










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.16 no.2 Pretoria Jun. 2022
http://dx.doi.org/10.7196/sajch.2022.v16.i2.1822
SHORT REPORT
South Africa regains polio-free status: Processes involved and lessons learnt
J C Y NyasuluI, II; R MaphotoIII; M G S KamupiraIV; N MsomiV
IPhD; Division of Community Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; AFRIQUIP, Health Systems Strengthening, Johannesburg, South Africa
IIIMMed; Child, Youth and School Health, National Department of Health, Pretoria, South Africa
IVPhD; World Health Organization, Pretoria, South Africa
VPhD; Department of Virology, School of Laboratory Medicine and Medical Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
The World Health Organization recommends continuous immunisation coverage and polio surveillance standards for countries to sustain a polio-free status. We highlight experiences and lessons learnt by South Africa (SA) in losing - and subsequently regaining - its polio-free status. Following some decline in achieving acute flaccid paralysis surveillance and immunisation coverage targets, SA had its polio-free status withdrawn in 2017. Existing gaps were addressed and the polio-free status was regained in 2019. Lessons learnt from this experience include reaffirming the importance of continued commitment to polio eradication efforts, strengthening health systems through quality improvement projects, ensuring accountability in supervision, and monitoring of polio-related indicators. Consistent political commitment, collaboration and accountability are critical in sustaining the country's health programmes, including maintaining a polio-free status and closing identified gaps.
Poliovirus is the main infectious cause of disability worldwide, with millions of children disabled globally, including in Africa.[1] Poliomyelitis is preventable through effective vaccination coverage, which has existed for decades.[2] Efforts across the world to eradicate the disease have taught us several lessons so far.[3]
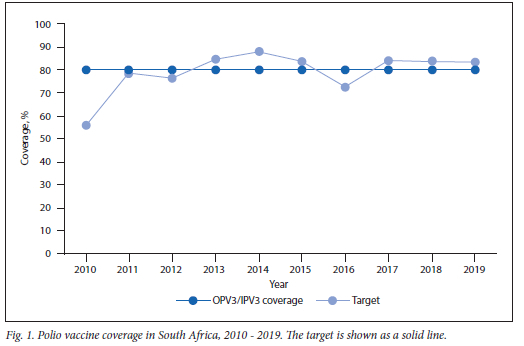
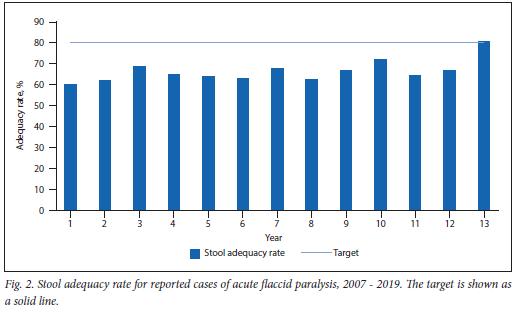
The key goal of the Global Polio Eradication Initiative (GPEI) in the new 2019 - 2023 Polio Endgame strategy is for countries to achieve polio-free certification.[4] For a country to be given a polio-free status by the World Health Organization (WHO), it needs to achieve the following minimum targets: >80% oral poliovirus vaccine (OPV) immunisation coverage; maximum 2/100 000 cases of non-polio acute flaccid paralysis (AFP) in the population younger than 15 years old per year; and >80% stool adequacy rate for reported AFP cases. [5] By 2017, Nigeria was the only African country where poliovirus remained endemic;[6] in 2020, it was declared to be polio free. This led to regional polio certification, which was a remarkable and significant achievement and a testament to the commitment of key partners in providing the much-needed resources and better implementation of strategies.[7]
To retain certification, a country with polio-free status is expected to maintain a sensitive AFP surveillance system with a robust poliovirus outbreak preparedness and response plan and a high population immunisation coverage against the virus, as well as robust containment activities.[5] In Africa, this is monitored by an independent body of experts, namely the African Region Certifications Committee (ARCC), who review annual progress reports from the various national certification committees.[8] The ARCC reserves the right to withdraw or rescind a countrys polio-free status if the country's performance is suboptimal.[9] South Africa (SA) is the only country in the African region that has lost - but subsequently regained - its polio-free status owing to suboptimal performance in maintaining the outlined WHO standards.[10] In this report, we describe the SA experience and the lessons learnt.
Withdrawal of South Africa's polio-free status
SA had its last wild polio case in 1989 and received the initial polio-free status in 2006,[10,11] with annual progress reports submitted to the ARCC from then on. Between 2015 and 2017, a constant decline was reported in full poliovirus immunisation coverage (based on administration of the third dose of either the inactivated polio vaccine (IPV) or the OPV, with the lowest performance at 72.5% in 2016. This was lower than the national target of 80% and occurred at the time of a global shortage of the hexavalent vaccine.[12] During this period, there was generally a low immunisation coverage, which resulted in low population immunity in SA, leading to outbreaks of other vaccine-preventable diseases.[13} In addition, the country has reported suboptimal performance in stool adequacy rates since 2006, with a figure of 64.2% reported by 2017.[12]
The decline in immunisation coverage in SA between 2015 and 2017, especially of the OPV3/IPV3, indicated that the immunisation coverage levels for the country were not high enough to prevent imported wild poliovirus from circulating, with the possible re-emergence of poliomyelitis.[12] In addition, AFP surveillance and stool adequacy rates consistently below 80% reflected poor AFP case reporting and investigation, indicating that the surveillance system in SA was not sensitive and would be unable to detect poliovirus importation should it occur. The national certification committee raised these concerns in their annual ARCC progress reports and the country's polio-free status was consequently withdrawn in December 2017.[14]
How did South Africa regain its polio-free status?
SA realised the need to take action, address the gaps and change the situation. These were accomplished through putting in place measures such as polio eradication advocacy initiatives, strengthening immunisation systems through quality improvement interventions, redefining polio eradication efforts, closely monitoring immunisation and polio surveillance, and improving collaborative efforts.
The country had two advocacy visits from the ARCC and the WHO African region. Meetings held with the national and provincial health ministers led to the health department officially committing to polio eradication efforts.[14] This involved a national advocacy memorandum to improve the polio surveillance indicators and a special appeal to prioritise polio eradication with a focus on the worst-performing provinces. [15] In addition, the national certification committee and other polio committee members used existing platforms, such as institutional academic meetings, to advocate for and support the process of addressing the existing gaps.
The national Department of Health's Expanded Programme on Immunisation (EPI) unit, with support from the national Maternal and Child Health Department and the WHO secretariat, conducted provincial workshops for maternal and child health managers and all involved in polio eradication services. These workshops focused on sensitising the provinces to the poor performance, identifying reasons for poor performance, and developing quality improvement plans at district and provincial level. Appropriate resources were subsequently allocated for provinces to meet their demands, which also strengthened their collaboration with the national health department and other partners such as the WHO country office, UNICEF and the National Institute for Communicable Diseases. Poor-performing provinces received individualised support from national and provincial managers and partners such as the WHO and UNICEF. Progress on implementation of quality improvement interventions at district level was presented quarterly and, in return, technical input was given to implementers. In addition, SA had rolled out the use of the integrated supportive supervision tool on the open data kit since April 2018. The open data kit has shown to improve surveillance recording[16] and since its implementation, most of the active-case search and surveillance supervision visits were documented.
It is important to ensure that poliovirus samples and infectious materials (including potentially infectious materials) in laboratories are handled according to the requirements of the Global Action Plan III to Minimise Poliovirus to prevent the virus from being reintroduced into the population and environment.[17] To this end, SA completed the process of laboratory surveys and documentation of the presence or absence of infectious and potentially infectious materials, with support from the WHO.
Environmental surveillance for poliovirus monitors the transmission of poliovirus among human populations by examining specimens in the environment that are contaminated by human faeces.[18] The ARCC recommended that SA establish an environmental surveillance programme, which was subsequently rolled out (in 2019) to three metropolitan areas, namely City of Ekurhuleni, City of Johannesburg and City of Tshwane. In addition, the country developed a polio outbreak preparedness and response plan in line with the WHO standard operating procedures for any polio outbreak or event, which resulted in two immune-deficient, vaccine-derived poliovirus cases successfully being detected, investigated and managed.[14]
Results
Collaborative efforts in addressing polio eradication gaps resulted in positive progress on various polio immunisation and surveillance indicators.
Polio immunisation coverage
An increase in polio immunisation coverage, exceeding the 80% target, was observed between 2016 and 2018 (Fig. 1).
Stool adequacy rate for reported cases of acute flaccid paralysis
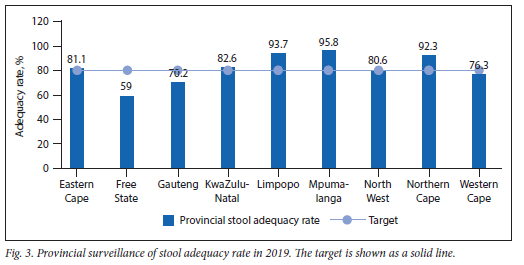
Fig. 2 summarises the analysis of AFP surveillance data since SA was certified polio free. At a national level, SA has been performing below the 80% target for stool adequacy rate since 2007. The initiatives to regain the country's polio-free status have shown to improve the indicator, with the rate exceeding the 80% target for the first time in 2019. Even though the performance was above target at national level, some provinces (Free State, Gauteng and the Western Cape) were still below target (Fig. 3).
Feedback on results
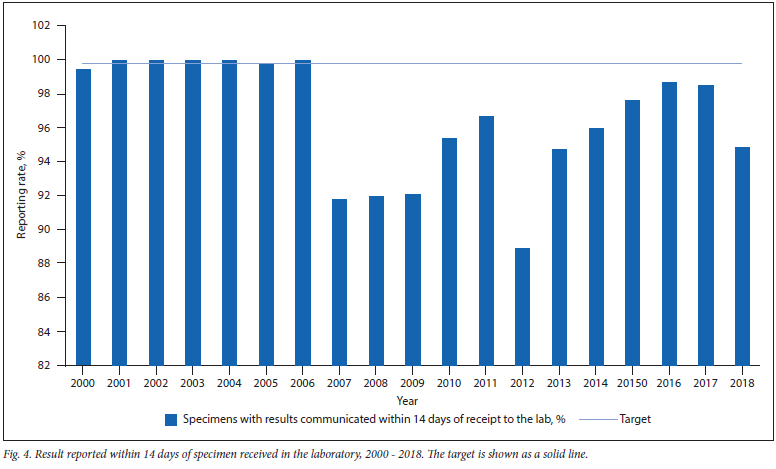
In addition to the 80% stool adequacy target, the National Institute for Communicable Diseases requires that 80% of all results be reported within 14 days of receipt from the laboratory. Gaps have existed since 2000 (Fig. 4).
Non-polio acute flaccid paralysis surveillance rate
Surveillance of non-polio AFP among children younger than 15 years reflects the sensitivity of the polio surveillance system. The WHO recommends that 2 cases per 100 000 of the population in this age group should be detected annually for a country to qualify for polio-free certification.[5] However, as SA has been performing above the minimum WHO standard, a higher benchmark was set by the country, namely 4 cases of non-polio AFP in 100 000 of the target population detected annually.
SA has consistently performed above the WHO target (except in 2007 and 2010), with the best performance in 2019 (Fig. 5). The intiatives put in place since 2017 have contributed to a steady improvement in surveillance performance.

National recommendation and documentation report
In response to the progress in the surveillance, immunisation coverage and containment indicators between 2017 and 2019, the national certification committee prepared a report to motivate for the certification of polio eradication in the country. In this report, the committee expressed confidence that the country was able to achieve and sustain routine immunisation and surveillance targets and recommended that the ARCC declare SA polio free. The report was followed by a verification visit by ARCC and WHO Africa representatives (see Fig. 6).
During the visit, the draft report was thoroughly reviewed and verified, which included facility visits to priority provinces, and feedback and recommendations were offered to address gaps. The final report was presented to the ARCC at a meeting held in Lusaka, Zambia, on 16 - 20 September 2019, where the regional committee accepted the SA recommendation and declared the country polio free. Further recommendations were included as part of the acceptance.[14]
Lessons learnt
Key lessons learnt from the SA experience are as follows:
1. Once polio-free status is achieved, continued effective leadership and commitment to polio eradication efforts are needed to ensure sustainability of polio surveillance.
2. Programmes shown to yield good results should be integrated to use resources optimally. For example, a campaign that focused on increasing demand for vaccination among under-5s was used as a platform to raise awareness about polio eradication.[19]
3. Commitment by political leaders and high-level advocacy contributed to resource mobilisation, motivating and inspiring implementation at all levels.
4. Strengthening health systems through quality improvement approaches was helpful in developing tailored district and provincial activities.
5. Collaboration by the national Department of Health, WHO, UNICEF, National Institute for Communicable Diseases, polio committees and provincial structures in providing technical support and mobilising resources to address the gaps was key in achieving the goal.
6. Through the collaborative efforts of the Department of Health and its partners demand for improved immunisation coverage increased and understanding of measles and AFP case definition was improved at the community level. This was done through aligning with campaigns that target national, regional and community radio stations, as well as harnessing the MomConnect and NurseConnect initiatives to improve awareness.[19,20]
7. The role of new technology and innovations such as the open data kit roll-out improved documentation of active-case search and surveillance supervision visits.[16]
8. Filling critical vacant positions (e.g. data manager and EPI specialist) at national level ensured close monitoring of the polio indicators and individualised support to address the gaps. In addition, ministerial communications on ensuring that targets for polio indicators were met spurred implementers to use data for planning and improved accountability.
Discussion
The high migration rates across SAs porous borders puts the country at risk of importing or exporting polioviruses.[21]
Therefore, it is critical that a good surveillance system and high immunisation coverage should be in place to detect and prevent. In December 2017, the ARCC rescinded the country's polio-free status owing to observed gaps in the national polio surveillance system.[14] Maintaining immunisation coverage and a sensitive surveillance system after being certified polio free is critical to retain the status.[5] This paper describes the SA experience of losing and regaining a polio-free status.
Firstly, the ARCC had two advocacy visits to the country and engaged with authoritative role players across all levels of implementation.[14] These advocacy visits were key in rekindling the national political commitment to prioritise and mobilise resources to strengthen polio surveillance structures. For example, ministerial communications demanding prioritisation of reaching the target indicators and allocating resources to fill important vacancies followed these advocacy visits.
Furthermore, identifying existing gaps and possible solutions during the quality improvement processes assistedin addressing the health systems gaps.[22] Strengthening health systems in provinces, districts and at a facility level helped to promote the use of data to identify and address gaps. Such support needs a continued, individualised approach, as seen in the performance of districts and provinces on key indicators. Therefore, continuous quality improvement would be key in sustaining the strengthened health systems gains.[23]
In addition, collaboration between partners and the uptake of innovative technology (e.g. the open data kit) have shown to be instrumental, as these measures improved the supervision rate for polio surveillance.[16] The roll-out and expansion of environmental surveillance were critical in complementing the existing AFP surveillance system.[18] In this case, both the use of the open data kit and implementing environmental surveillance were supported by the national WHO office.
Conclusion
This paper highlights that without effective leadership, commitment and monitoring, it is very easy for the long-term national poliovirus surveillance programme to break down, putting the African region at risk. Therefore, continued national support in maintaining and sustaining the national health programmes is critical to prevent the initiative from being neglected and risk the country losing its polio-free status.[14]
Declaration. None.
Acknowledgements. We acknowledge the collaborative efforts in supporting SA to address the gaps and regain its polio-free status, namely from the ARCC, Department of Health, WHO, UNICEF, National Institute for Communicable Diseases, the National Health Laboratory Service, the various polio committees and other partners.
Author contributions. All authors were involved in conceptualising and writing the paper and approved the final manuscript. JCYN is the guarantor of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Groce N, Banks LM, Stein M. Surviving polio in a post-polio world. Soc Sci Med 2014;107:171-178. https://doi.Org/10.1016/j.socscimed.2014.02.024 [ Links ]
2. Baicus A. History of polio vaccination. World J Virol 2012;1(4):108-114. https://doi.org/10.5501/wjv.vl.i4.108 [ Links ]
3. Cochi SL, Freeman A, Guirguis S, Jafari H, Aylward B. Global Polio Eradication Initiative: Lessons learned and legacy. J Infect Dis 2014;210(Suppl 1):S540-S546. https://doi.org/10.1093/infdis/jiu345 [ Links ]
4. Wold Health Organization. Global Polio Endgame Strategy 2019-2023: Eradication, intergration certification and containment. Geneva: WHO, 2019. [ Links ]
5. World Health Organization. Framework for certification of polio eradication in the African region. Dakar: WHO, 2018. [ Links ]
6. Okeibunor JC, Ota MC, Akanmori BD, et al. Polio eradication in the African Region on course despite public health emergencies. Vaccine 2017;35(9):1202-1206. https://doi.Org/10.1016/j.vaccine.2015.08.024 [ Links ]
7. World Health Organization. Global polio eradication initiative applauds WHO African region for wild polio-free certification, https://www.who.int/news-room/detail/25-08-2020-global-polio-eradication-initiative-applauds-who -african-region-for-wild-polio-free-certification. [ Links ]
8. Matjila MJ. Maintaining a polio-free status in South Africa - three national committees. KwaZulu-Natal Polio Symposium. Durban: Univeristy of KwaZulu-Natal, 11 March 2016. [ Links ]
9. World Health Organization. Polio-free status certification, https://www.afro.who.int/health-topics/polio/polio-certification (accessed 11 February 2021). [ Links ]
10. Department of Health. South Africa declared polio free, https://www.gov.za/health-sa-polio-free (accessed 2 February 2021). [ Links ]
11. Blecher M, Hussey G, Keen G, Eggers E, Girdler-Brown B. Eradication of poliomyelitis in South Africa. S Afr Med J 1994;84(10):664-668. [ Links ]
12. Dlamini N. Immunisation. District Health Barometer 2017;2017:137-154. [ Links ]
13. Hong H, Makhathini L, Mashele M, et al. Annual measles and rubella surveillance review, South Africa, 2017. Natl Inst Commun Dis Public Heal Surveill Bull 2017;16(2):64-77. [ Links ]
14. National Institute for Communicable Diseases. South Africa certified polio-free. http://www.nicd.ac.za/south-africa-certified-polio-free/. [ Links ]
15. Motsoaledi A (pers. comm, 2018). Polio eradication and need to improve acute flaccid paralysis (AFP) indicators namely: non AFP detection rate and stool adequacy [ Links ]
16. Maduka O, Akpan G, Maleghemi S. Using Android and Open Data Kit technology in data management for research in resource-limited settings in the Niger Delta region of Nigeria: Cross-sectional household survey. JMIR Mhealth Uhealth 2017;5(11):e171. https://doi.org/10.2196/mhealth.7827 [ Links ]
17. World Health Organization. Global Polio Eradication initiation: Polio Today, 2020. https://polioeradication.org/polio-today/preparing-for-a-polio-free-world/containment/ (accessed 11 February 2021). [ Links ]
18. Javed U. The Global Polio Eradication initiatives: From past to present. RADS J Biol Sci 2012. [ Links ]
19. National Department of Health. Together, we can ensure that South Africa youngest children receive the care they need to survive and thrive, https://sidebyside.co.za/ (accessed 20 March 2021). [ Links ]
20. Barron P, Peter J, LeFevre AE, et al. Mobile health messaging service and helpdesk for South African mothers (MomConnect): History, successes and challenges. BMJ Glob Health 2018;3(Suppl 2):e000559. https://doi.org/10.1136/bmjgh-2017-000559 [ Links ]
21. Segatti A, Landau L. Contemporary migration to South Africa: A regional development issue. Washington DC: World Bank, 2011. [ Links ]
22. Leatherman S, Ferris TG, Berwick D, Omaswa F, Crisp N. The role of quality improvement in strengthening health systems in developing countries. Int J Qual Health Care 2010;22(4):237-243. https://doi.org/10.1093/intqhc/mzq028 [ Links ]
23. Yapa HM, De Neve J-W, Chetty T, et al. The impact of continuous quality improvement on coverage of antenatal HIV care tests in rural South Africa; Results of a stepped-wedge cluster-randomised controlled implementation trial. PLoS Med2020;17(10):e1003150. https://doi.org/10.1371/journal.pmed.100315C [ Links ]
 Correspondence:
Correspondence:
J C YNyasulu
Julietnyasulu@gmail.com
Accepted 19 April 2021


{kind=link}