










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Child Health
versión On-line ISSN 1999-7671
versión impresa ISSN 1994-3032
S. Afr. j. child health vol.16 no.2 Pretoria jun. 2022
http://dx.doi.org/10.7196/sajch.2022.v16i2.1846
RESEARCH
Child development at age 5 years: The effects of maternal education, socioeconomic status and early-life growth examined prospectively in a low-resource setting
W StemmingI; SA NorrisII, III; J KaguraIV; H SaloojeeV; L RichterIII
IPhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; MRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics and Child Health, University of the Witwatersrand, Johannesburg, South Africa
IIIPhD; DSI-NRF Centre of Excellence in Human Development, University of the Witwatersrand, School of Public Health, Johannesburg, South Africa
IVPhD; Department of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
VMMed; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Deeper insight into relationships between social factors and early childhood growth and development is required, particularly in low-resource settings
OBJECTIVES: To determine (i) associations between early linear growth and child development at 5 years; and (ii) whether early childhood growth mediates relationships between maternal education, household socioeconomic status (SES) and subsequent child development
METHODS: This study used data from the Birth to Twenty Plus study, a longitudinal South African birth cohort study. The study sample comprised 636 participants with complete data at all relevant time points for the analysis. Household SES and maternal education were measured during pregnancy and the first two years of life, and growth between birth and 4 years of age. Child development was assessed using the Revised Denver Pre-screening Developmental Questionnaire (R-DPDQ). Multivariable regression analyses were used to investigate the association between SES, maternal education, growth and child development, and structural equation modelling was used to analyse the mediation of growth
RESULTS: In both sexes, higher birthweight and household SES were associated with higher R-DPDQ scores. Increased relative linear growth, particularly between 0 and 2 years, was associated with higher R-DPDQ scores among boys (β=0.82; 95% confidence interval (CI): 0.27 - 1.37) at age 5. Growth status but not SES mediated the association between maternal education and R-DPDQ scores
CONCLUSION: Child development at 5 years was independently associated with SES and birthweight. The negative effects of lower maternal education on child development was attenuated by better growth
The period from conception to 3 years of age is associated with rapid growth and development. Development during this particularly malleable period lays the foundation for a childs ability to learn, grow and participate in activities with others.[1,2] Children living in impoverished environments are at greater risk of compromised emotional, cognitive and social development.[3] As risk factors are cumulative and interactive,[4] children who experience poor growth early in life are also more likely to be exposed to suboptimal physical and psychosocial environments before and after birth.[5]
Evidence suggests that growth during the early years affects child development outcomes variably in different settings.[6-8] Studies conducted in low-resource settings, such as Colombia and Bangladesh, have explored these relationships in detail, but with conflicting results.[7,8] Differences in findings could be explained by contextual factors, such as variations in extreme (absolute) poverty levels and the prevalence of malnutrition. As there is limited evidence on this in Africa, further research is required to understand the relative effects of individual proximal exposures and the potential additive or mediating effects of growth on child development in low-resource settings.
This study, using data from a longitudinal birth cohort, aimed to explore the relationships between maternal education and household socioeconomic status (SES), early child growth and child development outcomes in a low-resourced, urban setting. The study assessed associations between early childhood growth (between birth and age 4 years) and child development at 5 years of age. It also assessed whether early childhood growth mediated associations between maternal education, household SES and child development at age 5, and if so, how
Methods
Study design and participants
The analysis used data from the Birth to Twenty Plus (Bt20+) study, a longitudinal birth cohort study of children born in Soweto, Johannesburg, South Africa.[9] For that study, pregnant women attending antenatal care at public health facilities were recruited and 3 273 singletons born between 23 April and 8 June 1990 were enrolled. Details of the study methods, profile and attrition of the Bt20+ cohort are available elsewhere.[9]
Maternal and infant data collected during pregnancy, at birth and between 6 months and 5 years of age were extracted from the Bt20+ database. The analytical sample for the current study included 636 participants with data at all relevant time points.
Child development measure
The Revised Denver Prescreening Developmental Questionnaire (R-DPDQ) was used to assess child development, when the index children were 5 years old.[10] The questionnaire comprises 32 items covering the child's motor, language, personal-social and cognitive abilities, which allows for preschool children at risk of developmental delays to be identified. The assessment included asking caregivers a set of questions, together with children being required to complete a series of age-appropriate tasks. The R-DPDQ was piloted for feasibility and appropriateness prior to inclusion in the Bt20+ study[11] Internal consistency (Cronbachs alpha) for the R-DPDQ measure in the Bt20+ sample was 0.72. An overall developmental score for each child was derived by adjusting the total raw score for the child's chronological age. The majority of participants had complete data on all 32 items; children with incomplete data missed mostly only one item.[12]
Maternal and household factors
Information on maternal education (years of schooling) and household SES was collected by trained, multilingual interviewers who verbally administered questionnaires to mothers between the third trimester of pregnancy and the first two years of childhood.
Ownership of a number of physical assets (car, television, refrigerator, landline telephone, radio, washing machine and house) was used to derive a proxy measure of household SES at the time. If an asset was present, a score of 1 was assigned; a score of 0 was assigned to assets not present in the household. This approach has been validated in similar studies, including in this cohort.[13,14]
Early childhood growth
In this cohort, weight was measured at birth, and length and height measures were recorded between 3 months and 4 years of age using standard procedures.[15] Z-scores were derived using the World Health Organization (WHO) growth standards.[15]
To address collinearity, conditional height variables (subsequently referred to as relative linear growth) were computed as residuals obtained by regressing present height on previous height and weight measures.[16] Conditional growth variables indicate deviation from a child's expected size based on their previous measures relative to the growth of other children (in a population or cohort). A positive value represents linear growth faster than predicted in a specified time interval, whereas a negative value represents slower growth than expected.
For the current analysis, we used relative linear growth between 0 and 2 years, and between 2 and 4 years. These variables are expressed in standard deviation units to allow direct comparison of regression coefficients.
Covariates
Parity, maternal height and quality of child care between 6 months and 2 years (a latent variable combining maternal responsiveness and cognitive stimulation in the home) were included as possible covariates in the regression analyses, based on the literature and prior analyses conducted on this cohort.
Statistical analysis
Our analyses present frequencies and percentages to describe categorical variables and continuous data are summarised using means and standard deviations (SDs). Stata 13.1 (Stata Corp., USA) was used for all analyses and statistical significance was set at p<0.05. Differences between the study sample included in the current analysis and the rest of the Bt20+ participants were assessed using Pearson's chi-squared (x2) test.
Sex-stratified multiple linear regression models were used to determine the associations between the exposure variables (birthweight and linear growth) and R-DPDQ scores at 5 years, adjusted for maternal education and household SES.
Modelling used a hierarchical approach. Individual factors (i.e. growth variables) were added first (model 1), followed by maternal education (model 2) and then household SES (model 3). Parity maternal height and quality of child care between 6 months and 2 years (a latent variable combining maternal responsiveness and cognitive stimulation in the home) were included as possible covariates in the regression analyses, based on the literature and prior analyses conducted on this cohort.
Regression analysis was followed by mediation analysis, using structural equation modelling (SEM) to assess whether early-life growth mediated the associations between maternal education, household SES and R-DPDQ scores at age 5. Fig. 1 depicts a standard path diagram for mediation analysis, which has been adapted to our model. A hypothetical SEM model was tested, which was partially informed by the results of the regression and correlation analyses, as well as a priori hypotheses as derived from the literature.[7,8] Child sex and quality of childcare in the home between 6 months and 2 years of age were adjusted for use in the SEM model, as these were associated with the outcome in regression analysis.
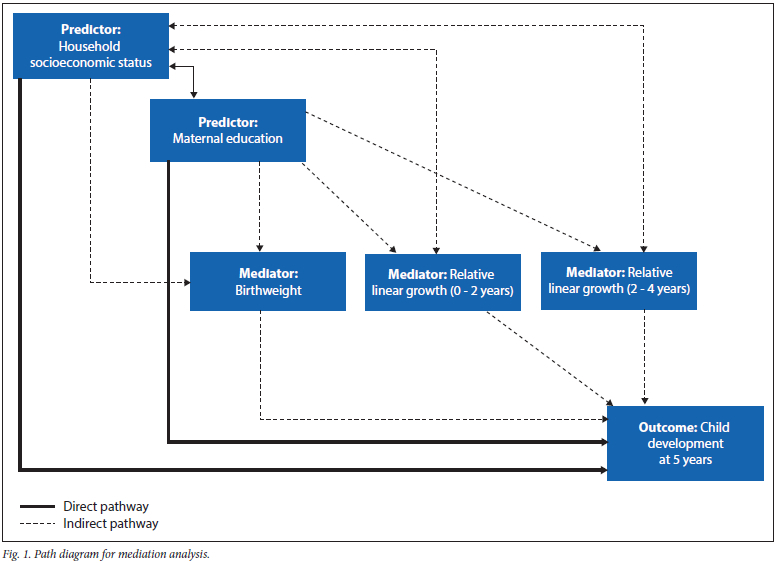
SEM results decompose the influences of one variable on another into direct, indirect and total effects. Direct effects represent the pathways from exogenous (exposure) variables (maternal education and household SES) to the outcome (R-DPDQ) while controlling for the mediators (birthweight and relative linear growth). Indirect effects depict the pathways from the exogenous variables to the outcome through the mediators. The total effects equal the sum of the direct and indirect (mediation) effects of the exogenous variables on the outcome.[17]
To evaluate the model that best fitted our data, we report goodness-of-fit indices, including the root mean square error of approximation (RMSEA), comparative fit indices (CFI) values and the standardised root mean square residual (SRMR).[17]
Ethical considerations
The Human Research Ethics Committee (Medical) of the University of the Witwatersrand granted ethical approval for the study (ref. no. M120609).
Results
Sample characteristics
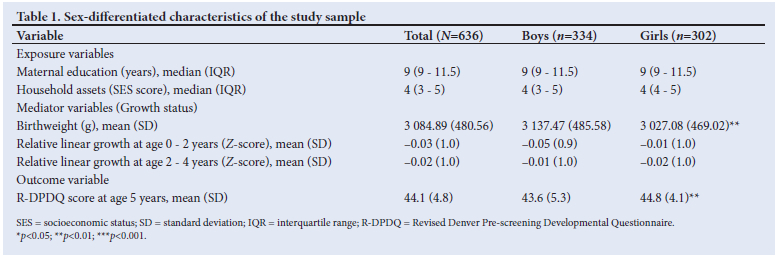
The R-DPDQ at age 5 years was completed for 1 231 children in the longitudinal study. Complete data for the questionnaire items and key exposure variables were available for 636 participants. The mean (SD) age of children included in the study at the time of developmental assessment was 62.6 (2.2) months, with 53% being male. Table 1 presents a summary of the study sample characteristics differentiated by sex.
Boys were significantly heavier at birth (mean difference: 110.4 g; 95% confidence interval (CI): 35.8 - 185.0 g). The mean (SD) R-DPDQ score at age 5 years was 44.1 (4.8) (range: 18.1 - 54.5), with boys scoring significantly lower than girls (mean difference: -1.2; 95% CI: -1.9 - -0.4).
The children included in the current analysis were more likely to be Black African, have mothers with comparatively higher levels of education and more household assets, and to score higher on the R-DPDQ (p<0.05 for all) compared with those excluded from the analysis. The two groups did not present significantly differently on growth parameters.
Effects of early-life growth and maternal and household exposures on R-DPDQ score at 5 years
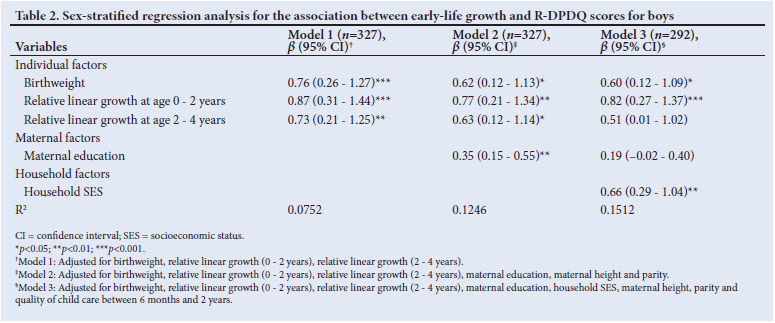
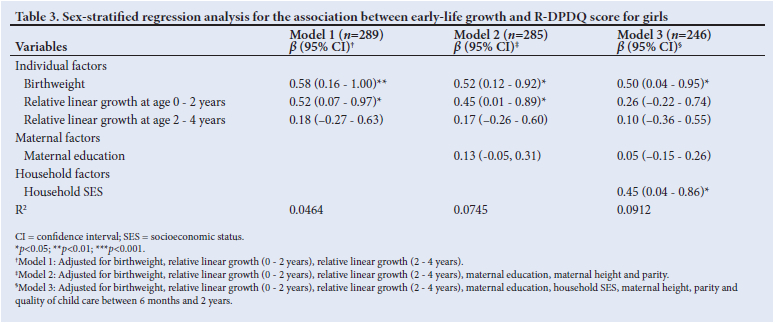
In sex-stratified multiple regression analysis, birthweight was positively associated with questionnaire scores for both sexes. These associations remained significant after controlling for maternal education, SES, parity, maternal height and quality of childcare. R-DPDQ scores increased by 0.6 units (β)3=0.60; 95% CI: 0.12 - 1.09) and 0.5 units (β)3=0.50; 95% CI: 0.04 - 0.95) for every 1 SD increase in birthweight for boys and girls, respectively (Table 2 and Table 3). In addition, relative linear growth between 0 and 2 years showed an independent association with R-DPDQ scores (β)3=0.82; 95% CI: 0.27 - 1.37) among boys. Household SES was also independently associated with R-DPDQ scores (for both boys and girls).
Mediation analysis
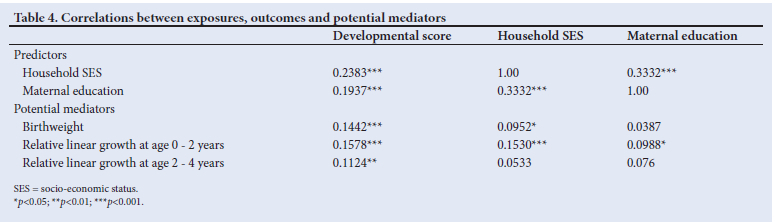
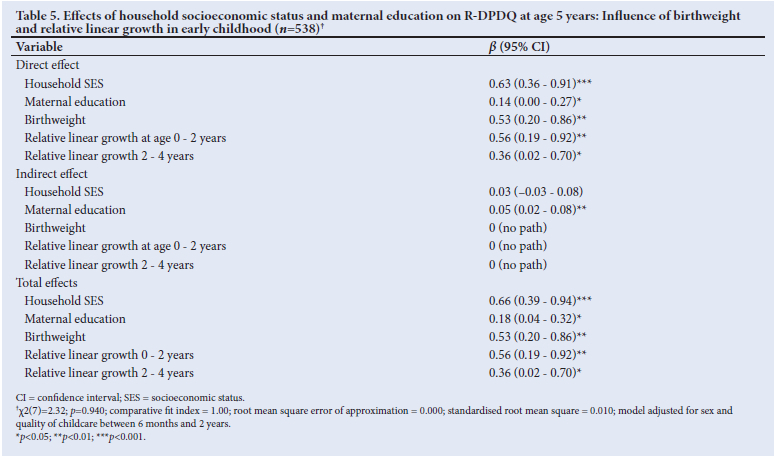
Correlations among the potential mediators (birthweight, and relative linear growth at 0 - 2 years and at 2 - 4 years), exposures (maternal education and household SES) and the outcome (R-DPDQ score) were examined (Table 4) to inform SEM analysis. Direct, indirect and total effects resulting from the SEM analysis are presented in Table 5.
Household SES showed significant direct effects on R-DPDQ scores, with no evidence of mediation by variables related to early-life growth. Thus, household SES was a key determinant of child development at age 5, independent of birthweight and relative linear growth (either at 0 - 2 years or 2 - 4 years) in this cohort. The direct path for the association between maternal education and R-DPDQ scores was significant and accounted for 78% of the total effect along this pathway. However, the association between maternal education and child development at age 5 was partially mediated by birthweight and relative linear early-life growth (between birth and 4 years) in this cohort. The assessed model indices indicated that the structural equation model fit the data well (Table 5).
Discussion
This study shows that birthweight (for both sexes) and (among boys) linear growth between birth and 2 years of age were positively associated with subsequent child development at age 5. This was independent of maternal education and household SES. The analysis also showed that the association between maternal education and R-DPDQ scores at 5 years was partially mediated by early-life growth status (birthweight and early-childhood linear growth), but not the association between SES and R-DPDQ scores.
There were clear associations between both prenatal and postnatal growth (using birthweight as a proxy) and child developmental outcomes. Although birthweight is often studied as a dichotomous variable (over or under 2 500 g), using a continuous birthweight measure revealed that higher infant birthweight was associated with higher R-DPDQ scores for both sexes. Positive relationships between birthweight and children's cognitive development have been observed elsewhere, including in lower-resourced settings.[18,19] Thus, interventions aimed at increasing birthweight may support or lead to gains in cognitive development in early childhood, although it is recognised that there is still some uncertainty as to the birthweight range that optimally promotes improved outcomes.[20]
The negative effects of stunting on child development are well described.[1] The pertinent evidence we add is that linear growth, particularly in the first two years of life, had significant independent effects on child development, predominantly among male children in this cohort. These effects persisted even when the influences of maternal and household factors were considered. These findings are biologically plausible as rapid physical growth and brain development generally occurs in the period from conception to age 3 years, providing the foundation for development throughout childhood and later life.[21,22] Well-nourished children will have the essential micro- and macronutrients (i.e. energy, fatty acids and protein) required for brain development and will also be better able to relate with their environment and caregivers and build on their experiences in ways that promote optimal development.[21]
Household SES was independently associated with child development at 5 years of age in both sexes, independent of growth status. Longitudinal studies across income settings describe family income and poverty status as more powerful predictors of children's IQ scores and behavioural development than maternal education, and associate poverty with developmental delays before 1 year of age, with deficits increasing at 5 years of age.[8,23] There is some evidence to suggest that these differences in cognitive performance between SES groups are smaller in more equitable societies.[24]
Maternal education itself has been shown to be a significant determinant of children's cognitive ability, educational performance and subsequent human capital.[1] Previous studies indicate that the effect of maternal education on a child's cognitive and behavioural development remains strong, even after accounting for SES and caregiving effects.[3,25] Although maternal education was positively associated with R-DPDQ scores among male children in this study the association was attenuated when SES and caregiving effects were controlled for. This suggests that, as shown previously, maternal education may influence child development through other pathways, such as particular parenting characteristics (e.g. caregiver warmth towards the child, maternal sensitivity and responsiveness, or the ability to provide a safe and stimulating environment for the child).[3,8]
This study found that growth between birth and 4 years of age partially mediated the relationship between maternal education (but not SES) and child development scores at 5 years of age. This is the first study in Africa to show this. Two earlier studies in low-income settings examined the extent to which child growth, including linear growth, mediated the effects of SES and maternal education on cognitive development.[7,8] A recent Colombian study found that height-for-age mediated the effect of SES on language development but not the effect of maternal education on cognitive development.[8] In contrast, our findings concur with those from a longitudinal study (using multiple measures of growth), conducted in rural Bangladesh, which showed that growth (particularly in the first two years of life) significantly mediated the association between maternal education and cognitive outcome in children at 5 years of age.[7]
A strength of this study is its use of prospective data from a longitudinal birth cohort in a low-resource setting to test associations, including biological and environmental factors, at the individual maternal and household level. Despite the data being from the early 1990s, the availability of sociodemographic information, repeated growth measures and subsequent child development assessments allows this specific research question to be explored in our context.
Study limitations
There are strong reciprocal interactions between cognitive and socio-emotional development, with changes in one potentially contributing to changes in the other.[26] Although the R-DPDQ instrument included some aspects of social and emotional child development, more in-depth exploration is needed of how growth and nutrition could influence behavioural development. The R-DPDQ is a screening tool and thus unable to assess specifics of any particular developmental construct. A useful addition to this study would be to further investigate the effects of social exposures and growth in early childhood on developmental outcomes using more definitive assessment tools. Although we were able to account for a variety of factors in the analysis, we lacked maternal IQ data. This would have strengthened the findings, as maternal IQ is a known moderator of child development.[1] The use of longitudinal data resulted in some participants being lost to inclusion after birth, with some differences noted in the retained sample (as outlined earlier). This reduces generalisability of the results, but, we believe, not in an important way
Conclusion
Early-life growth appears to affect child development outcomes differently in different settings, which can largely be explained by contextual factors such as poverty and parental education levels.[6-8]
This study provides evidence that early childhood growth (both before and after birth) was positively associated with development scores in children at 5 years of age. Furthermore, it offers encouragement that interventions targeting improved growth in the first few years of life could overcome some of the negative effects of lower maternal education on development outcomes of young children in a limited-resource African setting. Further research is needed to explore the appropriate timing and approach for interventions, such as integrated nutrition and development interventions, to optimise early childhood development outcomes in different contexts.
Declaration. None.
Acknowledgements. We thank the Bt20+ study participants and the research team for their contribution to this study.
Author contributions. WS, SN and LR were responsible for study conceptualisation. WS also handled data collection and interpretation, along with SN and IK, and wrote the manuscript. SN, IK, HS and LR contributed to critical review of the manuscript before submission. All authors approved the final manuscript for publication.
Funding. Financial assistance from the National Research Foundation (NRF) of South Africa is acknowledged (grant no. 84394). Opinions and conclusions are those of the authors and are not to be attributed to the NRF.
Conflicts of interest. None.
References
1. Walker SP, Wachs TD, Grantham-McGregor S, et al. Inequality in early childhood: Risk and protective factors for early child development. Lancet 2011;378:1325-1338. https://doi.org/10.1016/S0140-6736(11)60555-2 [ Links ]
2. Richter LM, Daelmans B, Lombardi J, et al. Investing in the foundation of sustainable development: Pathways to scale up for early childhood development. Lancet 2017;389:103-118. https://doi.org/10.1016/S0140-6736(16)31698-1 [ Links ]
3. Walker SP, Wachs TD, Meeks Gardner J, et al. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007;369:145-157. https://doi.org/10.1111/jcpp.12247 [ Links ]
4. Rutter M. Protective factors in children's responses to stress and disadvantage. Ann Acad Med Singapore 1979;8:324-338. [ Links ]
5. Stewart CP, Iannotti L, Dewey KG, Michaelsen KF, Onyango AW Contextualising complementary feeding in a broader framework for stunting prevention. Matern Child Nutr 2013;9:27-45. https://doi.org/10.1111/mcn.12088 [ Links ]
6. Huang C, Martorell R, Ren A, Li Z. Cognition and behavioural development in early childhood: The role of birth weight and postnatal growth. Int J Epidemiol 2012;42:160-171. https://doi.org/10.1093/ije/dys207 [ Links ]
7. Hamadani JD, Tofail F, Huda SN, et al. Cognitive deficit and poverty in the first 5 years of childhood in Bangladesh. J Pediatr 2014;134:el001-el008. https://doi.org/10.1542/peds.2014-0694 [ Links ]
8. Rubio-Codina M, Attanasio O, Grantham-McGregor S. Mediating pathways in the socio-economic gradient of child development: Evidence from children 6-42 months in Bogota. Int J Behav Dev 2016;40:483-491.https://doi.org/10.1177/0165025415626515 [ Links ]
9. Richter L, Norris S, Pettifor J, Yach D, Cameron N. Cohort profile: Mandela's children: The 1990 Birth to Twenty study in South Africa. Int J Epidemiol 2007;36:504-511. https://doi.org/10.1093/ije/dym016 [ Links ]
10. Frankenburg WK, Fandal AW, Thornton SM. Revision of Denver Prescreening Developmental Questionnaire. J Pediatr 1987;110:653-657. [ Links ]
11. Griesel R, Belciug M, Richter L. The predictive value of the Denver Prescreening Developmental Questionnaire: An investigation of the concurrent validity of three developmental scales. Pretoria: University of South Africa, 1985. [ Links ]
12. Hsiao C, Richter LM. Early mental development as a predictor of preschool cognitive and behavioral development in South Africa: The moderating role of maternal education in the Birth to Twenty cohort. Infants Young Child 2014;27:74-87. [ Links ]
13. Filmer D, Scott K. Assessing asset indices. Demography 2012;49:359-392. https://doi.org/10.1007/s13524-011-0077-5. [ Links ]
14. Sheppard ZA, Norris SA, Pettifor JM, Cameron N, Griffiths PL. Approaches for assessing the role of household socioeconomic status on child anthropometric measures in urban South Africa. Am J Hum Biol 2009;21:48-54. https://doi.org/10.1002/ajhb.20814. [ Links ]
15. WHO Multicentre Growth Reference Study Group. WHO child growth standards: Methods and development. Geneva: World Health Organization. 2006. [ Links ]
16. Stein AD, Wang M, Martorell R, et al. Growth patterns in early childhood and final attained stature: Data from five birth cohorts from low- and middle-income countries. Am J Hum Biol 2010;22:353-359. https://doi.org/10.1002/ajhb.20998. [ Links ]
17. Gunzler D, Chen T, Wu P, Zhang H. Introduction to mediation analysis with structural equation modeling. Shanghai Arch Psychiatry 2013;25:390. https://doi.org/10.3969/j.issn.1002-0829.2013.06.009. [ Links ]
18. Kuklina EV, Ramakrishnan U, Stein AD, Barnhart HH, Martorell R. Early childhood growth and development in rural Guatemala. Early Hum Dev 2006;82:425-433. https://doi.Org/10.1016/j.earlhumdev.2005.10.018. [ Links ]
19. Yang S, Tilling K, Martin R, Davies N, Ben-Shlomo Y Kramer MS. Pre-natal and post-natal growth trajectories and childhood cognitive ability and mental health. Int J Epidemiol 2011;40:1215-1226. https://doi.org/10.1093/ije/dyr094. [ Links ]
20. Piwoz E, Sundberg S, Rooke J. Promoting healthy growth: What are the priorities for research and action? Adv Nutr 2012;3:234-241. https://doi.org/10.3945/an.lll.001164. [ Links ]
21. Prado EL, Dewey KG. Nutrition and brain development in early life. Nutr Rev 2014;72:267-284. https://doi.org/10.1111/nure.12102. [ Links ]
22. Cusick SE, Georgieff MK. The role of nutrition in brain development: The golden opportunity of the "first 1000 days". J Pediatr 2016;175:16-21. https://doi.org/10.1016/j.jpeds.2016.05.013. [ Links ]
23. Fernald LC, Weber A, Galasso E, Ratsifandrihamanana L. Socioeconomic gradients and child development in a very low income population: Evidence from Madagascar. Dev Sci 2011;14:832-847. https://doi.org/10.1073/pnas.1121241109. [ Links ]
24. Adler NE, Ostrove JM. Socioeconomic status and health: What we know and what we don't. Ann NY Acad Sci 1999;896:3-15. https://doi.org/10.1111/j.1749-6632.1999.tb08101.x. [ Links ]
25. Bradley RH, Corwyn RF. Socioeconomic status and child development. Annu Rev Psychol 2002;53:371-399. https://doi.org/10.1146/annurev.psych.53.100901.135233. [ Links ]
26. Pollitt E. A critical view of three decades of research on the effects of chronic energy malnutrition on behavioral development. In: Schurch B, Scrimshaw NS. eds. Chronic Energy Deficiency: Consequences and Related Issues. Lausanne: International Dietary Energy Consultancy Group, 1988:77-94. [ Links ]
 Correspondence:
Correspondence:
W Slemming
Wiedaad.Slemming@wits.ac.za
Accepted 11 October 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}