










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.16 n.3 Pretoria Sep. 2022
http://dx.doi.org/10.7196/SAJCH.2022.v16i3.1901
RESEARCH ARTICLE
South African neonates with mild and moderate hypoxic-ischaemic encephalopathy
R MalanI; J van der LindeII; A KritzingerII; M CoetzeeIII; M A GrahamIV; E KrügerII
IM Comm Path; Department of Speech-Language Pathology and Audiology, Faculty of Humanities, University of Pretoria, South Africa
IIDPhil Comm Path; Department of Speech-Language Pathology and Audiology, Faculty of Humanities, University of Pretoria, South Africa
IIIMB ChB, MPhil (Neonatology); Department of Paediatrics and Child Health, Division of Neonatology, Steve Biko Academic Hospital and Faculty of Health Sciences, University of Pretoria, South Africa
IVBSc Fin Math, DPhil Math Stat; Department of Science, Mathematics and Technology Education, Faculty of Education, University of Pretoria, South Africa
ABSTRACT
BACKGROUND. Clear risk profiles of neonates with mild and moderate hypoxic-ischaemic encephalopathy (HIE) are lacking.
OBJECTIVE. To describe and compare factors associated with mild and moderate HIE in South African neonates.
METHODS. A prospective, comparative design was used to describe factors among South African neonates with mild (n=13) and moderate (n=33) HIE in an urban tertiary academic hospital. HIE diagnosis and encephalopathy grading were conducted using the modified Sarnat stages. Thompson scores were recorded. Participants' clinical records were reviewed to identify factors. Descriptive data were obtained. Chi-square and Fisher's exact tests were used to compare categorical data, and Mann-Whitney tests were used to compare continuous data between groups.
RESULTS. Significant differences were found between groups' admission (p<0.001) and highest Thompson scores (p<0.001). The mild group's APGAR scores were significantly higher than those of the moderate group at five (p=0.012) and ten minutes (p=0.022). Duration of resuscitation (p=0.011) and time to spontaneous respiration (p=0.012) also differed significantly between groups. Significantly more moderate than mild participants received therapeutic hypothermia (TH) (p<0.001).
CONCLUSION. Clinical tests and management factors differed significantly between groups. The findings provided the multidisciplinary team with an increased understanding of the heterogeneous HIE population and add to existing evidence for identifying neonates eligible for TH in resource-limited settings.
Hypoxic-ischaemic encephalopathy (HIE) is the fifth leading cause of death in children under five years globally and is a significant problem in low- and middle-income countries (LMICs).[1,2] Among survivors, HIE is a significant cause of cerebral palsy, seizures, sensory impairment, learning difficulties, cognitive or behavioural fallouts, and communication difficulties.[2-4] HIE, therefore, has a profound burden of disease.[2]
The HIE population is heterogeneous, with different clinical pictures and recovery patterns.[3,4] Using the modified Sarnat stages and/or Thompson score, HIE can be graded as mild, moderate or severe.[5-7] This grading can contribute to long-term prognostication, clinical decision-making and parent counselling because individual outcomes are often linked with severity of the neonatal condition.[3] Owing to the high incidence of HIE in LMICs and associated health concerns, the multidisciplinary team (MDT) requires a thorough understanding of HIE across severity types. Factors such as lack of antenatal care, intra-uterine growth restriction, prolonged second stage of labour, meconium-stained amniotic fluid, eclampsia and lower socio-economic status were previously linked to HIE in LMICs.[8-10] However, gaps in research, including dated studies, retrospective designs and lack of universally accepted HIE definitions, exist. Also, few studies compared factors between severity types, often grouping moderate and severe infants together or comparing survivors and non-survivors.[8,11]
Severe HIE has previously been researched and it is widely accepted that this neonatal group is at a significantly higher risk of mortality and major neurodevelopmental impairment.[4,8,11] Conversely, neonates with moderate HIE are more variable and their outcomes more difficult to predict.[4] Similarly, neonates with mild HIE frequently escape attention, despite mild HIE being more prevalent than moderate and severe HIE in many contexts and there being evidence suggesting adverse neurological and long-term developmental outcomes in this group.[12] The present study aimed to describe and compare factors associated with mild and moderate HIE in a sample of South African neonates.
Methods
A prospective, comparative design was used to describe factors among 46 neonates with mild and moderate HIE during admission to the 29-bed neonatal high-care unit of an urban tertiary academic hospital in South Africa between October 2018 and January 2020. Approval to conduct the study was obtained (protocol number 380/2018).
Neonatal encephalopathy was suspected to be secondary to an acute peri- or intrapartum event if participants presented with encephalopathy (disturbed neurological function manifested as an abnormal level of consciousness or seizures, possibly accompanied by respiratory difficulties and decreased tone and/or primitive reflexes), and had APGAR scores <5 at 5 and 10 minutes, or had evidence of fetal acidaemia (arterial umbilical cord blood gas or radial artery blood gas done within 60 minutes of delivery with a pH <7.0 or a base deficit >12 mmol/L).[13,14] Encephalopathy grading was performed using the modified Sarnat stages and was confirmed by a neonatologist.[6] Serial modified Sarnat scores were performed during the first 6 hours of life and, if there was progression of disease, the worse staging was assigned to the participant. Thompson scores were conducted daily until day 10 of life. Participants' first, highest and day seven Thompson scores were recorded where available.[7] Eligible neonates were born >37 weeks' gestation, using the most reliable information available, in order of preference being: ultrasound before 22 weeks' gestation, sure dates or new Ballard score.[15] Non-probability purposive sampling was used to recruit neonates meeting inclusion criteria.
Neonates with genetic syndromes, major congenital abnormalities, metabolic disease, meningitis, structural brain abnormalities, intracerebral or intraventricular haemorrhage, congenital hydrocephalus or perinatal stroke were excluded. Sixty-two neonates with mild or moderate HIE were identified. Sixteen were excluded for: lack of consent (n=7), demise before consent (n=2), meningitis (n=5), maternal myasthenia gravis (n=1) and Down syndrome (n=1). Forty-six participants were included in the study; 28.3% (n=13) had mild HIE and 71.7% (n=33) had moderate HIE.
Participants' clinical records were prospectively reviewed, and a checklist of factors related to the neonate and mother was used to capture data.[8,9,16] The SPSS statistical software package, version 26.0 (IBM Corp., USA), was used for all statistical analyses, except for the power calculation, which was done using G*Power version 3.1.9.4 (Heinrich Heine Universität, Düsseldorf). Factors from participants' clinical records comprised categorical and continuous variables and, for the latter, the Shapiro-Wilk test was used to test normality.[17] As normality was not detected, non-parametric tests were used. Chi-square and Fisher's exact tests were used to compare categorical data, and Mann-Whitney tests were used to compare continuous data between mild and moderate groups. For a level of significance of 0.05, the study's achieved power was 0.839, which is above the minimally acceptable achieved power of 0.8.[18]
Results
Participants (n=46) were divided into two groups based on whether they had mild (n=13) or moderate (n=33) HIE. Admission and highest Thompson scores were recorded for 44 participants (Table 1). The mild group had significantly lower admission (p<0.001) and highest Thompson scores (p<0.001) than the moderate group. Day seven scores were recorded for the minority of the sample (n=5; 10.9%).
Factors investigated were categorised as follows: antepartum, intrapartum, maternal, environmental and management factors.
Antepartum factors
Most participants were male (n=29; 63.0%), with a median gestation of 38.5 weeks. Antepartum factors did not differ significantly between groups (Table 2).
Intrapartum factors
Intrapartum factors included clinical tests such as APGAR scores, arterial pH and base deficit values (Table 3). The mild group's APGAR scores were significantly higher than those of the moderate group at five (p=0.012) and 10 minutes (p=0.022).
Mode of delivery and birth complications were also investigated but did not differ significantly between groups (Table 4). Sentinel events included the second twin being retained for more than one hour (n=2) and placental abruption (n=1). Birth complications other than those in Table 4 included breech presentation (n=6); transfer during labour (n=3); poor maternal effort (n=2); unco-operative mother (n=2); aspiration of blood by neonate (n=2); failed induction of labour (n=1); low-lying placenta (n=1); antepartum haemorrhage (n=1); prolonged latent stage of labour (n=1); maternal seizure at birth (n=1); eclampsia (n=1); and one case where the participant was born in the Casualty Department of a referring hospital. Some participants presented with more than one birth complication.
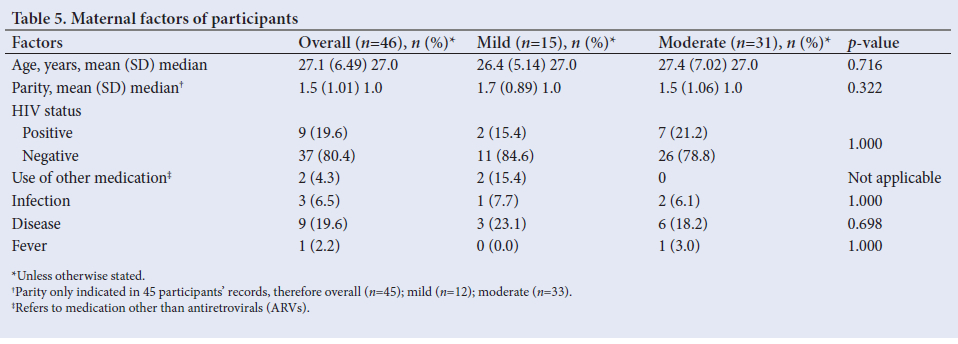
Maternal factors
Maternal factors did not differ significantly between groups (Table 5). The median maternal age was 27.0 years (minimum 15.0 years, maximum 44.0 years). Seven mothers (15.2%) were teenagers (<20 years), and four (8.7%) were of advanced maternal age (>35 years). Most mothers were primigravida (n=31; 67.4%), with 53.8% of mild participants' (n=7) and 72.7% of moderate participants' mothers (n=24) following this trend. Nine mothers (19.6%) were HIV positive; all of them used antiretrovirals (ARVs) during pregnancy. Two mothers used other medications; one used methyldopa and the other used herbal medication. Two mothers had urinary tract infections, and one reported a green vaginal discharge during pregnancy. The following maternal diseases were recorded: obesity (n=2); pre-eclampsia (n=2); gestational diabetes mellitus (n=2); drug-induced jaundice (n=1); elevated low-density lipoprotein (LDL) cholesterol (n=1); and gestational hypertension (n=1).
Environmental factors
Few clinical records reflected environmental factors such as parental marital or employment status. Participants came from urban (n=36; 78.3%) and peri-urban areas (n=9; 19.6%) and were mostly born at the hospital where the study was conducted (n=33; 71.7%). Statistically significant differences were not observed between groups.
Management factors
Thirty-six participants (78.3%) (eight mild (61.5%) and 28 moderate (84.8%)) required resuscitation at birth. Two participants (4.3%) received naloxone. No significant differences existed between groups' components of resuscitation (Table 6). Resuscitation duration differed significantly between groups (p=0.011). Overall, the median resuscitation duration was three minutes, with the moderate group requiring longer resuscitation than the mild group (median 5.0 minutes v. median 0.0 minutes). Length of time to spontaneous respiration was recorded in 20 participants' files and also differed significantly between groups (p=0.012), with the moderate group experiencing longer times to spontaneous respiration than the mild group (median 5.0 minutes v. median 0.0 minutes).
Thirty-six participants (78.3%) received whole-body therapeutic hypothermia (TH), where core body temperature was kept at 33.5°C - 34.5°C for 72 hours using servo-controlled methods (n=33; 91.2%) or frozen gel packs (n=3; 8.3%). Significantly more moderate (n=32; 97.0%) than mild participants (n=4; 30.8%) received TH (p<0.001). Overall, 10 participants (21.7%) did not receive TH; nine (90.0%) did not meet eligibility criteria and one participant (10.0%) was too unstable.
Discussion
Of the 46 participants, 28.3% (n=13) presented with mild and 71.7% (n=33) presented with moderate HIE. Although it is often estimated globally that 50.0% of neonates with HIE are mild,[1,12] the distribution of HIE in the present study is similar to other South African findings, where moderate and severe categories account for greater proportions of the HIE population.[8] This study used the modified Sarnat stages and not Thompson scores to grade participants.[5-7] Although Thompson scoring has limitations and may be influenced by factors such as TH and sedation,[19] this study suggests that allocating Thompson scores remains important, as demonstrated by the significant differences between groups for admission and highest Thompson scores. Furthermore, the median admission and highest Thompson scores for the mild (5.0 and 5.0) and moderate groups (10.0 and 10.5) are similar to a recent publication that suggests that the mild modified Sarnat stages align with a Thompson score of 5 - 6 and that the moderate modified Sarnat stages align with a Thompson score of 7 - 13.[20]
When comparing factors between mild and moderate groups, neither biological factors such as antepartum and maternal factors, mode of delivery and birth complications, nor environmental factors differed significantly. Management factors such as resuscitation duration and length of time to spontaneous respiration, and clinical tests such as five- and 10-minute APGAR scores were the only factors that could distinguish the two groups.
Similar to findings of Padayachee and Ballot,[11] the median gestation of participants was 38.5 weeks. The majority of study participants were male (n=29; 63.0%), which is comparable with other studies in LMICs.[8,9] As with other African studies, most mothers were primigravida (n=31; 67.4%).[8,10,11] The median maternal age was 27.0 years, which is higher than that of other studies.[8,9,11] This may reflect the global pattern of increasing maternal age.[21] Seven participants (15.2%) were born to teenage mothers, and four (8.7%) to mothers of advanced age. Childbearing during these years may pose increased risks to mothers and neonates.[21]
The median birthweight was 3 097.5 g, and 82.6% (n=38) of participants had appropriate growth for gestational age. Only 15.2% (n=7) of participants were small for gestational age (SGA). This differs from other studies where intra-uterine growth restriction was the most common antepartum factor associated with HIE.[22] Of the entire sample, 19.6% (n=9) were born to mothers who were HIV positive; this figure is lower than the reported prevalence of 25.9% among neonates with HIE.[8] All affected mothers in the study took ARVs during pregnancy. Only 50% (n=23) of mothers attended antenatal care, which is much less than mothers of infants with HIE in other South African studies, where 95.6% and 68.0% received antenatal care, respectively.*11 This difference may be due to poor record-keeping.
The present study found that both five- and 10-minute APGAR scores were significantly associated with HIE severity, while previous studies only reported a significant association between the 10-minute APGAR score and severity of HIE.[8,23] An arterial cord or radial pH level taken within 60 minutes after birth of less than 7.0, often plays a key role in identifying an intrapartum hypoxic event.[13] However, the median pH levels of both groups exceeded 7.0 in this study. As arterial blood gas analysis provides a representation of a neonate's respiratory and metabolic status, one of the factors contributing to the arterial pH exceeding 7.0 in this study may be secondary to a low partial pressure of arterial carbon dioxide (PaCO2) influencing pH levels in spontaneously breathing acidotic infants.[24]
The proportion of participants requiring resuscitation increased as HIE severity increased, and resuscitation duration and length of time to spontaneous respiration were significantly higher for the moderate group. Although the need for resuscitation at birth and resuscitation components such as need for chest compressions or adrenaline were previously significantly associated with poorer outcomes in neonates with HIE, these were not significantly associated with HIE severity in the present study.[8,11]
TH was the main neuroprotective strategy implemented among participants and, as expected, significantly more moderate participants received TH. As per international recommendations and the neonatal unit's protocol, participants with moderate HIE received TH routinely, unless too unstable (n=30; 96.8%). Although there are currently no recommendations for providing TH to neonates with mild HIE, four participants with mild HIE inadvertently received TH (30.8%). This trend is reflected in numerous studies from other countries.[25]
There is a paucity of literature on neonates with mild HIE, and neonates with moderate HIE are variable, with outcomes that are difficult to predict.[4] Obtaining clearer risk profiles of neonates with mild v. moderate HIE may help the MDT better understand these populations, to utilise resources such as TH more effectively.
Study limitations include no participants living in rural areas and incomplete information on participants' environmental factors, antenatal care and day seven Thompson scores. Future research should use complete clinical records and should include participants living in rural areas. Large-scale prospective studies in LMICs are also warranted to further investigate factors associated with different stages of HIE. The potential for early factors associated with HIE to predict later outcomes should also be explored.
Conclusion
This study used strict inclusion criteria and prospective methods to describe and compare factors associated with mild and moderate HIE, two distinct severity types with less clear risk profiles than their severe counterparts. Results showed significant differences between the groups, confirming the value of performing various clinical measures. Management factors such as resuscitation duration, length of time to spontaneous respiration and TH, and clinical tests such as five- and 10-minute APGAR scores differed significantly between participants with mild and moderate HIE. Conversely, other biological and environmental factors could not distinguish groups. Admission and highest Thompson scores were significantly lower in participants with mild compared with moderate HIE, indicating that performing the Thompson score remains important. These findings provide the MDT with an increased understanding of the heterogeneous HIE population and adds to existing evidence for identifying neonates eligible for TH in resource-limited settings.
Declaration. None.
Acknowledgments. None.
Author contributions. RM conceptualised the project, collected and analysed the data, and wrote this article. JV, AK and EK conceptualised the project, and assisted with writing and editing. MC assisted with participant identification, data collection and editing. MAG analysed the data, compiled statistics and assisted with editing.
Funding. None.
Conflicts of interest. None.
References
1. Lee AC, Kozuki N, Blencowe H, et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res 2013;74(s1):50-72. https://doi.org/10.1038/pr.2013.206 [ Links ]
2. Ballot DE, Rakotsoane D, Cooper PA, Ramdin TD, Chirwa T, Pepper MS. A prospective observational study of developmental outcomes in survivors of neonatal hypoxic ischaemic encephalopathy in South Africa. S Afr Med J 2020;110(4):308-312. https://doi.org/10.7196/SAMJ.2020.v110i4.14311 [ Links ]
3. Pin TW, Eldridge B, Galea MP. A review of developmental outcomes of term infants with post-asphyxia neonatal encephalopathy. Eur J Paediatr Neurol 2009;13:224-234. https://doi.org/10.1016/j.ejpn.2008.05.001 [ Links ]
4. Schreglmann M, Ground A, Vollmer B, Johnson MJ. Systematic review: Long-term cognitive and behavioural outcomes of neonatal hypoxic-ischaemic encephalopathy in children without cerebral palsy. Acta Paediatr 2019;109(1):20-30. https://doi.org/10.1111/apa.14821 [ Links ]
5. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. Arch Neurol 1976;33:696-705. [ Links ]
6. Shalak LF, Laptook AR, Velaphi SC, Perlman, JM. Amplitude integrated electroencephalography coupled with an early neurologic examination enhances prediction of term infants at risk for persistent encephalopathy. Pediatrics 2003;111(2):351-357. [ Links ]
7. Thompson CM, Puterman, AS, Linley LL, et al. The value of a scoring system for hypoxic ischaemic encephalopathy in predicting neurodevelopmental outcome. Acta Paediatr Scand 1997;86:757-761. [ Links ]
8. Bruckmann EK, Velaphi S. Intrapartum asphyxia and hypoxic ischaemic encephalopathy in a public hospital: Incidence and predictors of poor outcome. S Afr Med J 2015;105(4):298-303. https://doi.org/10.7196/SAMJ.9140 [ Links ]
9. Ibrahim MH, Asmaa MN. Perinatal factors preceding neonatal hypoxic ischemic encephalopathy in El-Minia locality. Gynecol Obstet (Sunnyvale) 2016;6(9):403. https://doi.org/10.4172/2161-0932.1000403 [ Links ]
10. Namusoke H, Nannyonga MM, Ssebunya R, Nakibuuka VK, Mworozi E. Incidence and short term outcomes of neonates with hypoxic ischemic encephalopathy in a peri urban teaching hospital, Uganda: A prospective cohort. Matern Health Neonatol Perinatol 2018;4(6). https://doi.org/10.1186/s40748-018-0074-4 [ Links ]
11. Padayachee N, Ballot DE. Outcomes of neonates with perinatal asphyxia at a tertiary academic hospital in Johannesburg, South Africa. S Afr J Child Health 2013;7(3):89-94. https://doi.org/10.7196/SAJCH.574 [ Links ]
12. Conway JM, Walsh BH, Boylan, GB, Murray DM. Mild hypoxic ischaemic encephalopathy and long term neurodevelopmental outcome - a systematic review. Early Hum Dev 2018;120:80-87. https://doi.org/10.1016/j.earlhumdev.2018.02.007 [ Links ]
13. American Academy of Pediatrics. Executive summary: Neonatal encephalopathy and neurologic outcome. Obstet Gynecol 2014;123:896-901. https://doi.org/10.1542/peds.2014-0724 [ Links ]
14. Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med 2005;353(15):1574-1584. [ Links ]
15. American College of Obstetricians and Gynecologists. ACOG committee opinion Number 700. Obstet Gynecol 2017;129(5):e150-e154. https://doi.org/10.1097/AOG.0000000000002046 [ Links ]
16. Badawi N, Kurinczuk JJ, Keogh JM, et al. Antepartum risk factors for newborn encephalopathy: The Western Australian case-control study. BMJ 1998;317:1549-1553. [ Links ]
17. Field A. Discovering Statistics Using IBM SPSS Statistics. 5th ed. United Kingdom: SAGE Publishers; 2018. [ Links ]
18. Cohen J. A power primer. Psychol Bull 1992;112(1):155-159. [ Links ]
19. Mendler MR, Mendler I, Hassan MA, Mayer B, Bode H, Hummler, HD. Predictive value of Thompson-score for long-term neurological and cognitive outcome in term newborns with perinatal asphyxia and hypoxic-ischemic encephalopathy undergoing controlled hypothermia treatment. Neonatology 2018;114:341-347. https://doi.org/10.1159/000490721 [ Links ]
20. Chansarn P, Torgalkar R, Wilson D, et al. Correlation of Thompson and modified Sarnat scores in neonatal hypoxic ischemic encephalopathy. J Perinatol 2021;41:1522-1523. https://doi.org/10.1038/s41372-021-00987-x [ Links ]
21. Londero AP, Rossetti E, Pittini C, Cagnacci A, Driul L. Maternal age and the risk of adverse pregnancy outcomes: A retrospective cohort study. BMC Pregn Childbirth 2019;19:261. https://doi.org/10.1186/s12884-019-2400-x [ Links ]
22. Yadav N, Damke S. Study of risk factors in children with birth asphyxia. Int J Contemp Pediatr 2017;4(2):518-526. https://doi.org/10.18203/2349-3291.ijcp20170701 [ Links ]
23. Laptook AR, Shankaran S, Ambalavanan N, et al. Prediction of early childhood outcomes of term infants using Apgar scores at 10 minutes following hypoxic-ischemic encephalopathy. Pediatrics 2009;124(6):1619. https://doi.org/10.1542/peds.2009-0934 [ Links ]
24. Szakmar E, Jermendy A, El-Dib M. Respiratory management during therapeutic hypothermia for hypoxic-ischemic encephalopathy. J Perinatol 2019;39: 763-773. https://doi.org/10.1038/s41372-019-0349-2 [ Links ]
25. Goswami IR, Whyte H, Wintermark P, Mohammed K, Shivanada S, Louis D. Characteristics and short-term outcomes of neonates with mild hypoxic-ischemic encephalopathy treated with hypothermia. J Perinatol 2020;40:275-283. https://doi.org/10.1038/s41372-019-0551-2 [ Links ]
 Correspondence:
Correspondence:
R Malan
malanroxanne@gmail.com
Accepted 1 August 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}