










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.16 n.3 Pretoria Sep. 2022
http://dx.doi.org/10.7196/SAJCH.2022.v16i3.1826
RESEARCH ARTICLE
Clinical evaluation and outcomes in children < 10 years old involved in road traffic accidents, presenting to Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
J-A CarreiraI; D KrugerII; J LovelandIII
IFCS (SA) ; Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; Research and Laboratories, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIICert Paed Surg (SA); Division of Paediatric Surgery, Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Road traffic accidents (RTAs) are a leading cause of injury and death globally, particularly among children. Pedestrians are most often injured, especially in middle- and low-income countries. The epidemiology, patterns and severity of injuries in children involved in RTAs in our community are hard to obtain.
OBJECTIVES. To evaluate the aetiological spectrum, injury characteristics and treatment outcomes of paediatric patients involved in RTAs, who presented to Chris Hani Baragwanath Academic Hospital (CHBAH), a tertiary hospital in Soweto, South Africa.
METHODS. Patients <10 years old, who were involved in RTAs and seen at CHBAH, were included in the study.
RESULTS. The study was conducted from 20 August 2017 to 31 March 2018, and included the data of 156 patients. Their ages ranged from 13 days to 10 years (65% were boys). Pedestrian vehicle accidents accounted for 78.8% of the injuries, with 60.8% of the children being unaccompanied by an adult. Motor vehicle accidents accounted for 19.2% of the injuries, with 92% of the children being unrestrained in the vehicle. Of the patients, 73.2% (n=112/153) underwent radiography and 44.4% required computed tomography (CT) scans, the majority being CT scans of the brain for suspected head injuries. Soft-tissue injuries accounted for 78.9% of cases, followed mainly by head (39.7%) and limb (16%) injuries. Only 12% of patients required surgical intervention, with 42% of the operations being for orthopaedic injuries.
CONCLUSION. The abovementioned data demonstrate that there is a lack of use of child restraints for children travelling as passengers in vehicles, and inadequate supervision of children on and around roads. This study supports other evidence, as it suggests that the paediatric population involved in RTAs is largely injured as pedestrians, and that males tend to be involved in more RTAs than females. The majority of injuries sustained involved the soft tissues, followed by head injuries.
Road traffic accidents (RTAs) are a major and increasing cause of death, injury and hospitalisation worldwide. According to the World Health Organization (WHO), ~1.35 million people die each year as a result of RTAs and >90% of these deaths occur in low- and middle-income countries of the African and eastern Mediterranean regions. WHO data for 2018 showed that RTA fatalities in South Africa (SA) reached 14 507 for 2016.[1]
The South African Medical Research Council found that in 2000, RTAs were the 9th leading cause of death in children <5 years of age in SA and the leading cause of death for children between the ages of 5 and 14 years - twice the global rate for that year.[2] However, there are few statistics regarding non-fatal injuries in children involved in RTAs.
In an international study of 11 countries investigating patterns of injury in children, Peclet et al.[3] identified trauma as the leading cause of death for children >1 year of age. Injuries sustained by motor vehicle accident (MVA) occupants and pedestrians account for the greatest number of these trauma deaths and continue to be a leading cause of death and disability in children.[3]
A retrospective study by Pretorius and Firth[4] documented admissions to the paediatric orthopaedic ward at Chris Hani Baragwanath Academic Hospital (CHBAH) over a 3-year period and showed that 13.4% of the total admissions of children <14 years of age were due to RTAs. Patients between the ages of 4 and 8 years had the highest frequency of injuries sustained in RTAs. In contrast, a study from the UK found that RTAs accounted for only 7% of paediatric fractures - half the incidence reported in the Soweto population.[4]
The WHO reported that 11% of all road-related injuries in children occur on public roads and can result in a fatality or a significant life-changing injury. They showed that head injuries comprised 23% of all transport-related injuries in children, which can result in long-term disability, placing a large burden on the child's family and community. In low- and middle-income countries, the proportion of children injured as pedestrians ranges between 30% and 40%.[5] Many studies showed that the majority of these injuries were sustained by boys.[2,4-10]
The exact epidemiology regarding RTA injuries in the SA paediatric population is unknown. There is a paucity of published data regarding the paediatric population in the local environment. Consequently, the statistics, patterns and severity of injuries, as well as the outcomes in children involved in RTAs, are hard to find.
This study therefore aimed to evaluate the injury characteristics and management of paediatric patients involved in RTAs in our local population. Statistics assist in gaining a better understanding of these preventable injuries in order to move forward with intervention strategies to curb the number of children injured on our roads.
The 'Promotion of a Childsafe South Africa' study[11] highlights that injury of children is a major public health problem and that there should be more focus on awareness and education of communities and parents regarding this 'neglected childhood killer disease.
Aim and objectives
The aim of this study was to evaluate the aetiological spectrum, injury characteristics, radiological investigations and treatment of paediatric patients involved in RTAs, who presented to a Gauteng tertiary hospital (CHBAH) in Soweto. The study objectives were:
• to determine the demographics and clinical characteristics of paediatric patients presenting to CHBAH after being involved in a road traffic-related accident
• to determine the mechanism and extent of the sustained injuries
• to report on the following outcomes:
• patient admission to a ward or intensive care unit (ICU)
• investigations that the child underwent
• patients who required surgery
• additional specialty consultation.
Methods
Patient selection
A prospective, descriptive, hospital-based study was conducted from 20 August 2017 to 31 March 2018 (7 months, 11 days). All patients <10 years old and who presented to the surgical emergency department at CHBAH after an RTA were included in the study. These patients were identified on arrival by a history of having been involved in a road accident.
Data acquisition
All data were collected on a data sheet in the form of a questionnaire, which was completed by doctors caring for the patients at various levels. Initially, the casualty doctor identified the patient as having been involved in an RTA and then referred them to a paediatric surgeon to assess and manage the child further. The paediatric surgeon subsequently completed the questionnaire. The information regarding some of the circumstances surrounding the accident was obtained from the caregiver of the child. The record review was anonymised to protect patient confidentiality. Each record was assigned a unique study number and no identifying data were included.
Statistical analyses
All identifiable patient data were coded and study data were recorded using a data collection sheet. The data were captured on a Microsoft Excel spreadsheet (Microsoft Corp., USA) and then imported into Stata analytical software (version 14.0) (StataCorp., USA). Descriptive statistics on continuous variables were reported as medians and interquartile ranges owing to the non-parametric nature of the data, whereas categorical data were reported as frequencies and proportions. The χ2 or Fisher's exact test and Mann-Whitney/Kruskal-Wallis tests were performed as appropriate, with _p<0.05 regarded as significant. Where significant, odds ratios and 95% confidence intervals were reported to determine effect size.
Ethical approval
Ethical approval was obtained from the University of the Witwatersrand Human Research Ethics Committee (Medical) (ref. no. M160451). Permission was obtained from the CHBAH clinical executive officer to conduct the research. Informed consent was obtained from the child's caregiver or parent as soon as they were available, according to the standards set out by legislation in SA and under the guidelines and standards of the ethics committee of the University of the Witwatersrand.
Results
A total of 156 patients were included in the study - their ages ranging from 13 days to 10 years (Table 1). The mean age (standard deviation (SD)) was 4.8 (2.5) years and 65% were male.
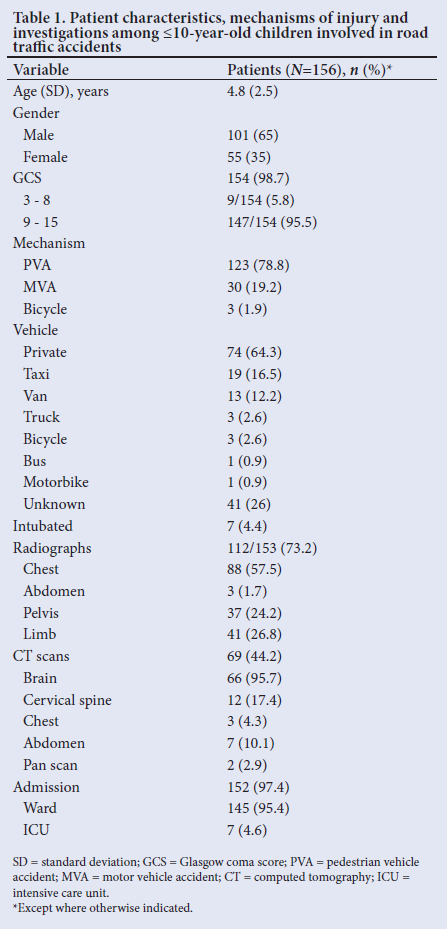
The majority of the study patients were involved in pedestrian vehicle accidents (PVAs) (78.8%), followed by MVAs (19.2%) and bicycle accidents (1.9%). RTAs mostly involved private vehicles for both MVAs and PVAs, with the remaining 16.5% being public transport, i.e. taxis.
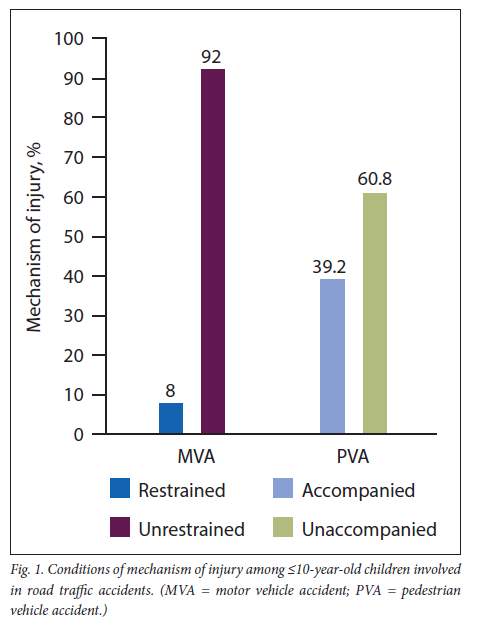
Alarmingly, 92% of children involved in MVAs were unrestrained and 60.8% of those involved in PVAs were unaccompanied by an adult at the time of the accident (Fig. 1). An adult was defined as a person aged >16 years.
The majority (73.2%) of the patients underwent radiography and 44.3% computed tomography (CT) scans (Table 1). Only 4.4% (n=7/156) of children required intubation and 75.8% presented with a Glasgow coma score (GCS) <9. The majority of study patients were admitted (97.4%), of whom 95.4% were admitted to the ward and 4.6% to the ICU.
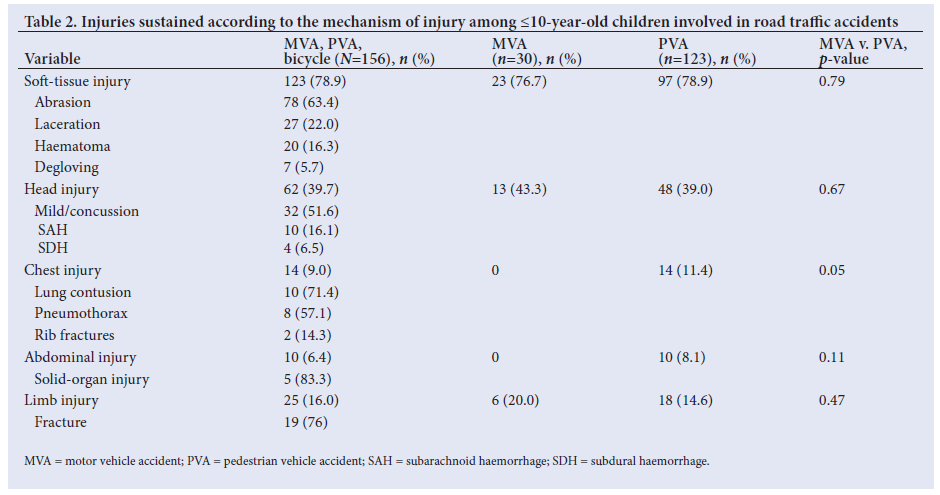
Table 2 shows the main admission diagnoses: soft-tissue injury - 78.9%, followed by head injury - 39.7%. The soft-tissue injuries were further classified into abrasions (66.1%), lacerations (22.9%), haematomas (16.9%) and degloving injuries (5.8%). Also, 8.5% of the patients had lacerations and abrasions. Chest injuries accounted for 9% (n=14), with diagnoses of rib fractures, lung contusions and pneumothoraces. Only 6.4% of study patients presented with abdominal injuries, with 1 child sustaining a bladder rupture. Of the 16% of patients with limb injuries, 76% had fractures. No statistically significant differences were seen between the injuries and the mechanism of injury, while none of the MVA patients had a chest or abdominal injury (Table 2; Fig. 2). In the PVA group we found that the rate of head injuries was significantly higher in those unaccompanied by an adult (44.4%) than in those who were accompanied (20.7%; £=0.037).
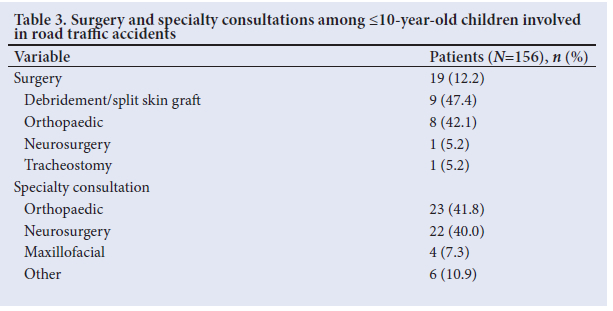
Only 12.2% of the patients required surgery, which included orthopaedic interventions (42.1%) and debridement or split skin graft (SSG) of wounds (47.4%) One patient underwent an intracranial procedure and 1 tracheostomy was performed (Table 3). Other specialists were consulted for 35.3% of the patients, with orthopaedic surgeons consulted most often (41.8%), followed closely by neurosurgeons (40.0%) and maxillofacial surgeons (7.3%). Only 2.5% of patients were discharged from casualty.
Discussion
In total, 60.8% of children in the current study who were involved in PVAs were not accompanied by a responsible person >16 years old. In the PVA group, we found that the rate of head injuries was significantly higher in children who were unaccompanied by an adult (44.4%) than in those who were accompanied (20.7%; p=0.037). These results are in line with other study outcomes: a Malaysian study'[21] found that parental supervision reduced the risk of children being injured in RTAs by 57% (n=15), and a study in Canada found that lack of parental supervision increased the risk of injury to child pedestrians and cyclists by a factor of 2.6.[13]
The abovementioned percentages raise many questions regarding the lack of supervision of young children on and around dangerous roads. One needs to ascertain the level of comprehension and understanding of traffic and road safety of a child aged ≤10 years. As mentioned in the study by Zeedyk et al.,[14] 'The cognitive processes involved in judgement, decision-making, reasoning and impulse control at that age are rudimentary, thus increasing the vulnerability of children in that age group in the road environment'. There is not a predetermined age at which a child can be said to be safe on and around roads and traffic. Young children are not able to comprehend and react to various traffic situations safely. They also have poor distance judgement and psychomotor abilities.[14] Hence, there should be supervision of such children when they are near roads and traffic, where an injury may occur. The mean age (SD) of unaccompanied children who were involved in PVAs, was 5.0 (2.4) years, while the mean age of accompanied children who were involved in PVAs was 4.3 (2.8) years.
The current study showed that of the children involved in MVAs, 92% were unrestrained in the vehicle. This percentage is higher than that shown in other comparable studies. A study in Singapore[7] showed a 63.3% unrestrained rate, whereas a study in the USA[15] showed that 2% of the children involved were unrestrained, although they also reported that a further 46% were inappropriately restrained. In our study, the mean age of unrestrained children in MVAs was 4.2 years.
According to the National Road Traffic Act, 2015, 'The driver of a motor vehicle operated on a public road shall ensure that an infant (0 - 3 years) travelling in such a motor vehicle is seated on an appropriate child restraint …'; however, this law does not apply to transportation of infants in a 'minibus, or bus operating for reward'.[16] The loophole here is that our communities' paediatric population use a local minibus/taxi as their main form of transportation.
The Act also states that children between the ages of 3 and 14 years (or <1.5 m tall) must be in a child restraint (car seat), if available, and that in the event of no car seat being available, the child should be strapped in with a seat belt. It goes on to say that '… if no seat belt is available and the vehicle is equipped with a rear seat, the driver must ensure that the child is seated in the rear seat'.[17]
There is a notable difference between the SA law and what is regarded as best practice worldwide. A safe child restraint needs to be based on the individual child's height, weight and age and cannot be categorised generally.[16] It has been shown that if correctly installed and correctly positioned and secured, car seats can reduce infant road accident deaths by 70%. These seats can reduce death rates of children aged 1 - 4 years by 54% and the incidence of significant injuries sustained by children aged 4 - 7 years by 59%.[18]
Snowdon et al.[19] performed a study in Canada that evaluated the effectiveness of booster seat legislation on restraint use in motor vehicles among children aged 4 - 8 years old. They found that in the provinces with legislation in place, 91.9% of children were restrained; conversely, in provinces without legislation, 84.4% of children were restrained, which may indicate that laws and enforcement of the legislation may contribute to better use of child restraints in motor vehicles.
Soweto is a large township with a population of ~1 271 628, according to Statistics South Africa at the time of the last census (2011). It is a low-income economic area, with a large proportion (~19%) of the population with no income, and only 3% of the township's total population earning >ZAR307 600 a year.[20] This may influence factors that may contribute to children walking unaccompanied and travelling unrestrained in vehicles in their local environment. These factors were not investigated in our study. Nevertheless, through our experience in this setting, we believe that lack of adult supervision and adherence to road safety laws may reflect lack of finance, education, awareness and law enforcement. These are some of the many variables that contribute to the high number of children being injured on and around the roads in Soweto.
In the local community where the study was conducted, parents are often already at work during the early hours of the morning and until late at night; children are therefore left to travel to and from school on their own. The majority of this population group travel by foot or require the use of public transport, which increases travelling time, as only 23.6% of households in Soweto own motor vehicles.[20] This is a major problem to which a solution is not easy to find.
There are various programmes being set up for road safety. Arrive Alive has 'Freddy, the safety character, to teach children about road safety. Also, a non-profit organisation, Childsafe, based in Cape Town, strives to create awareness and educate communities regarding child safety issues, including road safety, through events and campaigns. Some non-governmental organisations arrange the collection of used car seats that are in working condition to supply to those in need.
The majority of children involved in RTAs sustained soft-tissue injuries (78.9%) and a quarter (25.3%) also sustained various cuts and open wounds, with a laceration/abrasion rate of 22.9%.
The head injury rate was 39.7%, which explains the large number of CT scans of the brain performed in our study (66.7%). Children, especially infants, may suffer major head trauma, especially as their head comprises a significant proportion of their total body weight.
A global childhood unintentional surveillance study conducted by the WHO[5] - mostly in low- and middle-income countries -of injured children < 12 years of age, showed that, among those suffering road traffic injuries, concussion occurred in 26% and a further 3.2% experienced other head injuries. In our study, there was a 20.5% concussion rate.
There also seemed to be a small number of children who sustained fractures or other significant limb injuries (only 25 of the 156 patients sustained fractures (16%)) compared with the percentage in the study by Pretorius and Firth,[4] which showed that 13.4% of orthopaedic admissions over a 3-year period were due to RTAs.
The current study showed that 65% of the children involved in RTAs were boys. This percentage is consistent with that in numerous other paediatric studies, although not directly comparable, as our study only included children <10 years of age, with a higher injury rate in boys. This trend appears to continue into adulthood,[3-10] which may be due to boys generally displaying more risk-seeking behaviour and having a greater affinity for competitive behaviour. This concept, however, has not been investigated in our study.
A study by Van As and Millar[11] at Red Cross War Memorial Children's Hospital, Cape Town, SA, which included 4 690 patients, reported a mean age of children injured in RTAs as 6.3 years and RTA-related injuries as 40%. According to the literature, the mean age of children involved in RTAs ranges between 5 and 11 years;[1,4,7,8] however, we reported a mean age of 4.8 years, which could reflect the younger cut-off age of 10 years.
Globally, children involved in pedestrian accidents form the largest category of those injured on the roads.[2] This was reflected in our study, where 78.8% of children were involved in PVAs. Nevertheless, our PVA rate is very high compared with those in other international studies conducted in large urban cities, such as Singapore (28.5%)[7] and Montreal (57%),[9] and the multi-country global childhood unintentional injury surveillance study in Bangladesh, Colombia, Egypt and Pakistan (39%).[6]
Study limitations
This study required doctors who work in high-volume emergency units to collect data. Therefore, a large number of patients with minor injuries, not requiring work-up, would have been missed, which could explain the 97% admission rate. The burden of children
involved in RTAs was not fully assessed, as children who sustained minor or no injuries may have been attended to at local clinics or did not present to a healthcare facility.
The data were gathered from the caregiver of the child, which might have led to an inaccurate description of who was with the child at the time of the incident for fear of repercussions.
The exclusion ofpatients presenting to the orthopaedic department might have resulted in the fracture rate being underestimated. Some patients with isolated limb injuries may have been admitted directly and managed in orthopaedic departments.
Mortality was not investigated and therefore not all RTAs included were necessarily non-fatal, including children who succumbed to their injuries on the scene or who were declared dead on arrival.
Conclusion
RTAs are a leading cause of injuries and fatalities globally, particularly in low-income countries such as SA. Our study, along with other studies, shows that the paediatric population is at risk, specifically of being injured as a pedestrian. Children sustain a wide variety of injuries on our roads, the majority being soft-tissue injuries, followed by head injuries.
A major finding from this study is the lack of adult supervision of children < 10 years on and around the roads in Soweto, which, in turn, increases the rate of injuries sustained, particularly head injuries. In addition, the majority of children travelling in vehicles are not restrained, both in private and public transport. This situation needs to be addressed in our community.
Our study highlights the need for these outreach and educational programmes to continue to raise awareness and to help to reduce the number of children injured on and around our roads.
Declaration. The research for this study was done in partial fulfilment of the requirements for J-AC's MMed (Surgery) degree at the University of the Witwatersrand, Johannesburg, South Africa.
Acknowledgements. This Master's project took a number of years to complete. Time is a difficult thing to come by while managing a general surgery registrar post, as well as being a wife and mother. I am forever grateful to my mother for her unwavering support and immense help with this project, and to my husband for his patience. Special thanks to Prof. Deirdre Kruger, without whose continued encouragement and assistance I doubt this project would have been possible.
Author contributions. J-AC: conceived and designed the analysis, collected the data, performed the analysis and wrote the article; DK: contributed to designing the analysis, to the data and analysis tools, to performing the analysis and to editing the article; JL: contributed to conceiving and designing the analysis and to editing the article.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization. Global Status Report on Road Safety 2018: Summary. Geneva: WHO, 2018. https://www.who.int/publications/i/item/9789241565684 (accessed 14 March 2021). [ Links ]
2. Bradshaw D, Bourne D, Nannan N. What are the leading causes of death among South African children? MRC Policy 2003;3. https://www.samrc.ac.za/sites/default/files/attachments/2016-06-30/childmortality.pdf (accessed 18 August 2022). [ Links ]
3. Peclet MH, Newman KD, Eichelberger MR, et al. Patterns of injury in children. J Paediat Surg 1990;25(1):85-90. https://doi.org/10.1016/s0022-3468(05)80169-1 [ Links ]
4. Pretorius CJ, Firth GB. Road traffic accidents and orthopaedic injuries in children. S Afr Orthopaed J 2009;9(3);65-68. [ Links ]
5. Peden M, Oyegbite K, Ozanne-Smith J, eds. World Report on Child Injury Prevention. Geneva: World Health Organization, 2008. [ Links ]
6. Hyder AA, Sugerman DE, Puvanachandra P, et al. Global childhood unintentional injury surveillance in four cities in developing countries: A pilot study. Bull World Health Organ 2009;87:345-352. https://doi.org/10.2471/BLT.08.055798 [ Links ]
7. Lee YY, Fang E, Weng Y, et al. Road traffic accidents in children: The 'what, 'how' and 'why. Singapore Med J 2018;59(4):210-216. https://doi.org/10.11622/smedj.2017114 [ Links ]
8. Durkin MS, Laraque D, Lubman I, Barlow B. Epidemiology and prevention of traffic injuries to urban children and adolescents. Pediatrics 1999;103(6):e74. https://doi.org/10.1542/peds.103.6.e74 [ Links ]
9. Pless IB, Verreault R, Arsenault L, Frappier JY, Stulginskas J. The epidemiology of road accidents in childhood. Am J Public Health 1987;77(3):358-360. https://doi.org/10.2105/ajph.77.3.358 [ Links ]
10. Rivara FP, Barber M. Demographic analysis of childhood pedestrian injuries. Pediatrics 1985;76(3):375-381. [ Links ]
11. Van As AB, Millar AJW. From the pursuit of excellence to the quest for significance: Promotion of a Childsafe South Africa. S Afr Med J 2012;102;(6)427-428. https://doi.org/10.7196/samj.5602 [ Links ]
12. Fatimah M, Osman A, Masyarakat JK, Perubatan F. The risk of road traffic accidents among primary school children in Kuala Terengganu. Med J Malaysia 1997;52(4):402-408. [ Links ]
13. Pless IB, Verreault R, Tenina S. A case control study of pedestrian and bicyclist injuries in childhood. Am J Public Health 1989;79(8):995-998. https://doi.org/10.2105/ajph.79.8.995 [ Links ]
14. Zeedyk MS, Wallace L, Spry L. Stop, look, listen, and think? What young children really do when crossing the road. Accident Analysis Prevent 2002;34(1):43-50. https://doi.org/10.1016/s0001-4575(00)00101-9 [ Links ]
15. Chen IG, Durbin DR, Elliott MR, Kallan MJ, Winston FK. Trip characteristics of vehicle crashes involving child passengers. Injury Prevent 2005;11(4):219-224. https://doi.org/10.1136/ip.2004.006767 [ Links ]
16. Durocher A. Car seat safety. Safe Ride 4 Kids. 2016. https://saferide4kids.com/blog/law-versus-best-practice/ (accessed 3 August 2021). [ Links ]
17. Car seats for children and road safety in South Africa. https://www.arrivealive.co.za/Car-Seats-for-Kids-and-Road-Safety-in-South-Africa (accessed 25 March 2021). [ Links ]
18. Zaza S, Sleet DA, Thompson RS, et al. Reviews of evidence regarding interventions to increase use of child safety seats. Am J Prev Med 2001;21(4 Suppl):31-47. https://doi.org/10.1016/s0749-3797(01)00377-4 [ Links ]
19. Snowdon A, Rothman L, Slater M, et al. A comparison of booster seat use in Canadian provinces with and without legislation. Injury Prevent 2009;15(3):230. https://doi.org/10.1136/ip.2008.020537. [ Links ]
20. South African market insights, Soweto in detail: Social statistics. 2017. https://www.southafricanmi.com/soweto-in-detail.html (accessed 14 March 2021) [ Links ]
 Correspondence:
Correspondence:
J-A Carreira
jo-annecarreira@hotmail.com
Accepted 21 July 2021


{kind=link}
{kind=link}
{kind=link}