










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.16 no.1 Pretoria Abr. 2022
http://dx.doi.org/10.7196/sajch.2022.v16.i1.1849
RESEARCH
The emergence of Elizabethkingia meningoseptica infections in a quaternary-level paediatric intensive care unit in Durban, South Africa
R JassatI; PM JeenaII
IMBChB, FCPaed (SA); Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIPhD; Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Elizabethkingia meningoseptica is an emerging pathogen in adult intensive care settings, but there are limited data on infections in children.
OBJECTIVE: To describe the clinical presentation, risk factors for acquisition and management of infection in a quaternary-level paediatric intensive care unit (PICU).
METHODS: This was a retrospective observational analysis of E. meningoseptica infections at the Inkosi Albert Luthuli Central Hospital, Durban, from January 2017 to December 2019.
RESULTS: Eleven cases were identified, of which seven formed part of an outbreak cluster over an 11-week period. Enhanced infection control was implemented after the seventh case had been identified, resulting in immediate control. E. meningoseptica was identified exclusively from endotracheal aspirates. The clonality of outbreak isolates was confirmed from genotypic analysis. Five patients (45.4%) presented with nosocomial ventilator-associated pneumonia or systemic inflammatory response syndrome; one patient had possible meningitis. All patients were mechanically ventilated, with infection developing within 2-21 days. Exposure to multiple broad-spectrum antimicrobials (median: 5, range: 2-8) was identified as an acquisition risk. Seven of the nine patients who received targeted antimicrobial therapy survived. Of the untreated cases, one was discharged and the other died before isolate results were received. Overall, three patients (27%) demised.
CONCLUSION: E. meningoseptica infection is emerging as a potential cause of nosocomial pneumonia in the PICU setting, which may also extend to other paediatric critical care settings. Excessive antimicrobial use is a likely risk factor for acquisition. Effective infection control measures remain a cornerstone of limiting nosocomial spread.
Keywords: Elizabethkingia meningoseptica, intensive care unit, children
Elizabethkingia meningoseptica is regarded as an organism with low virulence in immunocompetent hosts. It is a non-fermenting, non-motile, oxidase-positive, Gram-negative bacillus.[1] Recent international data suggest that E. meningoseptica is an emerging pathogen in adult intensive care settings and is associated with significant morbidity and mortality. A retrospective review of a 22-month outbreak from an adult critical care unit in the United Kingdom showed monomicrobial E. meningoseptica infections to have a morbidity rate of 54%.[2] Smaller outbreaks in intensive care units (ICUs) have been reported in recent years.[3-5] An outbreak of five cases in two ICUs in Singapore,[3] three outbreak clusters involving both neonatal and non-neonatal paediatric patients in Ankara, Turkey,[4] and a four-case cluster in a paediatric intensive care unit (PICU) in Kuwait[5] have been described.
E. meningoseptica infection is generally rare in children, and occurs mainly in the immunosuppressed child. A review of the clinical presentation of E. meningoseptica infections in 275 symptomatic children from 1944 to 2017[6] showed that approximately three-quarters (74%) of these patients presented with meningitis, 23.7% with sepsis, 7.1% with bacteraemia and 6.7% with pneumonia. Risk factors for infection included an immunocompromised status, invasive procedures and prolonged hospitalisation, but the role of HIV infection or exposure has not been described. The bacterium's diverse antimicrobial-resistance properties, including chromosomal metallo-p-lactamases,[7] result in the lack of effective antimicrobial therapy for the infection. In a case series of 99 children and adults in Taiwan, 18% of the E. meningoseptica isolates were sensitive to gentamycin, 4% to imipenem and meropenem, and none to colistin.[8] Vancomycin, an antibiotic typically reserved for the management of Gram-positive infections, has been described as useful in the management of E. meningoseptica-related sepsis and meningitis, although effectiveness of treatment is improved through the addition of ciprofloxacin, linezolid or rifampicin.[9]
Cases of E. meningoseptica-related sepsis have emerged in children admitted to the PICU at Inkosi Albert Luthuli Central Hospital (IALCH), Durban, South Africa (SA) since 2017, including a cluster outbreak over an 11-week period in 2019. We describe the clinical presentation, risk factors for acquisition and management of these infections.
Methods
Study design and population
A retrospective observational analysis was conducted at a public hospital in Durban, SA, in response to a cluster of E. meningoseptica infections that occurred in the PICU between June and August 2019. Existing microbiological records from 1 January 2017 to 31 December 2019 were reviewed. We report on the institutional and provincial response to the outbreak, as well as the characteristics and outcomes of the affected patients.
Study setting
The 14-bed PICU comprises six single-bed, negative-pressure isolation cubicles (each with a handwashing station) and an open-plan unit of eight beds. The open-plan section has two handwashing stations. On average, 500 - 550 children are admitted to the PICU annually, and the case fatality rate is 15 - 18%. The nurse-to-patient ratio is maintained at 1:1, and the doctor-to-patient ratio is 1:6.
Routine care on admission
All admissions are routinely screened for bacterial, fungal and viral infection by a combination of blood, urine and endotracheal aspirate sampling after clinical assessment on the initial presentation. These samples are sent to the microbiology division of the National Health Laboratory Services (NHLS). Microbiologists conduct active surveillance, which includes daily monitoring of laboratory results, providing real-time microbiology advice and engaging with attending clinicians during daily ward visits.
Patients for whom positive E. meningoseptica cultures were reported while admitted to the PICU during the study period were identified using the microbiology database provided by the NHLS. The hospital's clinical records of these cases were accessed for data collection. Information collected included patient demographics, clinical course and physiological parameters, ICU interventions, details of the bacterial isolate, records of antimicrobial therapy, and outcomes at the time of discharge from the PICU
Primary outcome variables assessed were the clinical presentation, management and survival of patients who presented with E. meningoseptica infections in the PICU. Clinical syndromes, such as systemic inflammatory response syndrome (SIRS), ventilator-associated pneumonia (VAP), healthcare-associated infections and risk factors for acquisition of infection, including central line-associated bloodstream infections (CLABSI), were recorded All cases were assessed to ascertain whether they met the criteria for SIRS,[10] VAP[1l] and CLABSI to assess clinicopathological correlates of infection.
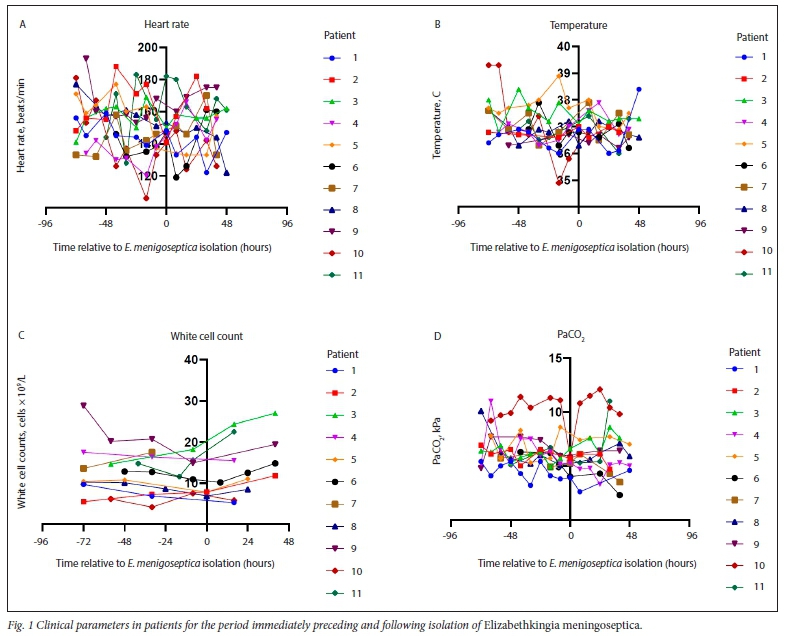
All physiological parameters are automatically captured for all patients admitted to the unit at regular intervals after admission. Physiological parameters in the 72 hours before and 48 hours after the identification of the bacterial isolates were analysed, together with the attending clinician's assessment, to determine the relevance of the isolates.
An on-site central sterilisation services department sterilises all procedural equipment. Laryngoscope blades, Magill forceps and face masks are disinfected in the unit (by soaking items in Endozime* AW Triple Plus, a multitiered enzymatic detergent with advanced proteolytic action). One of the professional nurses on duty is assigned to infection control. Two other professional nurses oversee infection control programmes and policy for the institution.
Microbiological investigation
All patient samples are processed at the microbiology laboratory on site at IALCH. Blood cultures are incubated using the BACTEC™ automated blood culture system (Becton Dickinson, USA). Both the identification of organisms and assessments of antimicrobial sensitivities are done using the VITEK* 2 microbial identification/ antibiotic susceptibility test system (BioMérieux, France). Pulse-field gel electrophoresis was used for genotyping of E. meningoseptica samples. The NHLS microbiological database was also used to evaluate the presence of both antecedent positive isolates (bacterial, virological or fungal) and co-infections at the time of initial E. meningoseptica isolation.
A register of antimicrobial agents and their duration of use during the period between admission and identification of infection was created from medication administration records.
Outbreak response
A cluster of cases satisfied the criteria for a nosocomial outbreak as outlined by the National Institute for Communicable Diseases.[12] Following identification of the seventh case, a support visit and investigation was conducted by the provincial infection and prevention control team. Environmental samples were taken from ventilator circuits, medication vials, high-touch equipment (including computer keyboards), laryngoscopes and other respiratory equipment used during resuscitation, and rinsing and handwashing areas. Swabs were also taken from the hands of attending clinical staff who had been in direct contact with the patients. Spatiotemporal relationships were defined to examine the pattern of spread within the unit. Viable E. meningoseptica isolates from the outbreak were sent for genotyping.
Data analysis
Descriptive statistics were used to summarise the data. Frequencies of numeric data are described as medians and percentages, whereas data on clinical parameters were collected over time and are displayed as spaghetti plots. All data analyses were performed using Microsoft Excel 2010 (version 14.0) and spaghetti plots were created using the Prism program (version 8.0) developed by GraphPad (GraphPad Software, USA).
Ethical considerations
The research protocol was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (ref. no. BREC/00001524/2020).
Results
General demographics
A total of 11 patient records of positive microbiological cultures for E. meningoseptica were found over the three-year study period. Six patients were female. The median age at admission was 5 months (range: 0.4 - 18 months). The primary diagnoses of the 11 cases were respiratory disease (n=5), surgical conditions (n=4), and one case each of cardiac and neurological disease. Six patients had undergone a surgical procedure during their admission, of whom three had multiple surgeries. Seven cases occurred during an 11-week outbreak in June - August 2019.
At the time of E. meningoseptica identification, all 11 patients had endotracheal and nasogastric tubes for a median duration of 5 days (range: 1-14 days) and 3.5 days (range: 1- 12 days), respectively Ten patients had urinary catheters (median duration: 4 days; range: 2-11 days) and peripheral arterial lines (median duration: 3 days; range: 2-13 days). Eight patients had central venous catheters (median duration: 4 days; range: 2-16 days) and peripheral intravenous cannulas (median duration: 2 days; range: 2-7 days) inserted. All patients were exposed to multiple broad-spectrum antimicrobials before specimens were collected for culture, with a median of five antibiotic treatments per patient (range: 2 - 8).
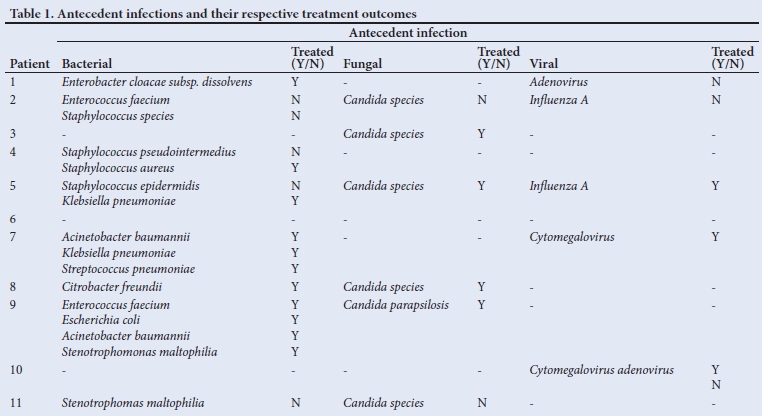
A summary of identified antecedent infections and their respective treatment outcomes for all 11 patients is given in Table 1.
Isolation of E. meningoseptica
The median time at which specimens were collected that positively cultured E. meningoseptica was 16 days after admission to the PICU (range: 2-21 days). All primary positive E. meningoseptica cultures were obtained from endotracheal aspirates. One patient had concurrent E. meningoseptica isolated from intraoperative peritoneal fluid. The antibiograms for the isolates consistently demonstrated resistance to carbapenems, aminoglycosides and colistin. All isolates were sensitive to vancomycin. Six patients had a monomicrobial E. meningoseptica infection, while the remainder had various bacterial co-infections. Cerebrospinal fluid was collected in five cases prior to the initiation of targeted antimicrobial therapy; one patient had a biochemical profile suggestive of bacterial meningitis but no organism was cultured.
Clinical presentation
All patients were on mechanical ventilation from the time of admission to when E. meningoseptica was identified. Eight patients clinical condition deteriorated in the 72 hours preceding the positive bacterial culture and five had accompanying radiological deterioration evident from serial chest radiographs. Of the three patients whose condition did not deteriorate, two were clinically stable and the other was improving. Monomicrobial infection with E. meningoseptica was demonstrated in five of the eight patients whose clinical condition deteriorated.
Fig. 1 provides a summary of clinical and laboratory parameters used to determine the incidence of attributable illness during the 72 hours preceding E. meningoseptica isolation and the subsequent 48 hours, for all 11 patients. Criteria for SIRS or VAP were met in five cases. Of the six patients with monomicrobial E. meningoseptica infection, criteria for SIRS and VAP were met in two cases. Among patients with bacterial co-infection (n=5), three met the criteria for VAP and two met the criteria for SIRS.
Treatment
Nine patients with E. meningoseptica infection received targeted antimicrobial therapy with vancomycin for a median duration of 7 days (range: 7-21 days). Of the remaining two patients, one died before the release of the culture result and the other was noted to have shown clinical improvement and antimicrobial therapy was not instituted. Eight of the nine treated cases had a poor clinical response to antimicrobial therapy and further microbiological screening was performed. Six of these patients demonstrated persistent positive E. meningoseptica culture from endotracheal aspirate specimens, while no growth was found in the samples from the remaining two patients. Repeated endotracheal aspirates were obtained at various intervals from the six patients with persistent positive E. meningoseptica cultures. The median time between the first and last positive cultures in these patients was 7 days (range: 5-17 days).
All five patients who showed bacterial co-infection at the time E. meningoseptica was isolated received targeted antimicrobial therapy.
Outcomes
Three patients died, but the remaining eight children were successfully discharged from the unit (mortality rate: 27%). The median age of children who died was 15 months, compared with an age of 6 months in those who survived (Table 2). In two of the children who died, E. meningoseptica infection persisted despite treatment with vancomycin. The other patient died before treatment could commence. Seven of the eight survivors received treatment, with clearance of E. meningoseptica shown in four, while clinical improvement was observed in the remaining three, without repeat cultures being required. The median duration of persistent E. meningoseptica infection was longer in patients who died (13.5 v 7 days).

The overall median duration of invasive ventilation (conventional mechanical ventilation and high-frequency oscillation ventilation) was 26 days (range: 12 - 58 days) while the median length of stay in the PICU was 32 days (range: 15 - 58 days). The median duration of ventilation (37 days) and length of stay (37 days) were longer in children who died than in survivors (23.5 days and 29 days, respectively) (Table 2).
Six patients were HIV exposed, of whom four were HIV positive. Two HIV-positive patients were on long-term antiretroviral therapy without virological suppression (HIV viral loads of 10 x 107 and 7.1 x 104 copies/mL, respectively). The two other HIV-positive patients were started on antiretroviral therapy during their stay in the PICU.
The median duration of invasive ventilation was generally longer in HIV-positive patients (35 days; range: 18-44 days) than in the two HIV-exposed but uninfected patients (ventilated for 20 and 21 days, respectively) and HIV-negative children (median: 26 days; range 13 - 58 days). HIV-positive children also stayed in the PICU longer (median: 39 days; range: 21 - 45 days) compared with HIV-exposed but uninfected children (20 days and 26 days, respectively) and HIV-negative children (median: 32 days; range: 15 - 58 days).
At least one other antecedent viral infection was noted for all the HIV-positive patients (adenovirus: n=2; cytomegalovirus: n=2; influenza A: n=1), whereas only one HIV-exposed but uninfected patient had had a viral infection in the antecedent period (influenza A). No antecedent viral infections were noted for HIV-unexposed patients. One patient died in each category of HIV status.
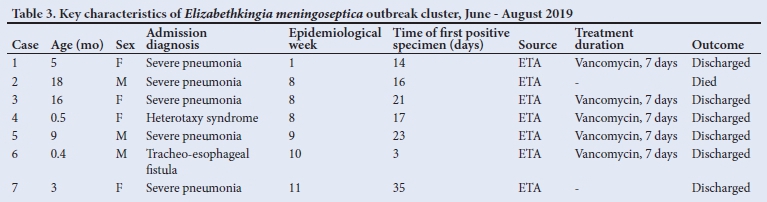
An outbreak investigation was conducted in response to the seven cases of E. meningoseptica infections that occurred in June - August 2019. The key characteristics of this outbreak are summarised in Table 3. The index patient was a 5-month-old HIV-positive, virologically unsuppressed female baby, who was admitted with severe pneumonia. E. meningoseptica was first identified from an endotracheal aspirate collected on day 14 of her PICU stay.
E. cloacae had been cultured from a previous endotracheal aspirate, which was successfully treated with meropenem. The spatiotemporal relationship of the sequence of case identification is summarised in Fig. 2.

Infection control interventions
None of the samples obtained from the environment and attending healthcare workers during the outbreak yielded any growth. The outbreak response team noted several observations related to poor hand hygiene practices by clinical staff, unavailability of appropriate hand sanitising agents in certain areas of the ward and absent labelling of disinfectant solutions for sterilising equipment at their initial visit. Patients from whom E. meningoseptica was cultured were relocated to a dedicated area in the PICU and measures to limit cross-contamination, including educating staff on hand hygiene, prohibiting sharing of equipment, and optimising cleaning of equipment and high-touch surfaces, were implemented. No further cases were subsequently identified.
Discussion
This study provides new evidence of the role of E. meningoseptica infections as a cause of nosocomial pneumonia in children with prolonged PICU stays in a lower middle-income setting. Respiratory illness is an unusual presentation of E. meningoseptica infection in the paediatric population, accounting for only 6.7% of symptomatic cases in recent literature spanning 73 years.[6] This finding is supported by the majority of patients having monomicrobial E. meningoseptica infections identified from an endotracheal aspirate, clinical deterioration in the 72 hours preceding identification, and presenting with at least two criteria for VAP. In adult studies, E. meningoseptica infections have been associated with nosocomial pneumonia.[2] Patients in our study were evaluated for meningitis, the usual clinical presentation of infection,[7] but only one case had this as a possible diagnosis.
A second major finding of the study was the emergence of an outbreak of E. meningoseptica in children admitted to the PICU. Despite limited data regarding E. meningoseptica outbreaks in PICUs,[1,4,5] recent evidence suggests that the bacterium is an emerging pathogen in adult ICU settings.[2,3,13] The clonal relationship between isolates during the outbreak period was confirmed from genotypic analysis. The pattern of spatiotemporal spread in the first four cases of the cluster favours an environmental point source.[2] Poor hand hygiene of healthcare workers may have contributed to the subsequent spread to two other quadrants of the PICU. Unfortunately, samples from the environment and clinical staff, which were negative, were obtained only after infection control measures had been implemented.
Several risk factors may have predisposed patients to the acquisition of nosocomial E. meningoseptica infection. Prolonged ventilation, ICU stay and antecedent antimicrobial therapy, together with a high number of antibiotics, were seen in a recent outbreak in a cardiothoracic PICU.[5] The prolonged poly-antimicrobial use seen in our study may have provided sufficient antibiotic pressure for this multidrug-resistant organism to dominate. No indwelling devices exceeded intervals outlined in established infection control guidelines (see Klompas et al.,[14] Marschall et a!.[15] and Gould et a!.[16]). The limited sample size of HIV-infected or exposed patients did not allow for meaningful conclusions to be reached with regard to the impact of HIV status on E. meningoseptica infection.
Treatments were guided by sensitivities. The prolonged duration of persistent infection in several cases where vancomycin monotherapy was used may point to the use of a combination of antimicrobials being more effective in clearing the organism, as has been previously suggested,[9] although no established guidelines exist. The finding also suggests that even though E. meningoseptica has long been regarded as an organism of low virulence in immunocompetent patients, it may be highly virulent in critically ill children. The overall mortality rate of 27% seen in this analysis is in keeping with that in other published studies.[5] Factors associated with a higher mortality risk included patients being older, antecedent viral infection, prolonged ventilation and ICU stay, and bacterial co-infection. A prolonged time to proven clearance of infection also contributed to mortality, as a median duration of 15.5 days of antibiotic use was noted in two of the three patients who died.
Study limitations
The small sample size of this study may call into question the generalisablity of the findings. This is unavoidable as the prevalence of E. meningoseptica remains relatively low in literature. As the study was retrospective in design, the analysis was limited by the quality of the recorded data. However, the electronic database used by the institution minimises the possibility of data loss, and all identified cases were analysed.
Conclusion
E. meningoseptica infection in the critically ill child is emerging as a potential cause of nosocomial infection, especially pneumonia. Prolonged and excessive antimicrobial use is a likely risk factor for acquisition. Outbreaks of E. meningoseptica infections are associated with significant case fatality rates. Effective infection control measures remain a cornerstone of limiting the occurrence of nosocomial infections.
Declaration. This manuscript was submitted as part of the requirements for an MMed (Paed) degree.
Acknowledgements. The authors thank Drs Y Mahabeer and S Buthelezi from the microbiology division of the NHLS for their assistance in compiling a record of E. meningoseptica cases and a summary of antimicrobial susceptibilities, and facilitating genotypic analysis of the outbreak isolates. We also thank the PICU team for allowing access to patient records.
Author contributions. PMJ conceptualised the study. RJ wrote the protocol, collected and analysed the data, and prepared the initial draft.
PMJ reviewed the initial draft prior to submission and supervised the entire study.
Funding. None.
Conflicts of interest. None.
References
1. Da Silva PS, Pereira GH. Elizabethkingia meningoseptica: Emergent bacteria causing pneumonia in a critically ill child. Pediatr Int 2013;55(2):231-234. https://doi.org/10.1111/j.1442-200x.2012.03650.x [ Links ]
2. Moore LSP, Owens DS, Jepson A, et al. Waterborne Elizabethkingia meningoseptica in adult critical care. Emerg Infect Dis 2016;22(1):9-17. https://doi.org/10.3201/eid2201.150139 [ Links ]
3. Balm MND, Salmon S, Jureen R, et al. Bad design, bad practices, bad bugs: Frustrations in controlling an outbreak of Elizabethkingia meningoseptica in intensive care units. J Hospital Infect 2013;85(2): 134-140. https://doi.org/10.1016/j.jhin.2013.05.012 [ Links ]
4. Ceyhan M, Yildirim I, Tekeli A, et al. A Chryseobacterium meningosepticum outbreak observed in 3 clusters involving both neonatal and non-neonatal pediatric patients. Am J Infect Control 2008;36(6):453-457. https://doi.org/10.1016/j.ajic.2007.09.008 [ Links ]
5. Hamza WS, Morsi SS, Al Roomi ES, Rotimi VO. Epidemiological analysis of Elizabethkingia meningoseptica infection cluster among mechanically ventilated pediatric intensive care patients. Int J Community Med Public Health 2018;5(8):8. https://doi.org/10.18203/2394-6040.ijcmph20182959 [ Links ]
6. Dziuban EJ, Franks JL, So M, Peacock G, Blaney DD. Elizabethkingia in children: A comprehensive review of symptomatic cases reported from 1944 to 2017. Clin Infect Dis 2017;67(1):144-149. https://doi.org/10.1093/cid/cixl052 [ Links ]
7. Pereira GH, De Oliveira Garcia D, Abboud CS, De Barros Barbosa VL, Da Silva PSL. Nosocomial infections caused by Elizabethkingia meningoseptica: An emergent pathogen. Braz J Infect Dis 2013;17(5):606-609. https://doi.org/10.1016/j.bjid.2013.02.011 [ Links ]
8. Hsu M-S, Liao C-H, Huang Y-T, et al. Clinical features, antimicrobial susceptibilities, and outcomes of Elizabethkingia meningoseptica (Chryseobacterium meningosepticum) bacteremia at a medical center in Taiwan, 1999-2006. Eur J Clin Microbiol Infect Dis 2011;30(10):1271-1278. https://doi.org/10.1007/sl0096-011-1223-0 [ Links ]
9. Jean SS, Hsieh TC, Ning YZ, Hsueh PR. Role of vancomycin in the treatment of bacteraemia and meningitis caused by Elizabethkingia meningoseptica. Int J Antimicrob Agents 2017;50(4):507-511. https://doi.org/10.1016/j.ijantimicag.2017.06.021 [ Links ]
10. Goldstein B, Giroir B, Randolph A. International Pediatric Sepsis Consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005;6(1):2-8. https://doi.org/10.1097/01.pcc.0000149131.72248.e6 [ Links ]
11. Hunter JD. Ventilator associated pneumonia. Postgrad Med J 2006;82(965):172-178. [ Links ]
12. National Institute for Communicable Diseases. Hospital infection outbreaks. https://www.nicd.ac.za/diseases-a-z-index/hospital-infection-outbreaks/ (accessed 12 December 2020). [ Links ]
13. Govindaswamy A, Bajpai V, Trikha V, Mittal S, Malhotra R, Mathur P. Multidrug resistant Elizabethkingia meningoseptica bacteremia - Experience from a level 1 trauma centre in India. Intractable Rare Dis Res 2018;7(3):172-176. https://doi.org/10.5582/irdr.2018.01077 [ Links ]
14. Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol 2014;35(8):915-936. https://doi.org/10.1086/677144 [ Links ]
15. Marschall J, Mermel LA, Fakih M, et al. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol 2014;35(7):753-771. https://doi.org/10.1086/676533 [ Links ]
16. Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA. Guideline for prevention of catheter-associated urinary tract infections 2009. Infect Control Hosp Epidemiol 2010;31(4):319-326. https://doi.org/10.1086/651091 [ Links ]
 Correspondence:
Correspondence:
R Jassat
riyaadhjassat@gmail.com
Accepted 1 March 2021


{kind=link}
{kind=link}
{kind=link}