










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.16 n.2 Pretoria Jun. 2022
http://dx.doi.org/10.7196/sajch.2022.v16i2.1878
RESEARCH
Infant injuries treated at Red Cross War Memorial Children's Hospital, Cape Town, South Africa
K K StormI; M van DijkII; A B van AsIII
IMD; Department ofPaediatric Surgery, Erasmus MC-Sophia Childrens Hospital, Rotterdam, The Netherlands
IIPhD; Department ofPaediatric Surgery, Erasmus MC-Sophia Childrens Hospital, Rotterdam, The Netherlands
IIIFCS(SA), PhD; Department of Paediatric Surgery, Red Cross War Memorial Children's Hospital, and Department of Paediatrics and Child Health, University of Cape Town South Africa
ABSTRACT
BACKGROUND: Infants are entirely dependent on their caregivers, especially <6 months old when they are not yet mobile. While the epidemiology of injury among children in general has been described, the exact causes of infant injury have never been investigated in South Africa (SA
OBJECTIVE: To describe causes of injury in infants aged <12 months, stratified for the four quarters of the first year of life, in order to identify opportunities for targeted prevention strategies based on local data
METHODS: This retrospective audit study used data collected by ChildSafe SA from the Red Cross War Memorial Children's Hospital in Cape Town, SA, over a 4-year period from January 2013 to December 2016. Infants <1 year of age presenting to the hospital's trauma casualty department were included. Additionally, mortuary data on traumatic infant deaths in the hospital's catchment area were collected.
RESULTS: A total of 2 279 injured infants were identified. More than half were male (55%; n=1250) and the median age was 8 months (interquartile range 5-10 months). Leading causes of injury were falls (42%; n=957) and burns (32%; n=736). A significant association between the age group and the cause of injury (p<0.001) was found. From 2014 to 2016, an additional 27 infants were traumatically injured and died before arriving at the hospital
CONCLUSION: Falls and burns are a significant contributor to the burden of infant injuries in Cape Town. This underlines the urgent need for targeted prevention strategies to improve safety, taking poverty into account
Trauma injury has a great impact on people's health, but children up to the age of 1 year are especially vulnerable[1,2] owing to their immature anatomy, skeletal composition, cardiovascular performance and drug metabolism. Falls - from a bed, couch, baby equipment or the arms of a caregiver - are the leading cause of injury in children <1 year old.[3,4] Burns are a second major cause of injury in infants. In Africa, the annual incidence of fire-related burns in children <1 year old is 35 per 100 000. This is more than three times the world average for this age group. Other known causes of injury in infants are interpersonal violence/assault, traffic crashes, poisonings and choking.[5-7] Most injuries occur at home, often as a consequence of household hazards such as loose hanging kettle cables and beds without safety bars, lack of supervision, as well as the increased mobility of older infants.[4,7,8]
Infants <6 months old are largely pre-mobile and dependent on their caregivers. When aged 6-12 months, they develop the ability to crawl, roll and eventually walk, and are then at greater risk for injury Even though injuries in children <1 year old account for only 2% of all injuries in children in low- and middle-income countries (LMICs), unintentional injury death rates in this age category are highest when compared with the older age groups.[2,3] The infant death rate from burns is highest in LMICs: 11 per 100 000 population.[3] Standard age groupings for paediatric injury research have been developed.[3,9] In most studies, however, children <12 months of age are taken as one group. Unfortunately, this practice may mask age-related injury trends in infants.
While the epidemiology of injury among children in general has been described, causes of infant injury have never been validly investigated in South Africa (SA). Insight into the leading causes of injury specified for different stages of the first year of life can help to develop interventions to prevent injury.[6,10] This study aims to describe causes of injury in children <12 months admitted to the trauma casualty department of the Red Cross War Memorial Childrens Hospital (RCWMCH) in Cape Town, SA, stratified for different age groups.
Methods
Study design
This is a retrospective, descriptive audit study.
Patients and setting
ChildSafe SA is an independent non-governmental organisation, established in 1978 (www.childsafe.org.za). Since 1991, ChildSafe SA has systematically kept a computerisedchildhoodtrauma surveillance system of all injured children presenting to the RCWMCH trauma unit, which serves as a national information system for childhood injuries in SA. Funding is provided by numerous donors.
We analysed available data of children <1 year old (365 days) seen between January 2013 and December 2016. Ethical approval was obtained from the Human Research Ethics Committee, University of Cape Town Faculty of Health Sciences (ref. no. 239/2018). No recruitment or informed consent was necessary as this is a retrospective study.
Data collection
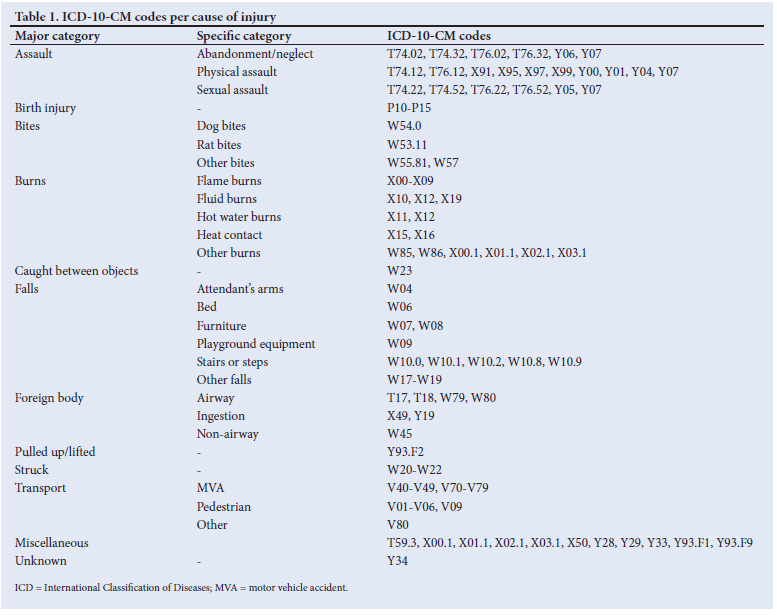
ChildSafe has developed a data collection form that consists of six major domains: (i) patient demographics; (ii) cause of injury; (iii) place of occurrence; (iv) severity of injury; (v) suspicion of abuse; and (vi) discharge destination. This ChildSafe form is completed by the attending physician for every child presenting at the trauma casualty department of the RCWMCH. The causes of injury are classified as assault, birth injury, bites, burns, caught [between objects], falls, foreign bodies, pulled up /lifted, struck, transport, miscellaneous or unknown. We translated the different causes of injury into ICD-10-CM codes for external causes of morbidity and mortality according to the International Classification of Disease. The ICD-10-CM codes classified under the main causes of injury are shown in Table 1. The place of occurrence contains the following options: own home; road/pavement; other home; public place; school/creche; sport; other; and unknown.
The severity of injury is classified with the use of the RCWMCH's four-point abbreviated injury score (AIS) as 'mild', 'moderate', 'severe' or 'mortal'.[11] Suspicion of abuse is represented by the abuse code on the ChildSafe form, and is classified as 'no abuse', 'possible abuse' or 'abuse'.
All variables were checked for missing or incorrect values in the database. If missing or incorrect values were identified, additional information was obtained from the medical records and processed in the database by the principal investigator (KKS). For the analysis we created four age groups (0-2 months old, 3-5 months old 6-8 months old and 9-11 months old), corresponding with the different levels of child development and mobility.
Mortuary data on traumatic infant deaths (<1 year old) in the hospital's catchment area for the study period were collected from the University of Cape Town Division of Forensic Medicine and Toxicology. This way we additionally included fatal injuries in which the infant did not make it to the hospital. Collected data included cause of injury and manner of death (intentional v. non-intentional) in infants who had died before arrival at the hospital.
Outcomes
The primary outcome is cause of injury. Secondary outcomes are place of occurrence, severity of the injury and the nature of fall injuries and burn injuries.
Data analysis
Normally distributed variables are presented as mean (standard deviation), and non-normally distributed variables as median (interquartile range (IQR)). Descriptive statistics (frequencies and cross-tabulations) were used to characterise injuries by cause for each age group. Age-related injury patterns were compared with published norms for child growth and development. Differences in categorical variables between age groups were tested with x2 or Fisher's exact tests, as appropriate. If exact test was not computable, we applied Monte Carlo. A p-value <0.05 was considered statistically significant. All data management was conducted in Excel (Microsoft Corp., USA) and statistical analyses were performed in SPSS for Windows, version 24.0 (IBM SPSS Statistics, USA).
Results
According to the trauma surveillance registry, 2 279 infants < 1 year old presented at the RCWMCH's trauma casualty department between January 2013 and December 2016. Table 2 gives the background characteristics of this patient group. More than half were male (55%; n=l 250) and the median age was 8 months (IQR 5 - 10).
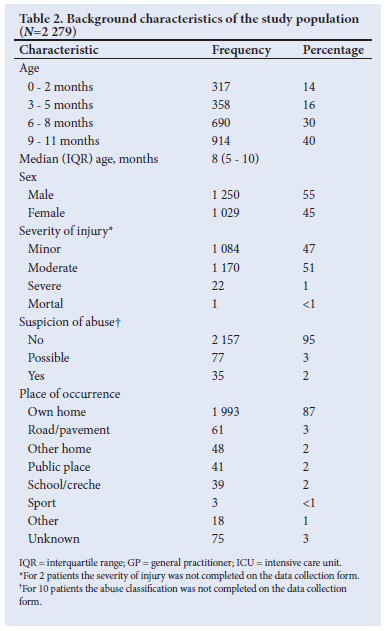
Most injuries were classified as moderate (51%; n=1170) or minor (47%; n=1084). Burn injuries in particular were frequently classified as moderate (83%; n=614). One infant had died at the trauma casualty department and therefore scored 'mortal' on the AIS. This was a 9-month-old female with a gunshot wound in her head.
Causes of injury
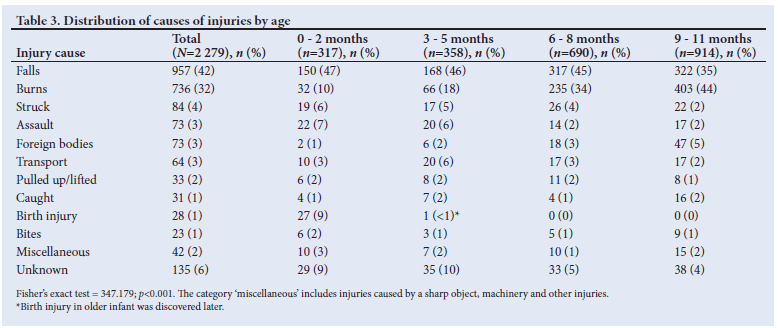
Table 3 provides details of the occurrences of the various causes of injury for the total group and the different age groups. Falls were the most frequent cause of injury, comprising 42% (n=957) of all injuries. This holds true for the three youngest age categories as well. The proportions of falls in the three youngest age groups were comparable, but in the oldest age group this proportion was lower than that in the three youngest age groups. In the oldest age group, burns were the most common injury (44%). Of all injuries, 70% had occurred in the two oldest age groups (n=1604). A significant association between the age group and the cause of injury (p<0.001) was found, in that assault was more frequent in younger infants. Older infants were more likely to be injured from burns and foreign bodies or caustic ingestion. In the two youngest age groups, the cause of injury was more likely to be unknown than in the two oldest age groups.
Falls
Falls from bed accounted for almost half of the fall injuries (49%; n=471). Other common types of fall were falls from attendants' arms (16%; n=154), falls from toy devices or playground equipment (8%; n=76), falls from stairs (6%; n=56) and falls from furniture (4%; n=38). The remaining 17% were defined as 'other falls' (n=162), consisting of falls while trying to walk or stand, falls out of car seats and unknown mechanisms of falls. Fig. 1 shows the distribution of age groups among the different types of falls. There was a significant association between the type of falls and the age groups (p<0.001), in that infants <6 months were more often dropped out of the attendant's arms, and older infants endured a greater number of other fall types. Of all falls, 22% led to a fracture (n=210), and 86% of the falls occurred inside the infant's own home (n=823).
Burns
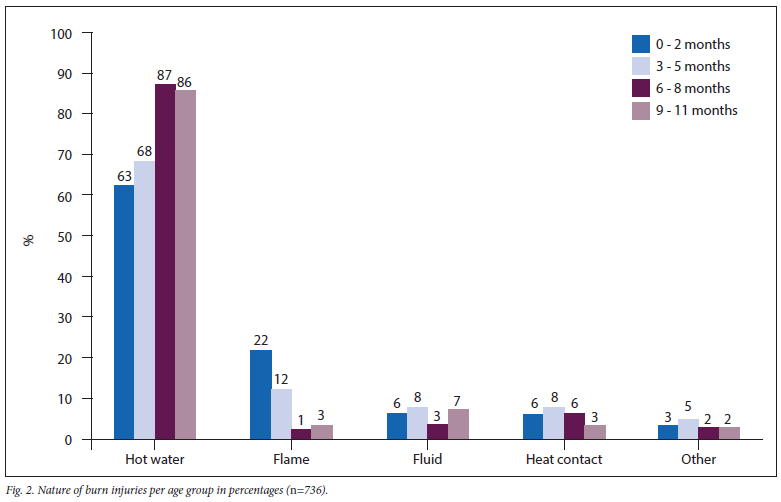
Burn injuries were the second-most common cause of injury in the total group (32%; n=736), and were more often seen in male than in female infants (p=0.007). Burn injuries occurred more frequently in the two older age groups (p<0.001): the proportion of burn injuries increased from 10% in the youngest age group to 44% in the oldest age group. Hot water burns contributed to over 80% of all burns (84%; n=615). The distribution of age groups among the different types of burns is seen in Fig. 2. Burns were in most cases (95%) sustained at home.
Other injuries
Eighty-four infants were injured due to being struck (4%) (Table 3). Of these 84 cases, 43 (51%) resulted in tissue damage such as abrasions, lacerations and closed tissue injuries.
Of the 73 assaulted infants, 60 (82%) were physically assaulted; 10 (14%) sexually assaulted and 3 (4%) abandoned or neglected. There was a significant association between assault and age group (p<0.001), in that assault was mostly seen in the two youngest age groups. In addition, females were more frequently victims of sexual assault, whereas physical assault was seen more often in males (p=0.019).
Injuries due to foreign bodies or caustic ingestion occurred significantly more often in infants >6 months of age (p<.001).
In the foreign body cases, airway foreign bodies (59%; n=43) were more common than non-airway foreign bodies (22%; n=16). Ingestion occurred in 13 cases (19%).
The most common transport-related injuries were motor vehicle crashes (72%; n=46). Seventeen infants were injured as pedestrians (27%).
In 23 cases (70%) of all infants who were injured by being pulled up or lifted, this resulted in an elbow injury. Dislocations were mostly caused by lifting up an infant (42%; n=14).
Being caught between two things was the cause of injury in 31 infants (1%).
Birth was the cause of injury in 30 cases, accounting for 1% of all injuries.
The 32 bites were classified as rat bites (n=10; 44%), dog bites (n=7; 30%), human bites (n=2; 9%) and other bites (n=4; 17%).
Cases were grouped under miscellaneous if the injury was caused by a sharp or a blunt object, massage, washing, crawling, pepper spray or smoke inhalation.
Mortuary data
Mortuary data on infants in 2013 were missing. Over the years 2014 - 2016, a total of 27 infants <1 year of age died before arrival in the hospital. Of the deceased infants, 14 (52%) were <6 months and 13 (48%) were >6 months of age. The related causes of injury in these infants were assault (30%; n=8), drowning (26%; n=7), burns (26%; n=7), road traffic accidents (7%; n=2), choking (7%; n=2) and falls (4%; n=1). Eighteen died unintentionally and 9 were murdered. The methods of murder were assault in 8 cases and drowning in 1 infant.
Discussion
The aim of this study was to describe the characteristics of injuries in children <1 year old in Cape Town, SA. We found that most injured infants were >6 months of age. The following may serve as an explanation: with increasing age, the child's mobility gradually advances from being only able to roll over at 4 months, but sit up at 6 months, pull up to a standing position at 9 months and eventually start walking at the age of 12 months.[12]
Previous research into paediatric injuries found that two-thirds of injuries were of minor severity in children aged <13 years.[10] Strikingly, the severity of more than half of the injuries in the present study was classified as moderate. This suggests that infants <1 year of age are more likely to be injured more seriously after experiencing a trauma than children of other ages.
Falls
Between 2013 and 2016, falls were the most frequent cause of injuries in infants presenting to the RCWMCH, and were the leading cause of injury in infants aged <9 months. Other research likewise cites falls as the most common cause of paediatric injury.[2,7,13] Owing to infants' rapid growth and developmental changes, the frequency and mechanism of falls change with increasing age. A higher proportion of children >6 months of age presented to the trauma unit as a result of falls. In previous research, younger children were found to be more likely to be dropped from a caregivers arms or to fall from furniture. [12] Our findings support this, and suggest that infants <6 months of age are at particular risk of being dropped. Parents should therefore be educated about the fast development of mobility in infants, to create more awareness of the hazards in the infants first year of life.
It is striking that even though infants <3 months old are usually not able to roll over, almost half of the infants aged 0-2 months who had experienced a fall were reported to have fallen out of bed. This raises some serious concerns about the veracity of the history provided, and should be considered a marker for child abuse until proven otherwise. It will help to educate providers that (i) inconsistent and developmentally implausible history and (ii) injury pattern requiring mobility in a non-mobile child are highly suspicious for child abuse.
In concordance with our study, other research has also indicated that the majority of non-fatal fall injuries occur in the home environment. [10] The significant burden of fall injuries highlights the urgent need for targeted interventions to improve the safety of infants, especially within the home. Mechanisms of falls are highly dependent on context, but in SA there is currently a lack of evidence-based research on risk factors and effective interventions to prevent falls in this specific age group. In the search for effective prevention strategies, poverty should be taken into account, since social class and childhood falls have shown a strong relationship.[3] Not only are not all interventions applicable in poor-quality housing, but also, in poor families, children are more often left unsupervised.[3]
Burns
The second leading cause of injury in the present study was burns. We found a predominance of burn injuries in males compared with females. Previous research conducted in SA showed the same predominance,[9] but in the global literature burns occur more often in females. Similarly to the global literature,[3] our study found that most burns had been sustained in the home environment. Flame burns were more frequently seen in the youngest age groups, while hot water burns occurred more frequently in infants >6 months old. Overall, hot water burns accounted for most of the burn injuries in infants. The increased vulnerability for burns with older age can be explained by the fact that when a child is able to stand upright, (s)he can more easily reach for hot objects and loose hanging kettle cables.
Strengths and limitations
A strength of this study is the distinction made between different age groups. Where other research used standard age groupings for paediatric injury, and infants <1 year of age are taken as one group, we were able to relate injuries to the level of development. This way we reduced the risk of masking small injury trends. Another strength is the use of mortuary data on traumatic infant deaths, which has increased the accuracy of the results.
A possible limitation of this study is the severity of injury assessment. We have tried to standardise severity assessment through the use of the RCWMCH's AIS,[1l] yet the severity of injury might have been subjectively assessed in some cases owing to the time pressure associated with high emergency. Also, by using this RCWMCH's modified AIS, this study is limited in comparing the severity of injury with that in studies from other settings.
A further limitation is that RCWMCH's trauma registry does not follow admitted children through the course of their hospitalisation. All data collected pertained to the injured child's stay in the trauma casualty department. Outcome data, including mortality, morbidity and hospital length of stay, were therefore not available.
A final limitation of this study is the lack of information about abuse. The abuse code was collected from the ChildSafe form, which is routinely completed at the moment the child presents to the trauma unit of the RCWMCH. At that point in time, the provision of adequate healthcare is the priority, and signs and signals of abuse may be overlooked at that stage. Besides, the abuse code only indicates whether abuse was suspected at the moment of completing the ChildSafe form, not if abuse was actually confirmed. Therefore, the abuse code does not seem a reliable tool to investigate abuse in infants. Future in-depth research into determinants predicting abuse in infants is necessary.
Conclusion
The most likely causes of injury in infants <1 year of age seen in the trauma casualty department are falls or burns. The significant burden of these injuries emphasises the urgent need for targeted prevention strategies to improve infants' safety, especially within the home. Parents should be educated about the fast development of mobility in infants and the milestones they will reach in their first year of life. Interventions should be devised that take poverty into account. Findings also suggest that abuse is under-recognised: more research into determinants that predict child abuse in a standardised way is necessary. The use of a screening tool at the trauma unit should be considered.
Declaration. This study was completed as part of KKS's MMed, but changes have been made since submission.
Acknowledgements. We are grateful to ChildSafe SA (www.childsafe.org.za) for providing the data for this study.
Author contributions. All authors made substantial contributions to all of the following: (i) the conception and design of the study, or acquisition of data, or analysis and interpretation of data; (ii) drafting the article or revising it critically for important intellectual content; and (iii) final approval of the version to be submitted.
Funding. None.
Conflicts of interest. None.
References
1. Tracy ET, Englum BR, Barbas AS, Foley C, Rice HE, Shapiro ML. Pediatric injury patterns byyear of age. J Pediatr Surg 2013;48(6):1384-1388. https://doi.org/10.1016/j.jpedsurg.2013.03.041 [ Links ]
2. Agran PF, Anderson C, Winn D, Trent R, Walton-Haynes L, Thayer S. Rates of pediatric injuries by 3-month intervals for children 0 to 3 years of age. Pediatrics 2003;111(6Pt 1):e683-692. https://doi.org/10.1542/peds.llL6.e683 [ Links ]
3. Peden MOK, Ozanne-Smith J, Hyder AA, et al. World report on child injury prevention. Geneva: World Health Organization, 2008. [ Links ]
4. Mulligan CS, Adams S, Tzioumi D, Brown J. Injury from falls in infants under one year. J Paediatr Child Health 2017;53(8):754-760. https://doi.org/10.llll/jpc.13568 [ Links ]
5. Isaac KN, Van Niekerk A, Van As AB. Child road traffic crash injuries at the Red Cross War Memorial Children' Hospital in Cape Town, South Africa in 1992, 2002 and 2012. Int J Inj Contr Saf Promot 2015;22(4):352-358. https://doi.org/10.1080/17457300.2014.912236 [ Links ]
6. BradshawCJ, Bandi AS, Muktar Z, et al. International study of the epidemiology of paediatric trauma: PAPSA research study. World J Surg 2018;42:1885-1894. https://doi.org/10.1007/s00268-017-4396-6 [ Links ]
7. Pickett W, Streight S, Simpson K, Brison RJ. Injuries experienced by infant children: A population-based epidemiological analysis. Pediatrics 2003;111(4 Pt 1):e365-370. https://doi.org/10.1542/peds.HL4.e365 [ Links ]
8. Laitakari E, Pyorala S, Koljonen V. Burn injuries requiring hospitalisation for infants younger than 1 year. J Burn Care Res 2012;33(3):436-441. https://doi.org/10.1097/bcr.0b013e31823359c4 [ Links ]
9. Wesson HK, Bachani AM, Mtambeka P, et al. Pediatric burn injuries in South Africa: A 15-year analysis of hospital data. Injury 2013;44(11):1477-1482. https://doi.Org/10.1016/j.injury.2012.12.017 [ Links ]
10. Herbert HK, van As AB, Bachani AM, et al. Patterns of pediatric injury in South Africa: An analysis of hospital data between 1997 and 2006. J Trauma Acute Care Surg 2012;73(1):168-174. https://doi.org/10.1097/ta.0b013e31824d67c3 [ Links ]
11. Salverda M, Ketharanathan N, Van Dijk M, et al. A review of blood transfusions in a trauma unit for young children. S Afr Med J 2017;107(3):227-231. https://doi.org/10.7196/samj.2017.vl07i3.11307 [ Links ]
12. Chaudhary S, Figueroa J, Shaikh S, et al. Pediatric falls ages 0-4: Understanding demographics, mechanisms, and injury severities. Inj Epidemiol 2018;5(Suppl 1):S7. https://doi.org/10.1186/s40621-018-0147-x [ Links ]
13. Wesson HKH, Bachani AM, Mtambeka P, et al. Changing state of pediatric injuries in South Africa: An analysis of surveillance data from a Pediatric Emergency Department from 2007 to 2011. Surgery 2017;162(6S):S4-S11. https://doi.Org/10.1016/j.surg.2017.03.019 [ Links ]
 Correspondence:
Correspondence:
KK Storm
stormkelly@outlook.com
Accepted 31 May 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}