance I: A survey of acute poisonings in South Africa based on Tygerberg Poison Information Centre data. S Afr Med J 2013;103(5):293-297. https://doi.org/10.7196/SAMJ.6647 [ Links ]
4. Nixon J, Spinks A, Turner C, et al. Community based programs to prevent poisoning in children 0-15 years. Inj Prev 2004;10(1):43-46. https://doi.org/10.1136/ip.2003.003822 [ Links ]
5. Coker M, Folayan MO, Michelow IC, Oladokun RE, Torbunde N, Sam-Agudu NA. Things must not fall apart: The ripple effects of the COVID-19 pandemic on children in sub-Saharan Africa. Pediatr Res 2020 Sep 24. https://doi.org/10.1038/s41390-020-01174-y.3 [ Links ]
6. Republic of South Africa. Disaster Management Act, 2002. Declaration of a National State of Disaster. Government Gazette No. 43096:313. 15 March 2020. https://www.gov.za/sites/default/files/gcis_document/202003/43096gon313.pdf (accessed 1 March 2021). [ Links ]
7. Roberton T, Carter ED, Chou VB, et al. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob Health 2020;8(7):E901-E908. https://doi.org/10.1016/S2214-109X(20)30229-1 [ Links ]
8. Dayasiri MBKC, Jayamanne SF, Jayasinghe CY. Risk factors for acute unintentional poisoning among children aged 1-5 years in the rural community of Sri Lanka. Int J Pediatr 2017;1-9. https://doi.org/10.1155/2017/4375987 [ Links ]
9. Chang A, Schnall AH, Law R, et al. Cleaning and disinfectant chemical exposures and temporal associations with COVID-19 - National Poison Data System, United States, January 1, 2020-March 31, 2020. MMWR Morb Mortal Wkly Rep 2020;69(16):496-498. https://doi.org/10.15585/mmwr.mm6916e1 [ Links ]
10. Jensen C, McKerrow NH. Child health services during a COVID-19 outbreak in KwaZulu-Natal Province, South Africa. S Afr Med J 2020;111(2):13185. https://doi.org/10.7196/SAMJ.2021.v111i2.15243 [ Links ]
11. Berta GN, Di Scipio F, Bosetti FM, et al. Childhood acute poisoning in the Italian North-West area: A six-year retrospective study. Ital J Pediatr 2020;46(1):1-9. https://doi.org/10.1186/s13052-020-00845-0 [ Links ]
12. Özdemir R, Bayrakci B, Tekşam Ö, et al. Thirty-three-year experience on childhood poisoning. Turk J Pediatr 2012;54(3):251-259. PMID: 23094535 (accessed 17 March 2021). [ Links ]
13. Ram P, Kanchan T, Unnikrishnan B. Pattern of acute poisonings in children below 15 years - A study from Mangalore, South India. J Forensic Leg Med 2014;25:26-29. https://doi.org/10.1016/j.jflm.2014.04.001 [ Links ]
14. Balme KH, Roberts JC, Glasstone M, et al. The changing trends of childhood poisoning at a tertiary children's hospital in South Africa. S Afr Med J 2012;102(3 Pt 1):142-146. https://doi.org/10.7196/samj.5149 [ Links ]
15. Street RA, Kabera GM, Connolly C. Ethnopharmacological use of potassium permanganate in South African traditional medicine. S Afr Med J 2018;108(3):187-189. https://doi.org/10.7196/SAMJ.2018.v108i3.12606 [ Links ]
16. Johnson TB, Cassidy DD. Unintentional ingestion of potassium permanganate. Pediatr Emerg Care 2004;20(3):185-187. https://doi.org/10.1097/01.pec.0000117926.65522.33 [ Links ]
17. Centers for Disease Control and Prevention. The National Institute for Occupational Safety and Health. Workplace Safety and Health Topics: Organic Solvents. https://www.cdc.gov/niosh/topics/organsolv/#ValueCurrentcriteria (accessed 11 June 2021). [ Links ]
18. Schmertmann M, Williamson A, Black D. Unintentional poisoning in young children: Does developmental stage predict the type of substance accessed and ingested? Child Care Health Dev 2014;40(1):50-59. https://doi.org/10.1111/j.1365-2214.2012.01424.x [ Links ]
19. Glenn L. Pick your poison: What's new in poison control for the preschooler. J Pediatr Nurs 2015;30(2):395-401. https://doi.org/10.1016/j.pedn.2014.10.009 [ Links ]
20. Dowswell T, Towner EML, Simpson G, Jarvis SN. Preventing childhood unintentional injuries - what works? A literature review. Inj Prev 1996;2(2):140-149. https://doi.org/10.1136/ip.2.2.140 [ Links ]
 Correspondence:
Correspondence:
R Vosloo
drruanvosloo@icloud.com
Accepted 7 February 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}