










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Child Health
versión On-line ISSN 1999-7671
versión impresa ISSN 1994-3032
S. Afr. j. child health vol.16 no.1 Pretoria abr. 2022
http://dx.doi.org/sajch.2021.v16.i1.1829
RESEARCH
The profile of ancillary laboratory tests in neonates with positive blood and/or cerebrospinal fluid cultures
L SonoI; S VelaphiII
IMB ChB, FCPaeds; Department of Paediatrics, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand and Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
IIMB ChB, PhD; Department of Paediatrics, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand and Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Blood and cerebrospinal fluid (CSF) cultures are used as a gold standard to diagnose neonatal sepsis/meningitis. A challenge in their use is low yield, and limited availability, especially in low-resource settings
OBJECTIVE: To evaluate profiles of full blood count (FBC), C-reactive protein (CRP), and CSF cell count and protein in neonates with culture-proven sepsis/meningitis
METHODS: Neonates with positive blood and/or CSF cultures who had results for FBC, CRP, CSF cell count and protein performed within 24 - 48 hours of culture were enrolled. The proportion of neonates with abnormalities in these tests was calculated and comparisons among different types of pathogens was performed
RESULTS: A total of 942 isolates were cultured in blood and/or CSF. Organisms isolated were Gram-negative (GN) bacteria (62.0%), Gram-positive (GP) bacteria (23.4%) and Candida species (14.6%). Common abnormality in FBC was thrombocytopenia, which was observed in 30% of neonates with culture-proven sepsis. There was a higher proportion of neonates with thrombocytopenia among those infected with GN bacteria (39.9%) and Candida species (44.6%) compared with those infected with GP bacteria (15.1%; p<0.001). Leukopenia was relatively more common among neonates infected with GN bacteria than those infected with GP bacteria (20.8% v. 8.4%; p<0.001). More than two-thirds (70%) of neonates had high CRP (>10 mg/L). Finally, less than a third of neonates (26.7%) with positive CSF cultures had abnormal CSF cell count (>20 cells/mm3) and 61.6% had high protein (>150 mg/dL
CONCLUSION: Majority of neonates with positive blood or CSF cultures have normal FBC or CSF cell count; therefore, the absence of abnormalities in these parameters cannot be used solely to exclude sepsis. CRP appears to be the most useful test for diagnosing sepsis, as it is raised in 70% of patients with culture-proven sepsis
Sepsis has been described as a systemic inflammatory response to pathogens such as bacteria, viruses, or fungi that is associated with haemodynamic changes and other clinical manifestations.[1,2] The definition of sepsis also includes isolation of pathogens from normally sterile body fluids such as blood and cerebrospinal fluid (CSF). Blood and/or CSF culture is the gold standard in the diagnosis of sepsis. In resource-limited settings, healthcare facilities might not have access to blood culture results for days after working up a patient with a possible serious bacterial infection (pSBI). Waiting for culture results will therefore result in delays in initiating antibiotics in neonates with pSBI. This often results in patients being treated based on clinical signs suggestive of sepsis and available laboratory ancillary tests, namely full blood count (FBC) and/or C-reactive protein (CRP), which are more easily accessible than blood cultures. Even when blood cultures are accessible, they are only available after 24 hours and the yield is low despite a patient having clinical signs suggestive of sepsis.
Delayed initiation of appropriate treatment for sepsis is associated with increased morbidity and mortality;[3,4] thus, antibiotics are started or continued based on abnormalities in FBC, white blood cell differential count (WBC-Diff) and CRP. The proportion of patients with bacterial or fungal culture-proven sepsis who have abnormal ancillary laboratory tests is not well known, especially in settings where there is a high incidence of sepsis. Knowing these proportions will assist attending physicians in estimating the likelihood of patients having sepsis due to bacterial or fungal infections in settings where culture is negative or not available. In this study we sought to determine abnormalities in FBC, WBC-Diff, and CRP in neonates with bacterial or fungal organisms considered pathogens isolated from blood, and to determine CSF cell count and protein levels in neonates with organisms isolated in CSF.
Methods
This is a retrospective study conducted at Chris Hani Baragwanath Academic Hospital (CHBAH), a public tertiary hospital in Soweto, South Africa (SA). The study population were neonates with pSBI admitted to the neonatal unit at CHBAH and identified to have a positive blood and/or CSF culture from January to December 2017. The inclusion criteria consisted of all neonates who had positive blood and/or CSF culture due to organisms considered a possible pathogen and at least one of the laboratory ancillary test results being available from the National Health Laboratory Services (NHLS) database. Corynebacterium, Bacillus, and coagulase-negative Staphylococcus were considered as contaminants and thus were excluded from the analysis. Ancillary laboratory tests assessed were total white blood cell count (WBC), platelet count, WBC-Diff, CRP levels, CSF cell count, and protein levels. For multiple organisms cultured, each organism was considered as a separate episode of bloodstream infection, thus laboratory ancillary tests were captured for each separate organism. The FBCs that were assessed were only those that were done within 24 hours of culture, and for CRPs it was only those that were done within 48 hours of culture.
Definitions of abnormalities for different parameters on laboratory ancillary tests were as follows: leukocytosis - white blood cell count >25 x 109/L;[5] leukopenia - white blood cell count <5 x 109/L; thrombocytopenia - platelet count <100 x 109/L;[6] neutrophilia - neutrophil count >7 x 109/L;[5,7] neutropenia - neutrophil count <1.75 x 109/L;[5] increased immature to total neutrophil ratio -ratio >0.2;[5,8] high CRP - CRP >10 mg/L[9] abnormal CSF white cell count - cell count >20 cells/mm3;[10] and high CSF protein - protein >150 mg/dL.[11]
The data were captured into a Microsoft Excel spreadsheet and analysed using Statistica (TIBCO Software Inc., USA). Comparisons in the proportion of patients with abnormalities in blood or CSF parameters among the different organisms were made using the Chi-squared test. The difference with a p<0.05 was considered statistically significant. The study was approved by the Human Research Ethics Committee (HREC) of the University of the Witwatersrand (ref. no. M180289).
Results
Organisms isolated from sterile sites
There were 942 neonates with pSBI who had positive cultures due to organisms considered to be pathogens over a 12-month period. A total of 886 and 106 pathogens were isolated in blood and CSF, respectively, and 50 of these were isolated from both blood and CSF (Table 1). Gram-negatives were the most common type of organisms found in both blood and CSF (62.0%; n=584). The most common bacteria isolated among the Gram-negatives were Acinetobacter baumannii (46.4%; n=271) and Klebsiella pneumoniae (33.9%; n=198). Among the Gram-positives, the common bacteria were Enterococcus species (33.6%; n=74), Staphylococcus aureus (21.4%; n=47) and Streptococcus viridans (20.9%; n=46). The most common fungi were Candida parapsilosis (62.3%; n=86) and Candida albicans (27.5%; n=38).

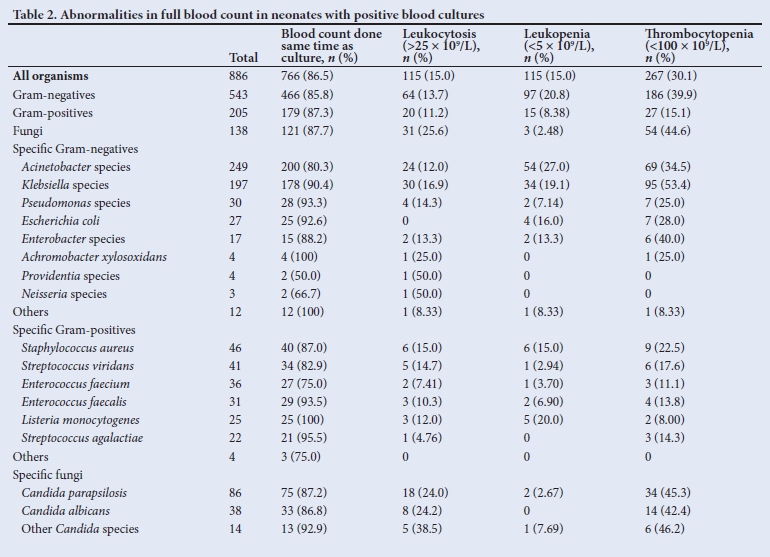
Abnormalities in full blood count
Abnormalities in FBC in neonates with culture-proven sepsis overall and for different types of organisms are presented in Table 2. More than three-quarters (85%) of neonates with positive blood cultures had results of FBC available and with blood for FBC having been taken at the same time or within 24 hours as the culture. Other FBCs had clotted and were repeated at more than 24 hours after the blood culture and thus were excluded from the analysis. The common abnormality in FBC was thrombocytopenia for all pathogens, occurring in 30% of neonates with positive cultures. Thrombocytopenia was observed in a low proportion of neonates infected with GP bacteria compared with those with GN (15.1% v. 39.9%, p<0.001) and fungal (15.1% v. 44.6%; p<0.001) infections. There were no significant differences in the proportion of neonates with thrombocytopenia infected with GN bacteria and fungi (39.9% v. 44.6%; p=0.366). Klebsiella species (53.4%) were the most common GN bacteria cultured in neonates with thrombocytopenia, followed by Pseudomonas species (25.0%). There were no significant differences in proportions of neonates with thrombocytopenia with specific organisms that were GP or fungi. Leukocytosis and leukopenia occurred at equal rates (15%) among neonates with positive cultures. Leukopenia was observed in relatively higher proportion in neonates infected with GN bacteria than those with GP (20.8% v. 8.4%; p<0.001) or fungal infections (20.8% v. 2.5%; p<0.001); while leukocytosis was more common in neonates with fungal infections than those with GN infection (25.6% v. 13.7%; p=0.002).
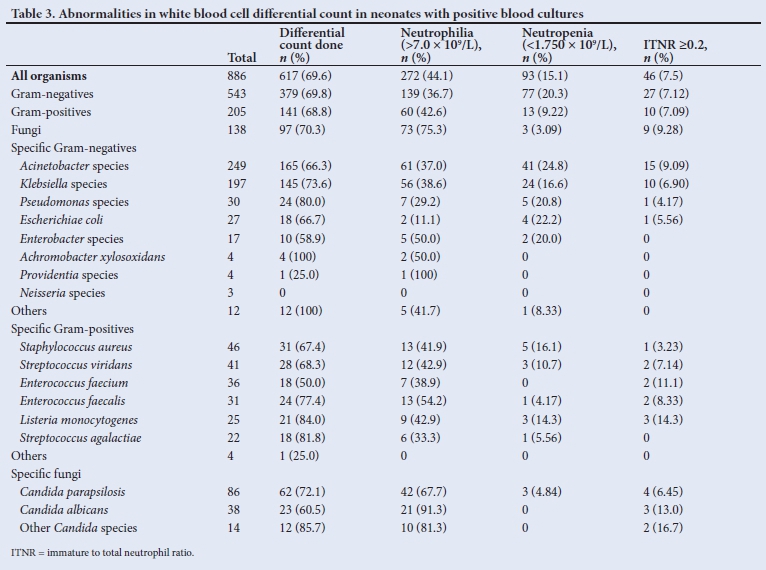
Abnormalities in white blood cells differential counts
The common abnormality in the WBC-Diff was neutrophilia for all types of organisms, but it was seen in higher proportions in those with fungal infection compared with those with GN (75.3% v. 36.7%; p<0.001) and GP bacterial infections (75.3% v. 42.6%; p<0.001) (Table 3). Neutropenia was more common in neonates with GN than GP (20.3% v. 9.2%; p=0.003) or fungal (20.3% v 3.1%; p<0.001) infections. Overall, less than a tenth of neonates with culture-proven sepsis had abnormal immature to total neutrophil ratio (ITNR). The proportions of the above abnormalities for individual organisms were similar for most organisms within each group of organisms.
CRP levels in neonates with positive blood cultures
CRP was done within 48 hours of blood culture and the results were available for 80% of neonates who had positive cultures (Table 4). It was abnormal in 53.9%, 73.5% and 82.7% of neonates with positive cultures for GP, GN, and Candida species, respectively. More than two-thirds of neonates had abnormal CRP (>40 mg/L). Less than three-quarters (70%) of neonates with GN infections had abnormal CRP except for Pseudomonas, where only 21.7% of cases had abnormal CRP. Among those with GP bacterial infections, a higher proportion of neonates with Streptococcus agalactiae (58.8%) and Listeria monocytogenes (86.7%) had high CRP. More than three-quarters (80%) of neonates with fungal culture sepsis had abnormal CRP.

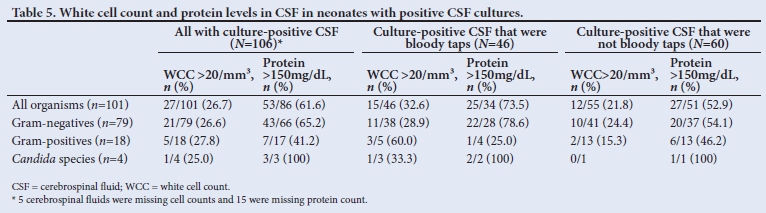
Abnormalities in CSF cells counts and protein levels among those with positive CSF cultures
The total number of pathogens isolated from the CSF was 106 (Table 5). Cell counts were missing in 4.7% (n=5/106) of patients and protein levels were missing in 18.9% (n=20/106) of patients. More than a third (45.5%; n=46) of CSF cultures were considered to be a bloody tap (defined as red blood cell count >500 x 109/L).[12] Jus over a quarter of neonates (26.7%) had high CSF WCC defined as count >20 cells/mm3, while under two-thirds (61.6%) of neonates had protein levels >150 mg/dL. The proportion of neonates with high CSF WCC was similar for the different types of organisms, while those with GN- (65.2%) and Candida species-positive (100%) cultures had high protein levels than those with GP cultures (41.2%; p<0.001). There was a higher proportion of neonates who had bloody tap CSF with a high WCC (32.6% v. 21.8%, p=0.01) and higher protein (73.5% v. 52.9%, p<0.001) than those without a bloody tap.
Discussion
In this study, we found that all neonates who had cultures done had FBCs done as part of a workup for sepsis, though only 86% of FBC were available for analysis. The main reason for unavailability was that the FBC done at the time of culture had clotted. The use of CRP and WBC-Diff was relatively lower than that of FBC, at 80% and 70%, respectively. In an analysis of FBCs, the common abnormality in neonates with positive cultures was thrombocytopenia, occurring in about 30% of cases and was observed at relatively higher frequencies in neonates with positive cultures for GN and fungal isolates. The proportion of neonates with thrombocytopenia was similar between those infected with GN bacteria and Candida species. Abnormalities in total WBC occurred in only 15% of cases, with leukocytosis being more common in those with fungal sepsis and leukopenia being common in those with GN cultures. Among those with WBC-Diff available, the common abnormality was neutrophilia followed by neutropenia, with neutrophilia being observed more commonly in those with fungal isolates and neutropenia being more common in those with GN isolates. Abnormalities in ITNR were observed in only less than 10% of cases. Overall, the ancillary test that was abnormal in most cases with positive cultures was CRP, as it was observed to be abnormal (>10 mg/L) in over 70% of neonates. High CSF protein was observed in a much higher proportion than high CSF cell count, occurring in about two-thirds, compared with high CSF cell count that was observed in only a quarter of neonates with positive CSF cultures.
Few studies have looked at the relationship between the presence of thrombocytopenia and positive culture results. One study that used a platelet cut-off of 100 x 109/L to define thrombocytopenia, reported a much higher prevalence of thrombocytopenia of 67% among those with culture-proven sepsis, compared with our findings where the prevalence was only 30%.[13] A prospective study of 230 positive blood cultures done in India[13] between the years 2000 and 2005 found that the proportion of patients with fungal, GN, and GP organisms who had thrombocytopenia was 50.0%, 45%, and 19.6%, respectively. Another cohort study of very-low-birthweight neonates with 154 positive blood cultures reported that neonates with GN and fungal isolates were more likely to have low platelet counts than those with GP cultures.[14] A multivariate analysis reported that GN sepsis as opposed to GP sepsis was independently associated with thrombocytopenia in neonatal sepsis. [6] There are suggestions that the endotoxin produced by GN organisms causes platelet destruction; thus, the high prevalence of sepsis in GN-infected patients. Thrombocytopenia could also indicate the severity of illness caused by GN organisms, or be due to disseminated intravascular coagulation.[15-17] Based on our findings in this study, the absence of thrombocytopenia cannot be used to exclude sepsis, as only about a third of neonates with culture-proven sepsis have thrombocytopenia and its presence cannot be used to differentiate between patients infected with fungi and those with bacteria, as it occurs at similar rates in those infected with GN and those with fungal culture-confirmed sepsis.
In this study, leukocytosis and leukopenia were found to be occurring at a similar rate (15%), with leukocytosis observed to occur commonly among the fungal infected cases while leukopenia was observed more commonly in neonates with GN cultures. A study that used a definition of leukocytosis (WBC >25 000) similar to ours, reported that 50% of positive blood culture cases had leukocytosis,[18] much higher than that observed in this study. Neutropenia has previously been reported to occur in 8.6% of infants with culture-proven sepsis, much lower than 15% reported in this study, but reported a higher prevalence of 26.6% among neonates with GN sepsis.[19,20] A study from Pakistan[18] reported that the immature to total neutrophil ratio (ITNR) had a sensitivity of 76.5%, much higher than the 7.5% observed in this study. In a retrospective review of 49 positive cultures in neonates, the ITNR was significantly higher among neonates with GN cultures,[20] which is different from our findings, where the rates of ITNR >0.2 occurred at similar frequencies among the different types of organisms. A study conducted in Japan[21] reported similar findings to this study, where the ITNR was similar among neonates with GP and GN bacterial growth in blood cultures.
High CRP was the most common abnormality in neonates, with positives cultures for all types of organisms. It appears that CRP is a relatively more reliable test in establishing the diagnosis of sepsis in neonates.[22] In a cross-sectional validation study of CRP done in Pakistan[18] in 2012 consisting of 147 neonates with 104 having positive blood cultures, CRP was done at 72 hours after admission, had a sensitivity of 76.9%, which is similar to findings in this study. The overall diagnostic accuracy of CRP in diagnosing neonatal sepsis has been reported to be 70%.[23,24] Some have reported that CRP was significantly higher among neonates with septicaemia due to GN sepsis than in those with GP septicaemia (75.0% v. 55.3%).[25] A retrospective cross-sectional study of 303 neonates and 88 positive blood cultures found no significant difference in CRP positivity between neonates with GN- and GP-positive cultures, similar to our findings.[26]
The common abnormality among all positive CSF cultures was high protein, and this abnormality was high among neonates, with cultures positive for fungi and GN bacteria. One study reported that CSF protein >90 mg/dL was found in 96% of neonates and levels >170 mg/dL were observed in 61% of neonates with meningitis, making this parameter a useful indicator to rule out meningitis.[27] Only 27% of neonates with positive CSF culture had high CSF-WCC and the difference was not statistically significantly different among the different types of organisms. In a large retrospective study from 150 neonatal intensive care units by Paediatrix Medical Group consisting of 14 017 lumbar punctures, GN meningitis was associated with high WCC compared with GP meningitis (median of 1217/mm3 v. 187/mm3; p=0.043).[28] A traumatic tap was observed in 46% of patients with positive CSF cultures. This is similar to the prevalence of 39.5 - 46.0% reported in other studies.[12,29,30] The proportion of neonates with high CSF WCC and CSF protein was higher in those with a bloody tap. These findings are similar to those reported by Lyons et al.,[31] who reported that the sensitivity of the CSF-WCC count was 87.9% among those with traumatic lumbar puncture and 58.6% among those with non-traumatic lumbar puncture.[31]
Despite the low yield in ancillary blood tests and culture results, these tests should still form part of the workup for sepsis in those neonates with suspected sepsis. These results can help guide the clinicians in determining the likelihood of the offending organism and guide the choice of antibiotics, especially in resource-limited settings where cultures are often not done, and if done, the results are often delayed or reported as negative despite a neonate having signs strongly suggestive of sepsis. These blood results should be interpreted in the context of signs and symptoms of sepsis. Normal ancillary test results cannot be relied upon to exclude sepsis.
Study strengths and limitations
The strength of the present study is that there was a large number of patients with positive cultures enrolled. Secondly, there was a high proportion of neonates with positive cultures who had ancillary laboratory tests performed at about the same time as positive cultures, and their results were available.
The limitations of the study are that it is a retrospective study; thus, not all ancillary test results could be analysed as some were missing. These results are from a single tertiary centre and therefore the results should be carefully considered before they are generalised to other centres as laboratory normal ranges might vary from laboratory to laboratory. Another limitation is that the demographics could not be captured, so we could not determine whether there is a difference in these abnormalities between premature and term infants and also classify organisms into early and late-onset sepsis. The lack of the group with negative cultures was another limitation in this study; therefore, parameters like sensitivity or specificity could not be determined for the different ancillary laboratory tests. More studies need to be performed in similar settings and these should include those with both negative and positive cultures.
Conclusion
In conclusion, CRP appears to be the most useful test for diagnosing sepsis as it is abnormal in more than two-thirds of patients with positive cultures. The absence of abnormalities in FBC, WBC-Diff cannot be used to exclude culture-confirmed sepsis, as less than 50% of patients with positive cultures have abnormalities in blood counts. Similarly, for CSF-WCC, normal CSF-WCC cannot be used to exclude positive CSF culture results, as only 27% of patients with meningitis have abnormal CSF count. Thus, a decision to stop empiric antibiotics must not be based on FBC or CSF cell counts alone but also on getting negative culture results. This highlights the importance of ensuring that cultures or other tests that can identify the organisms are performed and made available timeously and not to rely on ancillary laboratory tests only.
Declaration. This study was done in partial fulfilment of the degree requirements for Master of Medicine in Paediatrics.
Acknowledgements. National Health Laboratory Services of South Africa for giving us access to laboratory results from their Corporate Data Warehouse.
Author contributions. Equal contribution.
Funding. None.
Conflicts of interest. None.
References
1. Wynn JL. Defining neonatal sepsis. Curr Opin Paediatr 2016;28(2):135-140. https://doi.org/10.1097/mop.0000000000000315 [ Links ]
2. Napolitano ML. Sepsis 2018: Definitions and guideline changes. Surg Infect 2018;19(2):117-125. https://doi:10.1089/sur.2017.278. [ Links ]
3. Stoll BJ, Hansen NI, Adams-Chapman I, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004;292(19):2357-2365. https://doi.org/10.1001/jama.292.19.2357 [ Links ]
4. Haller S, Deindl P, Cassini A, et al. Neurological sequelae of healthcare-associated sepsis in very-low-birthweight infants: Umbrella review and evidence-based outcome tree. Eurosurveillance 2016;21(8):30143. https://doi.org/10.2807/1560-7917.es.2016.21.8.30143 [ Links ]
5. Manroe BL, Weinberg AG, Rosenfeld CR, Browne R. The neonatal blood count in health and disease. I. Reference values for neutrophilic cells. J Paediatr 1979;95(1):89-98. https://doi.org/10.1016/s0022-3476(79)80096-7 [ Links ]
6. Ree IMC, Fustolo-Gunnink SF, Bekker V, Fijnvandraat KJ, Steggerda SJ, Lopriore E. Thrombocytopenia in neonatal sepsis: Incidence, severity and risk factors. PLoS One 2017;12(10).e0185581. https://doi.org/10.1371/journal.pone.0185581 [ Links ]
7. Schmutz N, Henry E, Jopling J, Christensen RD. Expected ranges for blood neutrophil concentrations of neonates: The Manroe and Mouzinho charts revisited. J Perinatol 2008;28(4):275-281. https://doi.org/10.1038/sj.jp.7211916 [ Links ]
8. MacQueen BC, Christensen RD, Yoder BA, et al. Comparing automated v. manual leukocyte differential counts for quantifying the 'left shift' in the blood of neonates. J Perinatol 2016;36(10):843-848. https://doi.org/10.1038/jp.2016.92 [ Links ]
9. Bomela HN, Ballot DE, Cory BJ, Cooper PA. Use of C-reactive protein to guide duration of empiric antibiotic therapy in suspected early neonatal sepsis. Paediatr Infect Dis J 2000;19(6):531-535. https://doi.org/10.1097/00006454-200006000-00008 [ Links ]
10. Kestenbaum LA, Ebberson J, Zorc JJ, Hodinka RL, Shah SS. Defining cerebrospinal fluid white blood cell count reference values in neonates and young infants. Paediatrics 2010;125(2):257-264. https://doi.org/10.1542/peds.2009-1181 [ Links ]
11. Sarff LD, Platt LH, McCracken GH, Jr. Cerebrospinal fluid evaluation in neonates: Comparison of high-risk infants with and without meningitis. J Paediatr 1976;88(3):473-477. https://doi.org/10.1016/s0022-3476(76)80271-5 [ Links ]
12. Greenberg RG, Smith PB, Cotten CM, Moody MA, Clark RH, Benjamin DKJ. Traumatic lumbar punctures in neonates: Test performance of the cerebrospinal fluid white blood cell count. Paediatr Infect Dis J 2008;27(12):1047-1051. https://doi.org/10.1097/inf.0b013e31817e519b [ Links ]
13. Bhat MA, Bhat JI, Kawoosa MS, Ahmad SM, Ali SW. Organism-specific platelet response and factors affecting survival in thrombocytopenic very low birth weight babies with sepsis. J Perinatol 2009;29(10):702-708. https://doi.org/10.1038/jp.2009.72 [ Links ]
14. Guida JD, Kunig AM, Leef KH, McKenzie SE, Paul DA. Platelet count and sepsis in very low birth weight neonates: Is there an organism-specific response? Paediatrics 2003;111(6):1411-1415. https://doi.org/10.1542/peds.111.6.1411 [ Links ]
15. Bhat YR, Katakam PK, Lewis L, Purkayastha J. Prevalence and severity of thrombocytopenia in blood culture proven neonatal sepsis: A prospective study. Arch Paed Inf Dis 2018;6(2):e12471. https://doi.org/10.5812/pedinfect.12471 [ Links ]
16. Resch E, Hinkas O, Urlesberger B, Resch B. Neonatal thrombocytopenia - causes and outcomes following platelet transfusions. Eur J Paediatr 2018;177:1045-1052. https://doi.org/10.1007/s00431-018-3153-7 [ Links ]
17. Bedet A, Razazi K, Boissier F, et al. Mechanisms of thrombocytopenia during septic shock: A multiplex cluster analysis of endogenous sepsis mediators. Shock 2018;49(6):641-648. https://doi.org/10.1097/shk.0000000000001015 [ Links ]
18. Saboohi E, Saeed F, Khan RN, Khan MA. Immature to total neutrophil ratio as an early indicator of early neonatal sepsis. Pak J Med Sci 2019;35:241-246. https://doi.org/10.12669/pjms.35.L99 [ Links ]
19. Sarkar S, Bhagat I, Hieber S, Donn SM. Can neutrophil responses in very low birth weight infants predict the organisms responsible for late-onset bacterial or fungal sepsis? J Perinatol 2006;26(8):501-505. https://doi.org/10.1038/sj.jp.7211554 [ Links ]
20. Pauli I Jr., Shekhawat P, Kehl S, Sasidharan P. Early detection of bacteremia in the neonatal intensive care unit using the new BACTEC system. J Perinatol 1999;19(2):127-131. https://doi.org/10.1038/sj.jp.7200124 [ Links ]
21. Celik HT, Portakal O, Yigit §, Hascelik G, Korkmaz A, Yurdakök M. Efficacy of new leukocyte parameters v. serum C-reactive protein, procalcitonin, and interleukin-6 in the diagnosis of neonatal sepsis. Paediatr Int 2016;58(2):119-125. https://doi.org/10.1111/ped.12754 [ Links ]
22. Ahmed E, Rehman A, Ali MA. Validation of serum C-reactive protein for the diagnosis and monitoring of antibiotic therapy in neonatal sepsis. Pak J Med Sci 2017;33(6):1434-1437. https://doi.org/10.12669%2Fpjms.336.13927 [ Links ]
23. Hisamuddin E, Hisam A, Wahid S, Raza G. Validity of C-reactive protein (CRP) for diagnosis of neonatal sepsis. Pak J Med Sci 2015;31(3):527-531. https://doi.org/10.12669/pjms.313.6668 [ Links ]
24. Bapat SM. C-reactive proteins as diagnostic and prognostic indicator in neonatal sepsis. Int J Biomed Adv Res 2018;9(3):117-120. [ Links ]
25. Chacha F, Mirambo MM, Mushi MF, et al. Utility of qualitative C- reactive protein assay and white blood cells counts in the diagnosis of neonatal septicaemia at Bugando Medical Centre, Tanzania. BMC Paediatr 2014;14:248. https://doi.org/10.1186/1471-2431-14-248 [ Links ]
26. Sorsa A. Diagnostic significance of white blood cell count and C-reactive protein in neonatal sepsis; Asella Referral Hospital, South East Ethiopia. Open Microbiol J 2018;12:209-217. http://europepmc.org/abstract/MED/30069260 [ Links ]
27. Smith PB, Garges HP, Cotton CM, Walsh TJ, Clark RH, Benjamin DK Jr. Meningitis in preterm neonates: Importance of cerebrospinal fluid parameters. Am J Perinatol 2008;25(7):421-426. https://doi.org/10.1055/s-0028-1083839 [ Links ]
28. Smith PB, Cotten CM, Garges HP, et al. A comparison of neonatal Gramnegative rod and Gram-positive cocci meningitis. J Perinatol 2006;26(2):111-114. https://doi.org/10.1038/sj.jp.7211438 [ Links ]
29. Srinivasan L, Shah SS, Abbasi S, Padula MA, Harris MC. Traumatic lumbar punctures in infants hospitalised in the neonatal intensive care unit. Paediatr Infect Dis J 2013;32(10):1150-1152. https://doi.org/10.1097/inf.0b013e31829862b7 [ Links ]
30. Flett T, Athalye-Jape G, Nathan E, Patole S. Spinal needle size and traumatic neonatal lumbar puncture: An observational study (neo-LP). Eur J Paediatr 2020;179(6):939-945. https://doi.org/10.1007/s00431-020-03580-0 [ Links ]
31. Lyons TW, Cruz AT, Freedman SB, et al. Interpretation of cerebrospinal fluid white blood cell counts in young infants with a traumatic lumbar puncture. Ann Emerg Med 2017;69(5):622-631. https://doi.org/10.1016/j.annemergmed.2016.10.008 [ Links ]
 Correspondence:
Correspondence:
L Sono
linussono@gmail.com
Accepted 15 March 2021


{kind=link}
{kind=link}
{kind=link}