










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.17 n.1 Pretoria 2023
http://dx.doi.org/10.7196/sajch.2023.v17i1.1958
RESEARCH
Asthma control among adolescents in the inner provinces of South Africa: Perception v. reality
A O Olajide-IbiejugbaI; V NkosiII, III, IV; F Rathogwa-TakalaniV; J ShirindeII; J WichmannII; R J GreenVI; K VoyiII
IMPH; School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria, South africa
IIPhD; School of Health Systems and Public Health, Faculty of Health Sciences, University of Pretoria, South africa
IIIPhD; Environment and Health Research Unit, South African Medical Research Council, Johannesburg, South Africa
IVPhD; Department of Environmental Health, Faculty of Health Sciences, University of Johannesburg, South Africa
VMSc; Department of Advanced Nursing Science, Faculty of Health Sciences, University of Venda, Thohoyandou, South Africa
VIPhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Pretoria and Steve Biko Academic Hospital, Pretoria, South Africa
ABSTRACT
Proper asthma control can lessen the negative effects of asthma in adolescents, such that they can lead a normal and physically active life. The study aimed to compare self-reported asthma control and actual test scores among adolescents in the inner provinces (Gauteng and North West) of South Africa. The asthma control test (ACT) questionnaire was administered to 123 of adolescents who had reported doctor-diagnosed asthma during the cross-sectional study. There was a statistically significant difference between self-reported asthma control and actual test scores among study participants (p=0.003). Out of the 90 study participants who claimed that their asthma was controlled, only 25 (27.78%) were correctly classified as 'controlled' according to the ACT. A high percentage (72.22%) of adolescents misclassified their asthma as 'controlled, whereas it was not. There is a lack of studies on asthma control in Africa.
Asthma is a common chronic non-communicable respiratory disease. In 2018, the disease affected the quality of life and longevity of >340 million people globally.[1] Most of those affected were children under 15 years of age who lived in urban areas in low- and middle-income countries (LMICs), such as South Africa (SA). The situation is worsening in LMICs in contrast to many high-income countries.
In 2018, 67% of people in SA lived in urban areas.[2] Many factors that influence asthma development, exacerbation and control are associated with urbanisation, e.g. poor air quality, poverty, lifestyle and dietary changes.[1]
Globally, more research is needed on the economic burden of asthma, as many challenges remain in estimating its prevalence, as well as its direct and indirect costs. Direct costs include consumable healthcare services and products, such as hospital services, doctor visits and medicines. Its indirect costs to society include loss of work productivity of caregivers. [1] In children, asthma contributes significantly to sleep disturbance which may lead to school absenteeism, limited play activities and parental or caregiver anxiety. Children who had asthma were reported to be 3.5 times more likely than those without asthma to drop out of school by the age of 16 with only basic education.[3] They were also twice as likely to drop out of university before completing 3 years of tertiary education. Hence, children who develop asthma have worse life outcomes regarding education and employment prospects as they enter adulthood. Proper asthma control can lessen these negative effects as patients can lead normal and physically active lives.
However, numerous factors contribute to poor asthma control, including poor adherence to medication, inappropriate inhaler technique and exposure to risk factors which trigger asthma attacks.[1] A study conducted from July to October 2012 in Johannesburg, SA, involving 115 asthmatic children (aged 5 - 18 years) reported that the main reason for poor asthma control was the lack of adherence to medications, whereas household living conditions did not have a significant influence.[5]
In the face of a paucity of studies in Africa, the present study aimed to contribute to the body of knowledge on asthma control as well as to compare self-reported asthma control and the actual test scores among adolescents in the inner provinces of SA. The study locations frequently experienced air pollution levels that exceeded the World Health Organization air quality guidelines.[6]
Methods
Population and study design
A cross-sectional study, employing the ISAAC Phase 2 questionnaire, was carried out between March 2015 and September 2016. Participants were 6 500 adolescents living and studying in communities situated near mine-tailing dumps in SA, with a response rate of 91.2%. A sub-sample of 123 adolescents with doctor-diagnosed asthma were included in the follow-up study.
Questionnaire administration
The asthma control test (ACT) questionnaire was administered to 123 of the participants who had reported doctor-diagnosed asthma during the cross-sectional study. Having doctor-diagnosed asthma was defined as an affirmative response to the question 'Were you diagnosed as being asthmatic by a doctor?' The ACT is a validated, self-administered, 5-item questionnaire that assesses the level of asthma control over a period of 4 weeks, with scores varying from 5 to 25. The higher the score, the better the level of asthma control. An ACT score between 20 and 25 suggests well-controlled asthma and a score <20 suggests poorly controlled asthma.[7] Consent was obtained from parents and the respective school authorities. Ethical approval was obtained from the Ethics Committee of the Faculty of Health Sciences, University of Pretoria (ref. no. 303/2014).
Statistical analyses
Data were entered into a database using EPI DATA and were analysed using STATA version 15.0 (SPSS Inc., USA). Descriptive statistics, such as frequencies and percentages, were used to summarise data as appropriate. A chi-squared test of association was used to determine the relationship between perception of asthma control and actual test scores of control among adolescents in the inner provinces of SA. A p-value <0.05 was deemed significant.
Results
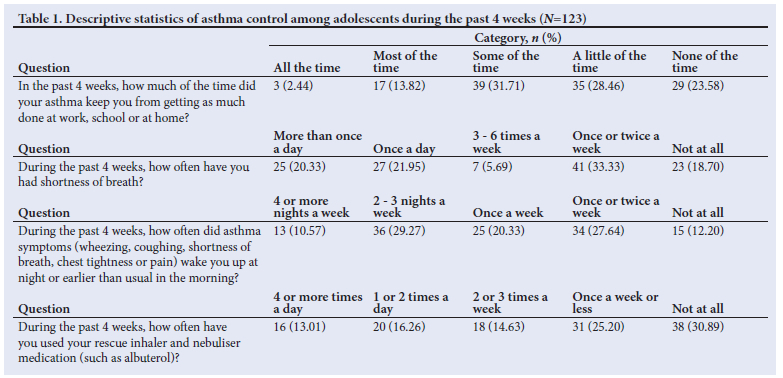
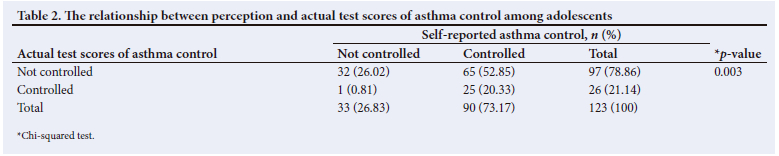
A total of 123 doctor-diagnosed participants was included in the study; 71 (57.72%) were female and 52 (42.28%) were male. Table 1 summarises the asthma control among adolescents during the last 4 weeks. The majority (n=94 (76.42%) of the adolescents reported that asthma had prevented them, to a certain extent, from doing their schoolwork and domestic chores during the past 4 weeks. Most participants (n=100; 33.30%) reported they had experienced shortness of breath, while 108 (n=87; 80%) had experienced asthma symptoms such as wheezing, coughing, shortness of breath and chest tightness or pain that disturbed their sleeping pattern during the past 4 weeks. Inhalers and nebuliser medications to relieve asthma were used by 85 (69.11%) of the participants during the past 4 weeks. Table 2 shows that there was a statistically significant difference between self-reported asthma control and actual test scores of controls among study participants. Out of 90 study participants who claimed their asthma was controlled, only 25 (27.78%) had correct classification as controlled according to the ACT. A high percentage (n=65; 72.22%) of misclassification was observed. A total of 32 (26.02%) participants was correctly classified as 'not controlled.
Discussion
The present study aimed to compare the self-reported control of asthma to the reality of asthma control based on actual test scores among adolescents in the inner provinces of SA. Ninety of the adolescents self-reported that their asthma was controlled; however, the ACT revealed that only 25 (27.78%) of the adolescents had controlled asthma. There was a high percentage (72.22%) of adolescents who misclassified their asthma as controlled, while they were in fact not controlled. Our results confirm that asthma was poorly controlled among adolescents. Uncontrolled asthma needs to be correctly identified, as it is a risk factor for asthma exacerbations, emergency room visits and hospital admissions, worsening lung disease and poor prognosis.[8] Factors leading to poor control of asthma are widely reported in the literature. These include lack of disease awareness, medication fears, affordability and access to asthma therapy, as well as stigma associated with taking asthma medication, i.e inhalers.[9] Other factors that lead to poor control reported in the literature are patients deliberately altering their doses to suit their own needs and forgetting to take medication as prescribed.[10] Some of the reasons given by adolescents for poor asthma control include poor treatment adherence caused by being independent and wanting to take medication on their own and thereby missing doses owing to feelings of embarrassment associated with administering medication in the presence of friends.[11] Asthma patients are often reluctant to report adherence to medication which contributes further to misclassification. The dangers of poor asthma control include the risk of asthma exacerbations, especially in communities where there is a high exposure to air pollution. It is well known that exposure to air pollution triggers or exacerbates asthma.
Conclusion
There is a lack of studies on asthma control in Africa, especially among adolescents living in communities exposed to high levels of air pollution, which are frequently above the levels in the World Health Organization air quality guidelines. Therefore this report will serve as a baseline to assist health practitioners treating asthmatic adolescents in structuring health messages on asthma control in this population group.
Declaration. None.
Acknowledgements. The authors would like to thank everybody who participated in the study, all the fieldworkers who assisted in data collection, and the data technicians for data capturing.
Author contributions. AOOI, RJG and KV: study design, data collection, statistical analysis, interpretation of results, drafted and critically revised manuscript. VN, FTR, JS and JW: statistical analysis and interpretation of results, drafted and critically revised the manuscript.
Funding. The study was funded by the Mine Health Safety Council of South Africa (grant no. SIM 100801).
Conflicts of interest. None.
References
1. The Global Asthma Network. The Global Asthma Report 2018. Auckland: GAN, 2018. http://globalasthmareport.org/ (accessed 23 November 2021). [ Links ]
2. The World Bank Group. World Urbanisation Prospects: 2018 Revision. https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS?name_desc=true (accessed 23 November 2021). [ Links ]
3. Schyllert C, Andersson M, Backman H, Lindberg A, Rönmark E, Hedman L. Childhood onset asthma is associated with lower educational level in young adults - a prospective cohort study. Respir Med 2021;186(1):106514. https://doi.org/10.1016/j.rmed.2021.106514 [ Links ]
4. Garba BI, Ballot DE, White DA. Home circumstances and asthma control in Johannesburg children. Curr Allergy Clin Immunol 2014;27(3):182-189. https://journals.co.za/doi/pdf/10.10520/EJC157482. [ Links ]
5. World Health Organization. 2021. Air Quality Guidelines - Update 2021. Copenhagen, Denmark: WHO Regional Office for Europe. https://apps.who.int/iris/handle/10665/345329. (accessed 23 November 2021) [ Links ]
6. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: A survey for assessing asthma control. J Allergy Clin Immunol 2004;113(1):59-65. https://doi.org/10.1016/j.jaci.2003.09.008 [ Links ]
7. Licari A, Marseglia G, Tosca MA, Ciprandi G. Asthma control in children and adolescents: A study in clinical practice. J Asthma 2020;57(6):645-647. https://doi.org/10.1080/02770903.2019.1594889 [ Links ]
8. Braido F, Chrystyn H, Baiardini I, et al. 'Trying, but failing' - the role of inhaler technique and mode of delivery in respiratory medication adherence. J Allergy Clin Immunol 2016;4(5):823-832. https://doi.org/10.1016/j.jaip.2016.03.002 [ Links ]
9. Burgess S, Sly P, Devadason S. Adherence with preventive medication in childhood asthma. Pulm Med 2011;2011:1-6. https://doi.org/10.1155/2011/973849 [ Links ]
10. Kaplan A, Price D. Treatment adherence in adolescents with asthma. J Asthma Allergy 2020;14(13):39-49. https://doi.org/10.2147/JAA.S233268 [ Links ]
 Correspondence:
Correspondence:
V Nkosi
vusi.nkosi@mrc.ac.za
Accepted 31 January 2022


{kind=link}
{kind=link}