










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.16 n.1 Pretoria Apr. 2022
http://dx.doi.org/10.7196/sajch.2022.v16.i1.1835
RESEARCH
Outcomes of periviable neonates born and admitted to a resource-limited hospital, Cape Town, South Africa
N DormohamedI; L van WykII
IMMed (Paed) L Lloyd, Cert (Neonatology) (SA); Department Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IICert (Neonatology) (SA); Department Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND: Periviability, defined as a gestational age of 20 0/7 to 25 6/7 weeks, is considered the limit of foetal maturity where a reasonable chance of survival exists. The outcome of these neonates in sub-Saharan Africa is poorly described
OBJECTIVE: To describe the mortality and morbidities of periviable neonates admitted to a resource-limited public hospital in South Africa (SA
METHODS: This was a retrospective, descriptive study performed at Tygerberg Hospital, Cape Town, SA, between January 2017 and December 2018. Records of all periviable neonates (gestational age <27 weeks or birthweight <750 g) born at or admitted to Tygerberg Hospital within 24 hours of birth were included
RESULTS: The study population consisted of 186 periviable neonates, of whom 157 (84.4%) had a gestational age <27 weeks, 101 (54.3%) weighed <750 g and 72 (38.7%) were <27 weeks and weighed <750 g at birth. Severe intrauterine growth restriction was noted in 16% of cases. Neonatal mortality varied with gestational age. The overall survival rate was 51%, with survival increasing with increasing gestational age. Morbidities are described according to gestational age and birthweight, and also varied with gestational age. Most periviable neonates received comfort care or specific supportive care only, congruent with the provincial policy guidelines
CONCLUSION: This is the first study to describe survival and morbidities of neonates delivered at the periviable limit at Tygerberg Hospital, a resource-limited public hospital in SA. Despite restricted resources and limited care, ~50% of these periviable neonates survived
Periviability, also known as the limit of viability, is a stage of foetal maturity that is characterised by high rates of mortality and severe morbidities among survivors.[1] The American College of Obstetricians and Gynaecologists defines it as delivery occurring between 20 0/7 and 25 6/7 weeks of gestation.[1] However, the definition of periviability varies between countries and facilities.[2,3] In the South African (SA) legislature, viability is not clearly defined, but in the case of the State vs. Molefe, the court ruled that foetal viability occurred at 28 weeks' gestation.[4]
The overall sub-Saharan neonatal mortality rate is 28 per 1 000 live births, which is much higher than the global rate of 19 deaths per 1 000 live births. In 2015, SA had a neonatal mortality rate of 15 per1 000 live births.[5]
Birthweight is often used as a proxy for gestational age in SA as many mothers do not attend antenatal clinics for early antenatal ultrasound dating.[6] Varying survival rates for neonates of extremely low birthweight have been reported in SA, ranging from 26% for neonates with a birthweight of less than 900 g to 56% for neonates with a birthweight <750 g and 79% for neonates with a birthweight of 750 - 1 250 g.[7,8]
Neonates delivered during the periviable period are at risk of significant morbidities, including respiratory distress syndrome, necrotising enterocolitis, intraventricular haemorrhage (IVH), periventricular leukomalacia, sepsis, retinopathy of prematurity (ROP) and chronic lung disease, with incidences linked to gestational age at birth.[9]
With just under 100 000 deliveries per annum, and a low-birthweight rate of 14% (2014 - 2016),[10] the Western Cape public health sectors resources are strained. In 2014, Tygerberg and Groote Schuur hospitals, the provincial academic hospitals, developed a protocol to standardise the postnatal interventions for periviable preterm infants.[11] According to this protocol, periviability is defined as neonates delivered at a gestational age of <27 weeks or a birthweight of <750 g to allow for optimal care being available to the most viable babies.
This study aimed to describe the survival rate and common neonatal morbidities in neonates delivered at the limit of periviability, as defined by the Western Cape periviability guidelines (i.e. <27 weeks gestational age or a birthweight of <750 g).
Methods
This was a retrospective, descriptive study performed at Tygerberg Hospital, a resource-constrained, public hospital in Cape Town, SA, from January 2017 to December 2018.
Records of all neonates born at Tygerberg Hospital, or transferred to the facility within 24 hours of birth, at a gestational age < 27 weeks or a birthweight <750 g were included in the analysis. Neonates with lethal congenital anomalies or for whom records were missing wereexcluded. Data were extracted from an existing neonatal database.
The following definitions were used for neonatal morbidities:
• neonatal respiratory distress syndrome - respiratory distress symptoms and signs and X-ray findings in keeping with surfactant deficiency[12]
• patent ductus arteriosus (PDA) - diagnosed by echocardiography or clinical symptoms[13]
• early-onset sepsis - a positive blood culture or C-reactive protein level >10 mmol/L within the first 72 hours of life[14]
• nosocomial sepsis - a positive blood culture or C-reactive protein level >10 mmol/L after 72 hours of life[15]
• necrotising enterocolitis - as per the Bell's criteria[16]
• chronic lung disease - respiratory support at 36 weeks' corrected gestational age[17]
• ROP - graded according to the International Committee for the Classification of Retinopathy of Prematurity[18]
• IVH - graded according to Papile's classification.[19]
Levels of supportive care were referenced from the Western Cape periviability protocol and were defined as follows:[11]
• comfort care - every effort would be made to increase the neonate's comfort, decrease pain and distress, and maintain dignity and humanity while avoiding all painful and uncomfortable procedures; includes the provision of oxygen via nasal prongs, intravenous fluids and antibiotics
• specific life-supportive care - attention to comfort, pain, dignity and humanity while providing specific support measures, including provision of oxygen via nasal prongs, caffeine and one dose of surfactant but excluding mechanical ventilation and life-prolonging care
• life-prolonging care - offered to neonates with a gestational age >27 weeks and a birthweight >800 g and includes specific life-supportive measures and mechanical ventilation.
Statistical analysis
Descriptive data are presented as means and associated standard deviations (SDs) and numbers and frequencies. Student's t-test and chi-squared (x2) tests were used to compare variables related to maternal and neonatal demographics (administration of antenatal steroids; mode of delivery; birthweight; resuscitation at delivery; and admission temperature) and neonatal clinical variables (gestational age; administration of surfactant; nosocomial sepsis; ROP; IVH) between survivors and non-survivors. The software package STATA (Stata Corp. 2015, College Station, TX: Stata Corp LL) was used for statistical analysis. A p-value <0.05 was considered statistically significant.
Ethical considerations
The study was approved by the Stellenbosch University Health Research and Ethics Committee (ref. no. S19/10/238). As this study was retrospective, a waiver of consent was granted. The research was conducted in accordance with Declaration of Helsinki (World Medical Association).
Results
Demographics of study population
Between January 2017 and December 2018, 1 556 neonates of very low birthweight were admitted to the neonatal service at Tygerberg Hospital. Of these patients, 186 (12%) were at the limits of viability (Table 1), with 157 neonates (84.4%) at <27 weeks' gestational age, 101 (54.3%) weighing <750 g and 72 (38.7%) being both <27 weeks and weighing <750 g at birth. Of the total study population, eight neonates (4.3%) were delivered at peripheral hospitals and admitted to Tygerberg within 24 hours.

Most pregnancies were dated by early ultrasound, with only one-fifth requiring dating by postnatal foot length measurements (Table 1). As shown in Table 1, almost all of the HIV-positive mothers were on antiretroviral treatment. Very few mothers who tested positive for syphilis had been adequately treated prior to delivery. Although most mothers (72%) had received antenatal steroids, 23% had received only one dose.
Approximately one-third of neonates were hypothermic at admission (12% with a body temperature <36°C; 23% with a body temperature of 36.0 - 36.5°C). Resuscitation at delivery was required by most neonates (Table 1) and included intermittent positive pressure ventilation (8%), continuous positive air pressure ventilation (43%) and cardiopulmonary resuscitation (8%). All but two patients required respiratory support upon admission in the form of oxygen via nasal prongs, humidified high-flow or continuous positive air pressure for a duration of 40.4 (27.4) days. Sixteen patients (9%) required admission to the neonatal intensive care unit owing to nosocomial sepsis (40%) and respiratory distress syndrome (34%).
Morbidities
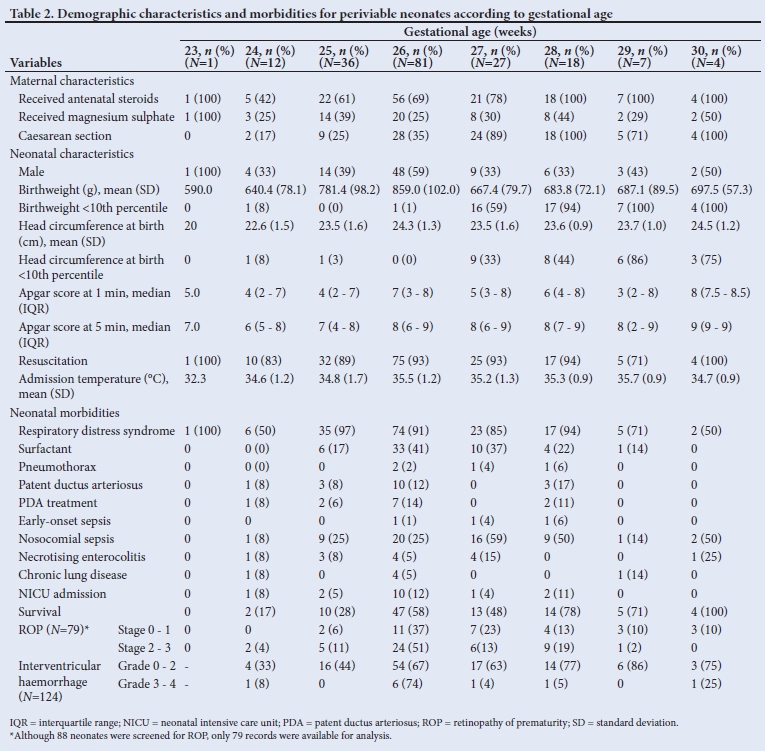
Maternal and neonatal characteristics, together with neonatal morbidities, are shown according to gestational age at birth in Table 2. Respiratory distress syndrome was the most common cause of morbidity, decreasing as gestational age increased.
Surfactant was administered more often to older neonates, but with decreasing need after 28 weeks' gestational age. ROP screening was performed in 93% of survivors(n/N=88/91): 30 (32%) had ROP stage 0 - 1 and 49 (62%) had stage 2 - 3; no records were available for nine of the neonates, despite having been screened. Cranial ultrasound screens were performed in 124 (69%) of the neonates, with 114 (92%) found to have grade 0 - 2 IVH and 10 (8%) with grade 3 - 4 IVH.
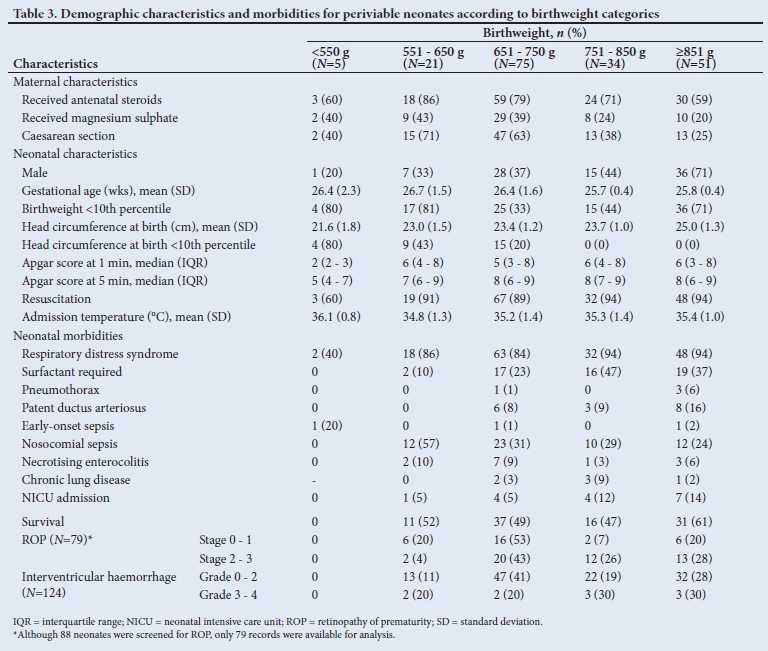
Maternal and neonatal demographics, together with neonatal morbidities, are shown according to birthweight in Table 3.
Survival and mortality
The overall survival rate was 51% (n=95), of whom 39 (41%) were discharged home and the rest transferred to other medical facilities for continued care. The mean (SD) length of hospitalisation for neonates who were discharged home was 91.2 (63.7) days, whereas neonates who were transferred elsewhere were hospitalised at Tygerberg Hospital for 55.7 (16.7) days. Death occurred at a mean (SD) age of 12.1 (38.7) days.
Mortality rate decreased, as expected, with increasing gestational age, despite a birth weight <750 g (i.e. severe intrauterine growth restriction (IUGR) as categorised by the Intergrowth-21st Consortium's reference standards).[20]
Significant differences (p<0.05) were found between survivors' and non-survivors' maternal and neonatal demographic characteristics with regard to antenatal steroid administration, mode of delivery, birthweight, resuscitation at delivery and admission temperature (Table 4). Significant differences (p<0.05) were found for survivors' and non-survivors' neonatal clinical variables with regard to gestational age, birthweight <10th centile for gestational age, head circumference <10th centile for gestational age, surfactant administration, nosocomial sepsis, all grades of ROP and IVH grade 0 - 2 (Table 4). A larger number of non-survivors (n=34; 69%) than survivors (n=20; 21%) received surfactant, suggesting that non-survivors may be sicker and more unstable neonates. All neonates who developed pneumothorax were on humidified high-flow oxygen and continuous positive air pressure ventilation.
Allocation of care
Supportive care was allocated according to the guidelines of the Western Cape periviability protocol. Most neonates (77%) were allocated supportive care within the first 2 days of life. Of the neonates <27 weeks, 56% and 25% received comfort and specific supportive care, respectively. Ofthe infants with birthweights <750 g, 60% and 17% received comfort and specific supportive care, respectively, with 1% receiving life-prolonging care (Table 5).
As per institutional protocol, the level of care should be reviewed every two weeks and be adjusted according to current weight, corrected gestational age and expected prognosis of the patient. Fifty neonates' supportive care plans were reassessed after approximately 3 weeks: 80% were escalated to life-prolonging care while 16% were downgraded to comfort care only. Four neonates' care plans were reviewed after approximately 6 weeks, with three of the plans changed to comfort care only (Fig. 1).

Of the 94 patients who were allocated to receive comfort care only, 84 (89%) received intermittent positive pressure ventilation at resuscitation before being placed on respiratory support in the neonatal ward. Thirty-nine neonates (21%) received surfactant while allocated to comfort care only, despite not qualifying for surfactant administration as per the Western Cape periviability guidelines.
Discussion
This is the first study to describe the short-term morbidities and survival of periviable neonates (defined as a gestational age of <27 weeks or birthweight <750 g) admitted to a resource-limited public hospital in Cape Town, SA. Neonatal mortality varied with gestational age, as expected. Birthweight-related survival seemed to be dependent on weight appropriateness rather than absolute weight.
In this study, the survival rate, according to gestational age, was lower than that found in studies from Thailand and Turkey.[21,22] In the current study, the use of antenatal steroids, caesarean section, birthweight, resuscitation and temperature at admission were associated with survival, similar to the findings of another study.[23] Sex was not found to influence survival, in contrast to findings from a Californian study which found that female neonates had better outcomes.[23]
In the current study, respiratory distress syndrome was common, similar to what was found in Turkish and Chinese studies.[22,24] Chronic lung disease was uncommon in this study, in contrast to many international studies, one of which found that the incidence may be as high as 44.2% in periviable neonates.[17] This may be due to the use of less invasive strategies for ventilation and surfactant administration in the current study population, as well as the higher mortality rate seen, owing to the application of the Western Cape Department of Health protocol for periviable preterm neonatal care.
Very few neonates were treated for PDA in the current study. Neonates at Tygerberg are not routinely screened for PDA, in contrast to many international institutions,[13] owing to a lack of resources and the large number of low-birthweight neonates being admitted. The liberal use of antenatal steroids and administration of surfactant may also have contributed to the low incidence of symptomatic PDA.
Necrotising enterocolitis was common in our study. This is similar to findings from studies from other resource-restricted settings,[25] but contrary to those from developed countries.[16] This may be explained by the use of breastmilk only in this population group (the practice at Tygerberg Hospital is to feed only mother's milk or donor-expressed breastmilk to neonates with a gestational age of <32 weeks and a birthweight of <1 200 g) and also the high mortality in the cohort.
The prevalence of ROP was low in this study, despite a relatively high screening rate. This is similar to findings from a Turkish study, which showed a prevalence of 24.4% for stage 2 ROP in periviable neonates.[22] However, the prevalence reported in the current study is much lower than that of an earlier SA and Kenyan study (30.3% and 41.7%, respectively).[18,26]
Cranial ultrasound screening was performed in many neonates in the study and IVH was often detected, albeit of a low grade. A study from Nigeria showed a lower prevalence of IVH in neonates of very low birthweight.[19] This could be due to the higher survival rate of neonates in SA compared with the rest of sub-Saharan Africa.
The decision whether to treat or not to treat neonates delivered at the limit of periviability in developing (resource-constrained) countries is difficult. Generally accepted prognostic factors, such as birthweight, sex, plurality of birth and exposure to antenatal corticosteroids, are often superseded by challenges of limited resources, lack of neonatal training, cost of care and different ethical or cultural considerations. In addition, most doctors in less-developed countries rank quality of life and suffering as more important than economic burden and legal considerations.[27] Providing care to infants like these leads to the increased use of already-constrained human and institutional resources at a high financial cost, with possible poor neurodevelopmental outcomes, poor long-term quality of life for survivors and additional burden to the family and healthcare facilities. Ongoing ethical concerns are the dilemmas of distributive justice versus beneficence and non-maleficence in the face of resource constraints in these countries.
Being from an upper middle-income country with limited resources, the public health sector in SA must ration health resources when treating infants born at a periviable gestational age. A balance must be achieved between improving outcomes with improved neonatal care for periviable neonates, using restricted resources judiciously and the unknown neurodevelopmental outcome of these patients.
Study limitations
The limitations of the study are related to its retrospective nature, which limited the accuracy of some of the neonatal outcome data. With the small size of the study population, absolute numbers in the respective categories of gestational age and birthweight were also small, compromising the generalisability of the findings. No long-term neurodevelopment follow-up was performed for these neonates.
Conclusion
This is the first study to investigate the survival and morbidities of neonates delivered at the limits of periviability at Tygerberg Hospital, a resource-constrained public hospital in Cape Town, SA. Despite limited resources and care, nearly 50% of the neonates born at <27 weeks or at a birthweight of <750 g survived. Higher survival was observed among neonates who were growth appropriate for gestational age. Further research is required on the outcome of periviable infants, especially with regard to neurocognitive development.
Declaration. This research was in part fulfillment of the MPhil in Neonatology.
Acknowledgements. The authors acknowledge Dr Sandi Holgate and other neonatal doctors for the management of the neonatal registry.
Author contributions. As primary investigator, ND conceptualised the study, collected the data and prepared the manuscript. LvW was the study supervisor and contributed to data analysis and manuscript preparation prior to submission. As co-supervisor, LL contributed to manuscript preparation prior to submission.
Funding. None.
Conflicts of interest. None.
References
1. Raju TNK, Mercer BM, Burchfield DJ, Joseph GF. Periviable birth: Executive summary of a Joint Workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. J Perinatol 2014;34:333-342. https://doi.org/10.1038/jp.2014.70 [ Links ]
2. Nishida H, Sakuma I. Limit of viability in Japan: Ethical consideration. J Perinat Med 2009;37:457-460. https://doi.org/10.1515/JPM.2009.112 [ Links ]
3. Costeloe KL, Hennessy EM. Short term outcomes after extreme preterm birth in England: Comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ 2012;345:e7976. https://doi.org/10.1136/bmj.e7976 [ Links ]
4. Du Toit-Prinsloo L, Pickles C, Saayman G. Managing the remains of fetuses and abandoned infants: A call to urgently review South African law and medicolegal practice. S Afr Med J 2016;106:578-581. https://doi.org/10.7196/SAMJ.2016.v106i6.10598 [ Links ]
5. Naidoo H, De Witt TW, Coetzee M. Improving survival of preterm babies in low- to middle-income countries - What can we do? S Afr J Child Health 2018;12(3):117-120 https://doi.org/10.7196/SAJCH.2018.v12i3.1503 [ Links ]
6. Poggenpoel EJ, Geerts LTGM, Theron GB. The value of adding a universal booking scan to an existing protocol of routine mid-gestation ultrasound scan. Int J Gynecol Obstet 2012;116:201-205. https://doi.org/10.1016/j.ijgo.2011.10.027 [ Links ]
7. Kalimba EM, Ballot DE. Survival of extremely low-birth-weight infants. S Afr J Child Health 2013;7:13-16. https://doi.org/10.7196/SAJCH.488 [ Links ]
8. Kirsten GF, Kirsten CL, Henning PA, et al. The outcome of ELBW infants treated with NCPAP and InSurE in a resource-limited institution. Pediatrics 2012;129(4):e952-e959. https://doi.org/10.1542/peds.2011-1365 [ Links ]
9. Morgillo D, Morgillo-Mitchell J, Fontanta M, et al. Outcome of extremely low gestational age newborns (ELGANs ) following a pro-active treatment approach. Swiss Med Wkly 2014;144:w14014. https://doi.org/10.4414/smw.2014.14014 [ Links ]
10. National Perinatal Mortality and Morbidity Committe. Saving babies 20142016: Triennial report on perinatal mortality in South Africa. Pretoria: National Department of Health, 2018. [ Links ]
11. Standard post-natal interventions for peri-viable preterm birth in extremely low birth weight infants in the Western Cape Province Department of Health - Decision Support Framework. http://www.obstyger.co.za/Downloads/Periviable_province.pdf (accessed 1 March 2021). [ Links ]
12. Kamath BD, MacGuire ER, McClure EM, Goldenberg RL, Jobe AH. Neonatal mortality from respiratory distress syndrome: Lessons for low-resource countries. Pediatrics 2020;127(6):1139-1146. https://doi.org/10.1542/peds.2010-3212 [ Links ]
13. Benitz WE. Treatment of persistent patent ductus arteriosus in preterm infants: Time to accept the null hypothesis? J Perinatol 2010;30:241-252. https://doi.org/10.1038/jp.2010.3 [ Links ]
14. Braye K, Foureur M, De Waal K, Jones M, Putt E, Ferguson J. Epidemiology of neonatal early-onset sepsis in a geographically diverse Australian health district 2006-2016. PLoS One 2019;14(4):e0214298. https://doi.org/https://doi.org/10.1371/journal.pone.0214298 [ Links ]
15. Mahieu LM, De Muynck AO, De Dooy JJ, Laroche SM, Van Acker KJ. Prediction of nosocomial sepsis in neonates by means of a computer-weighted bedside scoring system (NOSEP score). Crit Care Med 2000;28(6):2026-2033. [ Links ]
16. Lee JS, Polin RA. Treatment and prevention of necrotizing enterocolitis. Semin Neonatol 2003;8(6):449-459. https://doi.org/10.1016/S1084-2756(03)00123-4 [ Links ]
17. Davidson LM, Berkelhamer SK. Bronchopulmonary dysplasia: Chronic lung disease of infancy and long-term pulmonary outcomes. J Clin Med 2017;6(1):4. https://doi.org/10.3390/jcm6010004 [ Links ]
18. Jacoby MR, Du Toit L. Screening for retinopathy of prematurity in a provincial hospital in Port Elizabeth, South Africa. S Afr Med J 2016;106(6):598-601. https://doi.org/10.7196/SAMJ.2016.v106i6.10663 [ Links ]
19. Adegoke S, Ayoola O, Bankole KP, Ogunlesi TA. Intraventricular hemorrhage in newborns weighing <1500 g: Epidemiology and short-term clinical outcome in a resource-poor setting. Ann Trop Med Public Health 2014;7(1):48-54. https://doi.org/10.4103/1755-6783.14501320. [ Links ]
20. Villar JG, Fenton TR, Ohuma EO, Ismail LC, Kennedy SH. INTERGROWTH-21st very preterm size at birth reference charts Lancet 2016;387(10021):844-845. https://doi.org/10.1016/S0140-6736(16)00384-6 [ Links ]
21. Piriyapokin N, Chuthapisith J, Emrat K, Nuntnarumit P. Outcomes of preterm infants born with marginal viability in a university hospital in Thailand J Paediatr Child Health 2020:56(6):943-949. https://doi.org/10.1111/jpc.14782 [ Links ]
22. Kulali F, Bas AY, Erol S, et al. Survival of periviable infants : 5-year experience at a single center. J Matern Fetal Neonatal Med 2019;33(22):3725-3731. https://doi.org/10.1080/14767058.2019.1583734 [ Links ]
23. Anderson JG, Baer RJ, Partridge JC, et al. Survival and major morbidity of extremely preterm infants: A population-based study. Pediatrics 2016;138(1):e20154434. https://doi.org/10.1542/peds.2015-4434 [ Links ]
24. Xu F, Kong X, Duan S, et al. Care practices, morbidity and mortality of preterm neonates in China, 2013-2014: A retrospective study. Sci Rep 2019;9:19863. https://doi.org/10.1038/s41598-019-56101-x [ Links ]
25. Banieghbal B, Schoeman L, Kalk F, Da Fonseca JM, Davies MRQ. Surgical indications and strategies for necrotizing enterocolitis in low income countries. World J Surg 2002:26(4):444-447. https://doi.org/10.1007/s00268-001-0246-6 [ Links ]
26. Onyango O, Sitati S, Amolo L, et al. Retinopathy of prematurity in Kenya: Prevalence and risk factors in a hospital with advanced neonatal care. Pan Afr Med J 2018;29:152. https://doi.org/10.11604/pamj.2018.29.152.14046 [ Links ]
27. Patel RM, Rysavy MA, Bell EF, Tyson JE. Survival of infants born at periviable gestational ages. Clin Perinatol 2017;44(2):287-303. https://doi.org/10.1016/j.clp.2017.01.009 [ Links ]
28. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014;14:135. https://doi.org/10.1186/1471-2288-14-135. [ Links ]
 Correspondence:
Correspondence:
L van Wyk
lizelle@sun.ac.za
Accepted 15 March 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}