










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.16 n.3 Pretoria Sep. 2022
http://dx.doi.org/10.7196/SAJCH.2022.v16i3.1883
RESEARCH ARTICLE
Perceptions of healthy food, and perceived facilitators and barriers to buying and consuming healthy food, among female caregivers in Soweto, South Africa
D BesselinkI; H BrandtII; S KlingbergIII; C E DraperIII
IMMedSci; Department of Health Science, Faculty of Science, VU University of Amsterdam, The Netherlands
IIPhD; Department of Health Science, Faculty of Science, VU University of Amsterdam, The Netherlands
IIIPhD; SAMRC Developmental Pathways for Health Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Obesity poses a continuous health challenge in South Africa and disproportionately affects black African households. To target obesity in these settings, it is crucial to have an in-depth understanding of food choices made by affected households.
OBJECTIVES. To explore how healthy food is perceived by women living in Soweto, and the facilitators of and barriers to buying and consuming this food.
METHODS. This was a qualitative study that utilised semi-structured interviews. Ten participants were recruited using purposive sampling. Interviews were audio-recorded, transcribed verbatim and analysed using thematic analysis. The study took place in Soweto, South Africa, and was conducted from February to May 2019.
RESULTS. Six themes were developed from the data: perceptions of healthy food; protecting family members from unhealthy food; learning about healthy food; appreciation by the family; home-cooked food v. food bought on the street; and budgetary restrictions. The first three themes were grouped by the overarching theme 'consciousness of healthfulness of food', and the last three themes were grouped by the theme 'influences of the family and environment on food choices'.
CONCLUSIONS. A focus on the whole family's dietary behaviours is recommended and, in future interventions, guidance communicated in intervention materials should be tailored to existing knowledge of healthy eating.
When obesity was first recognised as an emerging health problem, it was considered a condition existing in high-income countries. Today, two-thirds of obese people live in low- and middle-income countries (LMICs).[1,2] This is because many LMICs are experiencing changes in both physical activity patterns and dietary behaviour, such as increased use of motorised transport, more sedentary leisure time activities and increased consumption of processed food.[3-Processed food is typically energy-dense food containing refined carbohydrates, added sugars, fats and animal-sourced food; these foods are all associated with overweight and obesity.[1]
A country where diets are increasingly characterised by energy-dense food is South Africa (SA). Between 2005 and 2010, sales of processed food, such as packed snacks and ready-made meals, rose by 40%.[4] Moreover, a study from 2012 indicates that the most desired food among young adults comprised fast food, cookies, sweets and sugar-sweetened beverages.[5] As diets are becoming more energy-dense, the number of people with obesity and non-communicable diseases (NCDs) in SA is rising.[6,7] Furthermore, as the affordability of food is a pivotal factor when choosing what to eat, the consumption of diets high in energy-dense food is more common in low-income areas in SA.[2,5,8,9] A specific population group disproportionately affected by obesity and poverty in the country are black African women. Compared with 31% of South African men, 68% of women above the age of 15 years in SA were classified as overweight or obese in 2016.[10 Besides, within black African households affected by poverty, 63.4% were female headed.[2,11]
As the home environment is highly influential in the progress of obesity, home-based interventions are a common method to target obesity-related behaviours.[12] Therefore, in order to make home-based interventions successful, it is crucial to have in-depth understanding of the specific context in which the intervention will be implemented.[13] However, little is known about the motives behind food choices when considering the healthfulness of food in low-income households in South Africa, particularly in relation to the healthy eating habits of young children. Given the importance of establishing healthy eating behaviours early in life, the aim of this study was to explore female caregivers' perceptions of healthy food, and their perceived facilitators and barriers to buying and consuming this food.
Methods
Study design
This study was an exploratory qualitative study which aimed to provide an in-depth understanding of female caregivers' perceptions of healthy food in an urban township, with a focus on female caregivers of 3 - 5-year-old children. Individual semi-structured interviews were utilised to allow participants to elaborate on their experiences and feelings about healthy food.[14]
Ethics
Ethical approval was obtained from the University of the Witwatersrand's Human Research Ethics Committee (Medical; M181063). All participants gave informed written consent for participation.
Participant recruitment
The study took place in Soweto, an urban township located in Johannesburg, South Africa. Inclusion criteria were: (i) being a female caregiver of a child between approximately 3 and 5 years old, (ii) living in Soweto, (in) minimum age of 18 years, and (iv) the willingness and ability to be interviewed in English.
Prior to conducting the study, a household survey was conducted in Soweto by the University of the Witwatersrand. This study provided a list of individuals who had consented to be re-contacted for future studies. The initial contact with potential participants was made telephonically by the first author. During the phone call, the purpose of the study was explained, and fulfilment of inclusion criteria was ascertained. If an interviewee agreed to participate, a time and location were agreed upon for an interview. A total of 10 participants were recruited.
Instruments
An interview guide was developed based on existing literature regarding factors influencing food choices and perceptions of healthy food. Two conceptual frameworks were drawn on to guide the scope of the interview questions. The first framework was the Attitude, Social Influence and Self-Efficacy model, which posits that health behaviours depend on a person's intention to perform this behaviour, and it was used to capture personal factors influencing food choices.'151 The second framework, the Socio-Ecological Model (SEM), emphasises the complex societal aspects that influence health choices, and it was used to capture the external factors influencing food choices.'16,171 After a pilot interview and throughout the interview process, questions were added and removed, and adaptions were made to make the questions easier to understand for participants.
Procedures
Interviews took place between March and April 2019, with translation assistance from a local research assistant where necessary. After each interview, the course of the interviews and interpretation of answers of the participants were discussed between the researcher and research assistant. All interviews took place in participants' homes. Nine interviews were audio-recorded, and the responses of one participant who declined audio-recording were captured by taking notes. The durations of the interviews conducted varied from 30 minutes to 1 hour. All participants were compensated for their time (at the end of the interview) with a supermarket voucher (value approximately $7US.
Data analysis
The interviews were transcribed verbatim and anonymised. Data analysis was done using an inductive thematic analysis with support of Atlas.ti 8 software.[18] While data collection was still ongoing, the first interviews were transcribed and coded.'141 The codes formed conceptual labels that enabled the categorisation of data. Throughout data collection, the range of codes was expanded. To improve the robustness of the analysis process, codes were discussed within the research team. When all interviews were completed, all transcripts were read again, and codes were refined where needed. Broader relationships between the codes and the research question were then sought. In this way, new connections and overarching themes were created and reported patterns in the data were generalised, creating thematised meanings of the collected data.[14]
Results
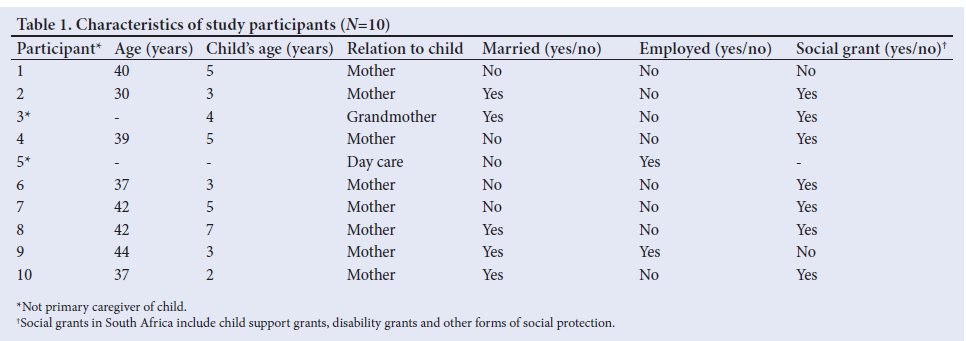
Six themes were developed from the data: perceptions of healthy food; protecting family members from unhealthy food; learning about healthy food; appreciation by the family; home-cooked food v. food bought on the street; and budgetary restrictions. The first three themes were grouped by the overarching theme 'consciousness of healthfulness of food, which captured the perceptions of healthy food, and the willingness to consume healthy food. The last three themes were grouped by the theme 'influences of the family and environment on food choices', which captured the facilitators and barriers to consuming and buying the food perceived as healthy food. In Table 1, participants' specific characteristics are presented.
Consciousness of healthfulness of food
Perceptions about healthy food
There was reportedly a clear understanding among participants that healthy food consists of vegetables and food low in oil, sugar and salt (Table 2: Quote 1 and 2). One participant in particular frequently consumed vegetables, and found it very important for her family to do the same. According to her, the high consumption of vegetables ensured that her family members did not get sick (Table 2: Quote 2). However, most participants were of the opinion that they did not consume enough vegetables, and expressed that they wanted to consume vegetables more frequently (Table 2: Quote 3).
Protecting family members from unhealthy food
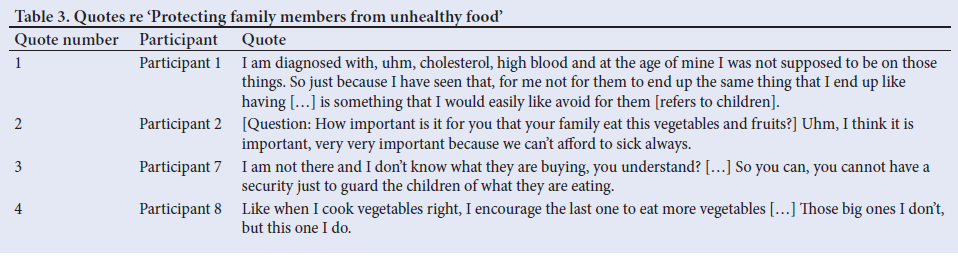
All participants had an experience of chronic disease - either themselves, or through a family member being chronically ill. Participants were highly aware of the possible consequences of an unhealthy diet, and this motivated most participants to control their families' consumption of unhealthy food. Especially when considering their children, participants tried to promote healthy eating behaviours and avoid the consumption of sweets. Participants' motivations to protect their children against unhealthy food differed; some believed that when their children were familiarised with healthy food at a young age, it would prevent them from becoming chronically ill later in life (Table 3: Quote 1). One participant had a more practical reason to promote the consumption of healthy food in her family. According to her, the consumption of fruit and vegetables was necessary to prevent her family from falling ill because she was afraid of the extra costs that they might have to incur (Table 3: Quote 2).
Most participants also acknowledged that it was difficult to stop their children from eating unhealthy food because they could not control what their children ate when they were not present (Table 3: Quote 3). A way for most participants to make sure that their children ate the food that they gave them was to dish up for them and not give them any choice but to eat the food. One participant mentioned that her youngest child was the only child she could still control in eating healthy food, and therefore she focused more of her energy on the younger child (Table 3: Quote 4).
Learning about healthy food
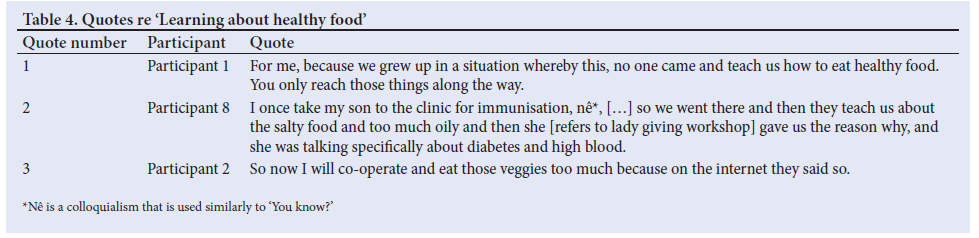
Some participants explained that receiving education about healthy food and the benefits of healthy food motivated them to consume healthier diets. However, the education that led to this motivation was usually gained later in life, and not during school (Table 4: Quote 1). Many participants mentioned the nearby health clinic as a source where they received education about healthy food (Table 4: Quote 2). In addition, social media, the internet and TV were also often mentioned as having taught participants about the benefits of healthy food (Table 5: Quote 3).
Influences of the family and environment on food choices
Appreciation by the family
Most participants bore the main responsibility for cooking within the household. The decision about what was going to be cooked for the day was highly influenced by the preferences of their family members (Table 5, Quote 1). Family members' favourite meals typically consisted of a starch and a meat. Participants who lived with a man explained that meat was the food that men appreciated the most. One participant explained this to be because the consumption of meat was part of South African culture (Table 5: Quote 2). Participants explained that starches were highly desired because these gave them and their family members the feeling of being full the whole day (Table 5: Quote 3).
Even though most participants cooked according to the wishes of their family members, they also acknowledged that they perceived the food that their family members preferred as unhealthy. For example, some believed that starchy foods could lead to constipation and weight gain, and the consumption of too much meat was often mentioned as a risk factor for developing gout. In their opinion, the need to cook the food that their family members appreciated the most felt like a barrier towards the consumption of a healthier diet for themselves and their family members (Table 5: Quote 4).
Home-cooked food v. food bought on the street
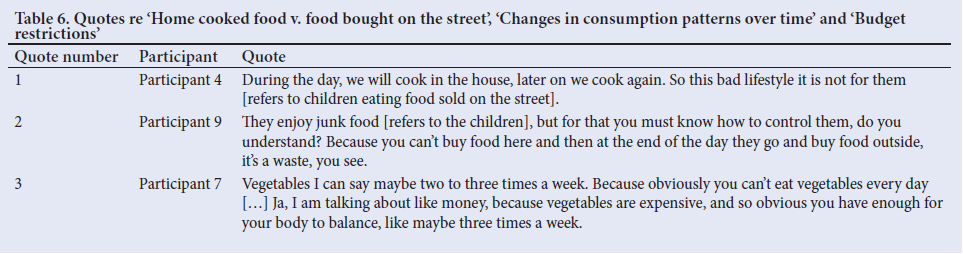
Most participants preferred their family members to eat food cooked at home rather than food sold on the street - also referred to as junk food. Participants thought of such food as unhealthy because it tends to be high in fat and low in vegetables (Table 6: Quote 1). However, most participants were aware that junk food was appealing to many, especially their children. One participant explained that the consumption of junk food by her children was wasteful because she would already have bought food to be cooked at home. Preventing this waste was an extra motivation for her to control her children's consumption of junk food (Table 6: Quote 2).
Budgetary restrictions
All participants explained that having a restricted budget was a major barrier to buying and consuming healthy food. They explained that rather than purchasing the food that they perceived as healthy, they would buy cheaper options or special deals. These cheaper options and deals were often considered as less healthy; for example, fish oil rather than olive oil. Almost all participants perceived the high cost of vegetables as a barrier to buying vegetables because they had to compromise on the amount of vegetables that they consumed during the week (Table 6: Quote 3).
Discussion
The present study highlighted the perceptions of female caregivers of young children living in Soweto regarding healthy food, and what they perceived to be facilitators and barriers to buying and consuming healthy food. The main findings were that vegetables and food low in oil, sugar and salt were perceived as healthy by participants. Participants who encountered chronic illness, either themselves or within their families, perceived this awareness as a facilitator to buying and consuming healthy food. Family members' preferences for unhealthy food and purchasing food on a restricted budget were barriers to buying and consuming healthy food.
Study participants were highly aware of the consequences of unhealthy food, and they explained this awareness as the reason why they desired to consume a healthier diet. This stance was in contrast to a previous study conducted in SA, which showed that most participants did not associate poor eating habits with chronic diseases and did not think of being overweight as something that impaired their health.[19] Factors that led to this awareness which were mentioned by participants in the current study were receiving education about healthy food and experiencing health issues due to the consumption of unhealthy food.
Budget restrictions were a major barrier to buying healthy food. This finding is not surprising, as it is well established that a lower income shapes food behaviour towards the consumption of unhealthier diets.[20] Additionally, the costs of healthy food in South Africa are rising, and widening the gap between what foods poor households can afford and what they should be buying for basic nutrition.[21] On the other hand, a study conducted in Durban, South Africa, showed that even if the household income of participants had increased substantially over the years, the price of food was still a significant concern for these participants. Always on a search for the best deals, participants of the Durban study tried to save as much money as possible on food.[22] This point suggests that in the current study, prioritising low-priced food may have been the main barrier towards buying healthy food, rather than the absolute cost of vegetables as experienced by participants.
The analysis presented here shows a contradiction between the desire of most participants for their family members to consume healthier food, and the food that they cook for themselves and their family members. When deciding what to cook, the preferences of family members were very influential, and especially male preferences took precedence. Nevertheless, the food preferred most was also perceived as unhealthy when consumed too often, and prevented participants from cooking more healthy food for their families. A study conducted with families in the United States showed the same contradiction: mothers wanted to make healthy food choices, but fathers desired the less healthy options more, with adolescents in these families leaning more towards the diet habits of their fathers.[23] A reason why male preferences in the current study took precedence could be because of prevailing patriarchal norms in South Africa.[24]
The current study clearly shows the desire of study participants to promote healthy food choices for their children. However, it also suggests that when children are not supervised by their caregivers, there is no control over what they consume. A strategy of participants in the current study to gain more control over the food that their children ate, was to motivate their children to eat home-cooked food rather than junk food bought on the street. This strategy was shown to be successful in improving childhood obesity in other studies as well.[26,27] By emphasising home-cooked meals and family dinners, children are taught to adopt healthier diets at an early age.
The findings of the current study can inform home-based health interventions addressing food behaviours. Firstly, it could be beneficial for such interventions to include the whole family rather than only one person, considering the effect that family members had on the food choices of participants. Secondly, the current study showed that participants already had a broad knowledge about healthy food. By building upon this knowledge rather than repeating facts that participants already knew, home-based health interventions addressing food choices could potentially be more effective. Because many of the participants mentioned the local health clinic to be a source where they learned about healthy eating, guidance on healthy eating could be provided by community healthworkers operating from local health clinics. However, future research is needed to explore the feasibility and effects of this suggested method, whether the material provided is easy to understand by caregivers, and to obtain further insights into why existing guidelines (e.g. South African food-based dietary guidelines) are not necessarily implemented. Lastly, future research could explore the financial constraints to buying healthy food described by participants, as the analysis here suggests a complex balance between affordability and priorities of budget allocation.
It is important to recognise that the factors hindering the consumption of healthy food were highly embedded in the cultural and environmental factors ofparticipants' surroundings. For example, budget restrictions experienced by participants are determined by their socio-economic status. Furthermore, the possible patriarchal norms that pose a barrier towards the consumption of more healthy food in the families of participants, are deeply embedded in their social and cultural norms and values.[7,20] In order to improve these factors, systematic and long-term changes that are not being addressed by home-based interventions need to occur.
Limitations of the study included the potential for socially desirable answers, the potential misinterpretations owing to translation and cultural differences, and a relatively small sample size. Nevertheless, as the aim of the current research was to capture perceptions of food rather than measure food intake of participants, potential socially desirable answers were not perceived to have a substantial effect on the study's results. The relatively small sample size could be perceived as a limitation, and may raise questions regarding data saturation. However, the utility and compatibility of saturation with thematic analysis has been questioned, and there is no definitive measure of data saturation.[26] Instead, this study was more concerned with the richness of data, and the number of interviews was determined by pragmatic and analytical considerations of how well the aims of the study could be fulfilled with the data collected. The strengths of the study lay in the continuous discussion of interpretations between the researcher and research assistant to help ensure the credibility of the findings. Besides, interviewing participants in their home environment helped the researcher to understand participants' contexts.
Conclusion
This study has built upon the understanding of food choices made in a low-income setting in SA. Even though participants found it important for themselves and their families to consume healthy diets, they faced several barriers that prevented them from doing so. By addressing these barriers, future home-based health interventions can become more successful in targeting malnutrition in low-income settings.
Declaration. None.
Acknowledgements.The authors wish to thank the participants for taking part in this study.
Author contributions. DB, SK and CED conceptualised the study; all authors provided input on the methodology. DB collected and analysed the data, with input from co-authors. DS drafted the manuscript, and all co-authors edited the manuscript and approved the final version.
Funding. None.
Conflicts of interest. None.
References
1. Zobel EH, Hansen TW, Rossing P, von Scholten BJ. Global changes in food supply and the obesity epidemic. Curr Obes Rep 2016;5(4):449-455. https://doi.org/10.1007/s13679-016-0233-8 [ Links ]
2. Caraher M, Coveney J. Food poverty and insecurity: International food inequalities. Cham: Springer, 2016. [ Links ]
3. Popkin BM. The nutrition transition and obesity in the developing world. J Nutr 2001;131(3):871s-873s. https://doi.org/10.1093/jn/131.3.871s [ Links ]
4. Steyn N, Labadarios DMB. Street foods and fast foods: How much do South Africans of different ethnic groups consume? Ethnicity Dis 2011;21:462-466. [ Links ]
5. Igumbor EU, Sanders D, Puoane TR, et al. 'Big Food, the consumer food environment, health, and the policy response in South Africa. PLOS Med 2012;9(7):e1001253. https://doi.org/10.1371%2Fjournal.pmed.1001253 [ Links ]
6. Steyn NP, McHiza ZJ. Obesity and the nutrition transition in Sub-Saharan Africa. Ann N Y Acad Sci 2014;1311:88-101. https://doi.org/10.1111/nyas.12433 [ Links ]
7. Wrottesley SV, Pisa PT, Norris SA. The influence of maternal dietary patterns on body mass index and gestational weight gain in urban black South African women. Nutrients 2017;9(7):732-746. https://doi.org/10.3390/nu9070732 [ Links ]
8. Temple NJ, Steyn NP. The cost of a healthy diet: A South African perspective. Nutrition 2011;27(5):505-508. https://doi.org/10.1016/j.nut.2010.09.005 [ Links ]
9. Kern DM, Auchincloss AH, Stehr MF, et al. Neighborhood price of healthier food relative to unhealthy food and its association with type 2 diabetes and insulin resistance: The multi-ethnic study of atherosclerosis. Prev Med 2018;106:122-129. https://doi.org/10.1016/j.ypmed.2017.10.029 [ Links ]
10. National Department of Health. South Africa Demographic and Health Survey, Key Indicator Report. https://www.statssa.gov.za/publications/Report%2003-00-09/Report%2003-00-092016.pdf; 2016. [ Links ]
11. The World Bank. Overcoming poverty and inequality in South Africa, an assessment of drivers, constraints and opportunities. Washington, DC: World Bank Group; 2018. [ Links ]
12. Knowlden AP, Sharma M. Systematic review of family and home-based interventions targeting paediatric overweight and obesity. Obesity Rev 2012;13(6):499-508. https://doi.org/10.1111/j.1467-789x.2011.00976.x [ Links ]
13. Klingberg S, Draper CE, Micklesfield LK, Benjamin-Neelon SE, van Sluijs EMF. Childhood obesity prevention in Africa: A systematic review of intervention effectiveness and implementation. Int J Environ Res Public Health 2019;16(7):1212-1230. https://doi.org/10.3390/ijerph16071212 [ Links ]
14. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychology 2006;3(2):77-101. [ Links ]
15. Verstraeten R, Van Royen K, Ochoa-Aviles A, et al. A conceptual framework for healthy eating behavior in Ecuadorian adolescents: A qualitative study. PLoS One 2014;9(1):e87183. https://doi.org/10.1371/journal.pone.0087183 [ Links ]
16. Robinson T. Applying the socio-ecological model to improving fruit and vegetable intake among low-income African Americans. J Community Health 2008;33(6):395-406. https://doi.org/10.1007/s10900-008-9109-5 [ Links ]
17. Drew S, Lavy C, Gooberman-Hill R. What factors affect patient access and engagement with clubfoot treatment in low- and middle-income countries? Meta-synthesis of existing qualitative studies using a social ecological model. Trop Med Int Health 2016;21(5):570-589. https://doi.org/10.1111/tmi.12684 [ Links ]
18. Atlas.ti, 8. Scientific Software Development GmbH. Berlin. [ Links ]
19. Okop KJ, Mukumbang FC, Mathole T, Levitt N, Puoane T. Perceptions of body size, obesity threat and the willingness to lose weight among black South African adults: A qualitative study. BMC Public Health 2016;16:365-378. https://doi.org/10.1186/s12889-016-3028-7 [ Links ]
20. Faber M, Wenhold FA, Laurie SM. Dietary diversity and vegetable and fruit consumption of households in a resource-poor peri-urban South African communitydiffer by food securitystatus. Ecol Food Nutr 2017;56(1):62-80. https://doi.org/10.1080/03670244.2016.1261024 [ Links ]
21. PACSA. PACSA Monthly Food Price Barometer: March 2016. South Africa: Information Exchange DataHub (accessed 4 June 2021). https://cloud.csiss.gmu.edu/uddi/fa_IR/dataset/food-prices-in-south-africa/resource/ccf5c9f3-4768-4782-afca-32e72b129e3b [ Links ]
22. Chevalier S. Food, malls and the politics of consumption: South Africa's new middle class. Food Culture Soc 2015;19(1):151-170. [ Links ]
23. Fielding-Singh P. Dining with dad: Fathers' influences on family food practices. Appetite 2017;117:98-108. [ Links ]
24. Thobejane TD, Florence SB. Exploring gender division of labour within households : A case of Schoemansdal Village, Nkomazi local municipality, Mpumalanga Province, South Africa. AFRIKA J Politics Econo Soc 2018;8(2):67-80. [ Links ]
25. Rogers CA. Simple suppers: Findings from a family meals childhood obesity prevention intervention. Ohio State University: Columbus; 2017. [ Links ]
26. Reicks M, Banna J, Cluskey M, et al. Influence of parenting practices on eating behaviors of early adolescents during independent eating occasions: Implications for obesity prevention. Nutrients 2015;7(10):8783-8801. https://doi.org/10.3390/nu7105431 [ Links ]
27. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exercise Health 2021;13(2):201-216. https://doi.org/10.1080/2159676X.2019.1704846 [ Links ]
 Correspondence:
Correspondence:
D Besselink
djoekebesselink@outlook.com
Accepted 22 July 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}