










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Child Health
versión On-line ISSN 1999-7671
versión impresa ISSN 1994-3032
S. Afr. j. child health vol.15 no.4 Pretoria dic. 2021
http://dx.doi.org/10.7196/SAJCH.2021.v15i4.1827
RESEARCH
Physical activity and sedentary behaviours during pregnancy are associated with neonatal size at birth
A PrioreschiI; S V WrottesleyI; S A NorrisI, II
IPhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; Global Health Research Institute, School of Human Development and Health, and NIHR Southampton Biomedical Research Centre, University of Southampton, UK
ABSTRACT
BACKGROUND. Pregnancy is a crucial time to examine modifiable maternal behaviours associated with neonatal outcomes so that preventative measures can be taken against childhood obesity.
OBJECTIVES. This study aimed to examine the pathways through which maternal physical activity impacted neonatal size and body composition. Methods. A subsample of participants who had objectively measured physical activity data were included from a pregnancy cohort study. Sociodemographic data were collected at the first visit during pregnancy. Gestational weight gain (GWG) was calculated at each visit, and the presence of gestational diabetes, hypertension and HIV were assessed. Physical activity was measured using a hip-worn triaxial accelerometer, at 14 - 18 weeks' and 29 - 33 weeks' gestation. At delivery, gestational age, birthweight and length were measured and neonatal body composition was analysed. A structural equation model (SEM) was run with either weight-to-length ratio (WLR) or fat mass index (FMI) as the outcome.
RESULTS. A total of 84 participants were included in this study, and a subsample of neonates (n=45) also had FMI data. Most (66%) mothers presented as overweight or obese at their first visit, and gained on average 0.35 (19) kg per week. The SEM showed that only gestational age at delivery and sedentary time were positively associated with WLR. Step count was directly associated with GWG (β=-0.02, p=0.01), and with gestational age (β=0.16, p=0.04), and was therefore indirectly associated with decreased fetal abdominal circumference.
CONCLUSION. This study showed that increasing daily step count and decreasing sedentary behaviour could have beneficial effects on maternal health as well as delivery outcomes and neonatal size.
Pregnancy is a complex physiological state including a number of interrelated physiological processes; health behaviours prior to, and during, this time can have effects on both maternal and neonatal health. Some risk factors may even continue to impact on the offspring's health into adulthood.[1] Therefore this is a crucial period to examine modifiable maternal behaviours, and to determine which of these behaviours are associated with neonatal body size and composition outcomes so that preventative measures can be taken against childhood and later life obesity.
Previous research from a South African (SA) pregnancy cohort has shown that factors occurring pre conception and during pregnancy were associated with fetal growth, and in some cases with neonatal body composition (fat mass index (FMI)) or size (specifically weight-to-length ratio (WLR)). Specifically, preconception factors such as socioeconomic status (SES), whether or not the pregnancy was planned, and parity; and maternal lifestyle factors such as body mass index (BMI) at the start of pregnancy and diet have been associated with fetal and/or neonatal size.[2-4] Furthermore, pregnancy factors such as gestational diabetes mellitus (GDM), HIV status and treatment, and gestational weight gain (GWG), have also been associated with fetal growth and/or FMI or WLR. [2--4]Additionally, objectively measured physical activity during pregnancy was shown to be associated with GWG in a sub-sample of this population, but not with any delivery outcomes.[5] Various other potential predictors have been examined in relation to fetal growth and FMI or WLR in this population,[2-6] and we have therefore been able to develop a conceptual model showing the potential pathways through which maternal factors before and during pregnancy are related to FMI and/or WLR (Fig. 1).

However, differential effects have been shown when considering either WLR (size) or FMI (body composition) as the outcomes. While neonatal size is used as a predictor of childhood obesity and disease risk, newborn adiposity has been shown to be more indicative of metabolic programming and thus short- and long-term risk of obesity and disease risk.[7] Additionally, we have not yet studied the combined effects of all of these pathways in the same model, in order to determine which pathways are directly or indirectly associated with FMI or WLR. Furthermore, while maternal physical activity has been examined in relation to delivery outcomes, we have not yet examined how physical activity and sedentary behaviours are related to fetal growth or neonatal FMI or WLR; previous research on this topic shows varied results.[8-15] As maternal physical activity has been associated with GWG,[5]we suspect that physical activity patterns may play a role in the relationship between maternal health during pregnancy and neonatal body composition and size outcomes.
The present study therefore aims to examine the interrelationships between maternal biological and lifestyle factors, and fetal growth (Fig. 1) using a structural equation model (SEM) in order to specifically determine the pathways through which maternal physical activity behaviours influence (i) neonatal size (WLR), and (ii) body composition in a subsample who had FMI measures.
Methods
Study setting and participants
Participants were recruited from a prospective longitudinal pregnancy cohort study (the Soweto First 1000-Days Study (S1000)) which was conducted at the South African Medical Research Council (SAMRC)/ Wits Developmental Pathways for Health Research Unit (DPHRU), at the Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg, South Africa. The S1000 study has been explained in detail elsewhere,[2] but in brief, 1 017 naturally conceived pregnant women were enrolled from Soweto at <14 weeks' pregnant. Data were collected at six time-points during pregnancy (<14 weeks; 14 - 18 weeks; 19 -23 weeks; 24 - 28 weeks; 29 - 33 weeks and 34 - 38 weeks), as well as at delivery. For the purpose of this analysis, a subsample of participants who had objectively measured physical activity data as well as complete WLR data (n=84) were assessed;[5] and a subsample of these also had FMI data (n=45). Ethical clearance for the study was obtained from the University of the Witwatersrand's Human Research Ethics Committee (ref nos. M120524 and M130309). All study participants provided informed written consent prior to their inclusion in the study.
Maternal data
Sociodemographic data were collected at the first visit during pregnancy (<14 weeks' gestational age) in an interview using questionnaires administered by trained research assistants. Household socioeconomic status (SES) was estimated by scoring each participant according to the number of physical assets possessed out of a possible 11, based on standard items used in the Demographic and Health Surveys household questionnaire.[16, 17] Women self-reported their date of birth at enrolment, from which their age was calculated. Women reported whether their current pregnancy was planned or unplanned. Parity was defined as the number of previous births at a gestational age of 24 weeks or more - regardless of whether the infant was born alive or was stillborn. Self-reported HIV-status was collected at baseline as well as at each subsequent pregnancy visit, and confirmed using the results from the participant's antenatal clinic card. All HIV-positive participants were receiving antiretroviral treatment (ART) during the study.
Maternal anthropometry was collected at the first pregnancy visit by trained research assistants. Maternal height was measured to the nearest 1 mm at baseline using a wall-mounted stadiometer (Holtain, UK). A digital scale was used to measure maternal weight to the nearest 0.1 kg at each pregnancy visit. Weight at recruitment (<14 weeks) was used as a proxy for pre- pregnancy weight and, together with height, was used to calculate maternal BMI (weight (kg)/height (m2)).[18] GWG (kg/week) was calculated as (weight at final pregnancy visit - weight at recruitment)/weeks of follow-up). A two-hour 75 g oral glucose tolerance test (OGTT) was conducted at 24- 28 weeks' gestation in order to determine whether gestational diabetes mellitus (GDM) was present according to the World Health Organizations' (WHO) 2013 criteria.´19] Maternal blood pressure (mmHg) was measured at the fourth pregnancy visit (24- 28 weeks) using an Omron 6 automated machine (Kyoto, Japan). A 5-minute seated rest was observed before blood pressure measurements were taken. Seated blood pressure was measured three times on the right side, with a 2-minute interval between each measurement. Hypertension was defined as a systolic measure >140 and/or a diastolic measure >90 using the mean of the second and third readings according to the NICE guidelines (NG133, 2019).
Physical activity was measured using a hip-worn triaxial accelerometer (ActiGraph GT3X+, ActiGraph, Pensacola), at 14 18 weeks' and 29 - 33 weeks' gestation as described previously.[5] Non-wear time was defined as periods lasting three hours or longer where the standard deviation of acceleration in each axis remained below 5 mg[20] All data from midnight to 06h00 were excluded as sleep time. A day was considered valid if it contained at least seven hours of wear time, and a minimum of three valid days of wear time was required for a record to be included in this analysis. Acceleration was calibrated to local gravity,[20] following which a measure of overall PA volume was derived. Moderate to vigorous physical activity (MVPA) was set at a cut point >1 952 counts per minute, and presented as minutes/ valid day in trimesters one and three. The percentage of participants meeting WHO guidelines for physical activity (>150 MVPA/ week) was calculated and reported. Sedentary behaviour was set at a cut point of 100 counts per minute and presented as minutes/valid day in trimesters one and three. Steps per day were recorded in trimesters one and three by the accelerometer and reported as steps per day when counts per minute were higher than 100 (i.e. not sedentary behaviour).
Fetal ultrasonography
All participants had a pregnancy dating scan at the first visit (median (interquartile range (IQR)) 12 (11 -13) weeks) using a Philips HD-9 (Philips Ultrasound, Bothell, Washington) ultrasound machine.1211 Participants were invited for follow-up scans every five weeks at the following visits: 14 - 18 weeks', 19 - 23 weeks', 24 - 28 weeks', 29 - 33 weeks' and 34 - 38 weeks' gestation, and abdominal circumference, biparietal diameter, head circumference and femur length were recorded each time. [22] All five serial measurements of abdominal circumference from first to the third trimester of pregnancy were included in the analyses. These data were modelled using the Superimposition by Translation and Rotation (SITAR) as described previously,[21] and are represented as individual variation along the y-axis, giving an absolute deviation of each individual from the sample mean in the units of the measurement. While SITAR produces three parameters [23] - corresponding to the size, tempo and velocity of growth for each measurement, this study focuses only on the abdominal circumference size variable, as abdominal circumference has been shown to be the most reliable predictor of birthweight.[24, 25] Males and females were modelled together and the sex variable was included as an interaction term in the model to assess sex differences owing to previous analyses on this cohort demonstrating sex differences in fetal growth. [3]
Neonatal data
Gestational age at delivery (weeks) was calculated as: (duration of pregnancy follow-up (date of delivery - date of baseline ultrasound dating scan) + gestational age at baseline (days)). Birthweight and length were measured by trained research nurses within 24 hours of delivery. Where assessment within this window was not possible-for example, owing to the infant being admitted to hospital for observation - measurements were taken within 48 hours (18% of total sample). WLR ratio (kg/m) was calculated to represent the best anthropometric predictor of neonatal body composition at delivery.[26]
Neonatal body composition was analysed via either air displacement plethysmography (ADP) using the Peapod (Cosmed, USA) or dual-energy X-ray absorptiometry (DXA; Hologic DiscoveryA S/N 86254, APEX software version 4.0.2, Hologic Inc., USA) within the first month of life. Both of these measures have been described previously.[4] ADP was utilised when possible (n=32), but in cases where a neonate had only DXA measurements (n=13), fat mass and fat-free mass were converted to their ADP equivalent estimates as described previously.[4] FMI (kg/m3) was calculated from these estimates to describe adiposity in neonates.
Statistical methods
Data were analysed in STATA V13.0 (StataCorp., USA). All data are presented as mean (SD), median (IQR) or n (%). A p-value <0.05 was considered statistically significant. However, confidence intervals and beta coefficients are presented to determine the strength of the associations between variables. Maternal and fetal/ neonatal descriptive data were summarised and reported. Maternal predictors of physical activity, step count, and sedentary behaviour in trimesters one and three were determined using linear regression models. Thereafter, a SEM was developed based on the conceptual framework presented in Fig. 1 and the regression results. SEM is used to test and estimate the relationships between multiple variables when more than one pathway is suspected, and mediation or moderation may exist, and provides a complete picture of how all the variables interact with one another. The structural model defines the relationship between any composite latent variables and other observed variables. Two SEM models were run with either WLR or FMI (in a smaller subsample who had these data (n=45) as the outcome variables. Direct and indirect (whereby one variable is acting through another) effects were calculated, and total effects (overall model results when direct and indirect effects are combined) were presented with the pathways detailed.
Results
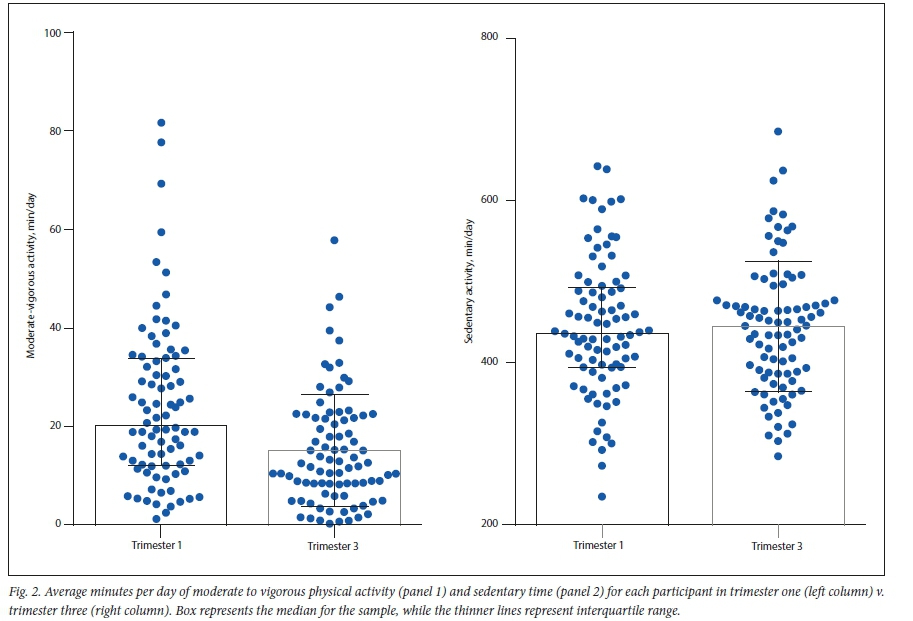
A total of 84 participants were included in this study. A post hoc power calculation showed that with the given sample size, we had >80% power in the regression models with 95% confidence. Table 1 shows the descriptive data for this sample. Mothers were on average 30 years old. Most (66%) mothers presented as overweight or obese at their first visit, and gained on average 0.35 (1.9) kg per week. Just under half (47%) of pregnancies were planned. In trimester one, 50% of mothers met the physical activity guidelines and 50% were accumulating 10 000 or more steps per day while, in trimester three, only 29% met the guidelines and only 41% were accumulating 10 000 or more steps per day. Average minutes per day of MVPA and sedentary time in trimester one v. trimester three are presented in Fig. 2. Neonates weighed on average 3 kg at birth, were born at a mean (SD) of 38 (SD=2) weeks' gestational age, and 51% were male.

The results from the linear regression models showed that in trimester one, parity trended towards a positive associated with sedentary time (β=16.75, p=0.05), and a negative association with step count (β=-764.39, p=0.07). In trimester three, only maternal age was positively associated with sedentary time (β=4.25, p=0.02), and negatively associated with MVPA (β=-0.59, p=0.02). BMI, GWG, GDM, HIV and SES were not associated with MVPA or sedentary time. However, GWG was negatively associated with step count in trimester three (β=-5865, p=0.02), whereby each kg increase in average weight gain per week was associated with nearly 6 000 fewer steps per day. None of the maternal factors was associated with the change in physical activity from trimester one to trimester three, yet maternal age was associated with less change in sedentary time (β= -1.24, p=0.02).
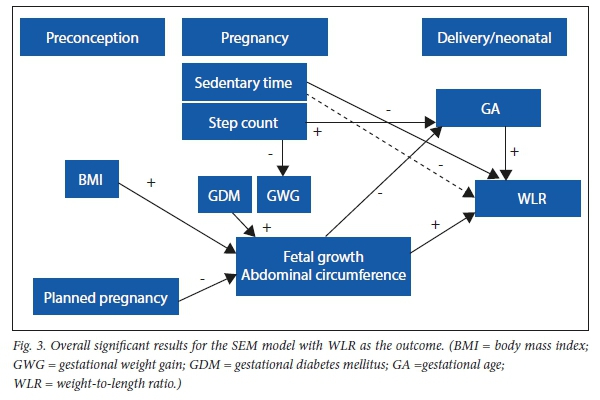
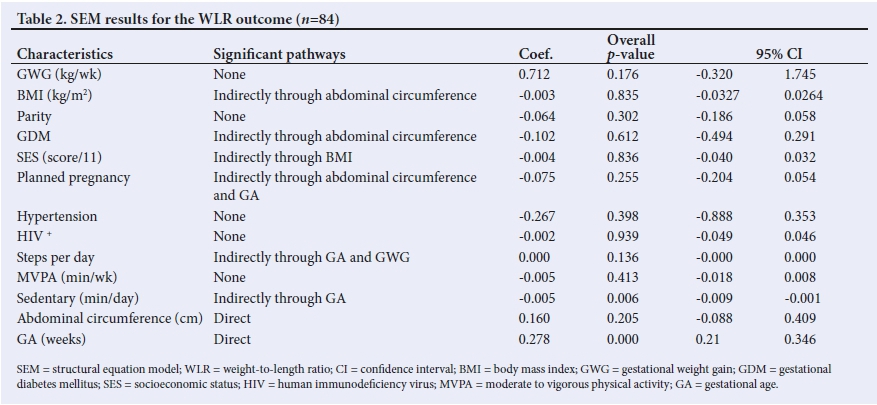
Finally, the SEM (model pathways shown in supplementary Fig. 1) showed that only GA (directly and positively) and sedentary time (negatively acting through GA), were associated with WLR (Table 1). While not directly related to WLR, step count (values were divided by 1 000 to provide β-coefficients >0) was directly associated with GWG (β=-0.02, p=0.01), and with GA (β= 0.16, p=0.04). Therefore, step count was indirectly (but not significantly) associated with decreased fetal abdominal circumference. Fetal abdominal circumference was also directly associated with GA (β=-0.82, p=0.02) and WLR (β=0.39, p<0.01), yet was not associated with WLR in the overall SEM results. BMI and GDM were also directly associated with increased abdominal circumference, and whether or not the pregnancy was planned was directly associated with decreased abdominal circumference. All significant pathways are shown in Fig. 3. When considering FMI as the outcome in a subsample of participants (n=45), only BMI was associated with FMI, indirectly through GA and abdominal circumference (β=0.02, p=0.04); shown in supplementary Table 1. Although there were no significant correlates of trimester one physical activity and sedentary behaviours, sensitivity analyses were run including trimester one physical activity and sedentary behaviours in the SEM models, yet these did not result in any changes to the pathways and so results are not presented.
Discussion
This study aimed to determine the interrelationship between maternal biological factors, maternal lifestyle behaviours and fetal growth, with neonatal size and body composition. We found that maternal sedentary behaviour during pregnancy was negatively associated with neonatal size (WLR), and that their step count was associated with decreased GWG and a higher gestational age. However, none of these factors was associated with neonatal FMI, indicating that activity behaviours may not affect adiposity deposition. Therefore, it seems that increased activity and decreased sedentary time are associated with later delivery of bigger neonates but not necessarily with higher adiposity in these neonates.
This study confirmed some of the pathways that have been previously examined in this population, while also elucidating some of the pathways through which these associations act. Specifically, we were able to clarify the detrimental effects of an increased BMI at the start of pregnancy for poor delivery outcomes and increased fetal and neonatal adiposity and size. Furthermore, the development of GDM predisposes neonates to the same detrimental delivery outcomes, and could thus compound the effects of entering pregnancy overweight. This study adds to the multitude of data describing the risks of entering pregnancy overweight or obese,[2,27-30] and further elucidates these relationships by showing that maternal BMI increases both fetal and neonatal adiposity - both of which have been linked to later life obesity.[2,10,15,31] In this study, 60% of mothers entered pregnancy overweight or obese - which is indicative of a population of young women at risk, who are transferring this risk on to the next generation.
While half of women entering pregnancy were sufficiently physically active, this had decreased to only 30% by the third trimester of pregnancy. This significant decrease in physical activity levels during pregnancy has been shown in other studies.[5,32,33]The maternal benefits of acquiring sufficient physical activity and decreasing sedentary time during pregnancy include lower GWG, decreased risk of GDM and hypertension, increased sense of wellbeing, and improvements in peripartum depression scores.[13,34,35] Yet there is less research describing the effects of physical activity during pregnancy on the offspring in utero or after delivery. Most studies have reported no adverse effects to the neonate and have therefore deemed exercise during pregnancy as safe - with the exception of maximal exertion training and potentially resistance training in a supine position.[9,10] A few studies have shown that exercise is related to neonatal birth sizet141 or to increased gestational age,[32] and that decreased sedentary time is related to decreased neonatal adiposity.[8] Associations with placental perfusion have also been observed.[10] Previous reviews of the literature have encouraged studies to include factors such as pre pregnancy BMI, GWG and GDM status.[10] The present study, when considering the interrelationship between those maternal factors, found that increased physical activity (step count) and decreased sedentary behaviour had beneficial effects on both maternal health and on neonatal size at delivery, while not increasing fat mass. Interestingly, all of these neonatal associations acted through fetal abdominal circumference - which is suggestive of metabolic programming of in utero abdominal adiposity. This aspect has not previously been studied in association with maternal physical activity.
In the present study, women who were accumulating more steps per day during the last trimester of pregnancy were likely to have gained less weight during their pregnancy, and their offspring were likely to be delivered later into gestation. However, MVPA did not show the same relationship. Other studies have shown that light physical activity has beneficial effects on placental perfusion, as well as fetal cardiac adaptability,[10] while higher intensity exercise can lead to transient fetal distress (while not causing any long-term detrimental effects).[910] As walking to accumulate steps is generally considered light to moderate intensity activity, it could present a safe, translatable and easy-to-achieve goal to improve pregnancy and fetal healthJ361 This would be a particularly important public health message, given that South Africa does not currently have any routine physical activity recommendations for pregnant women, or for women who are entering pregnancy overweight or obese. Conversely, sedentary behaviour was associated with a lower gestational age, and thus with decreased neonatal size. In trimester one, half of women were achieving the recommended 10 000 steps or more, while by trimester 3 this had decreased to 41%. As the SEM results showed that each extra 1 000 steps per day were associated with just over a day's extra gestation time and 200 g less GWG per week, it would be advisable to encourage women to accumulate as many steps as possible per day during their pregnancy. Furthermore, encouraging women to replace sedentary time with walking would potentially provide additional benefits to gestational age and to neonatal size at delivery. Additionally, increasing physical activity and decreasing sedentary time could decrease risk of GDM, and work towards decreasing obesity prevalence in this population of women and for any future offspring.[12,13,37] The combined effects of these behaviours are therefore highly relevant.
The present study is limited by the small sample size and by being constrained to one setting. However, a post hoc power calculation showed that with the given sample size, we had >80% power in the regression models with 95% confidence. Additionally, the longitudinal and precise objective measurement of physical activity and sedentary behaviour adds value and power to the analyses. The inclusion of repeated fetal growth measurements throughout pregnancy is unique to this study, and again adds power. Furthermore, by including maternal biological and behavioural correlates into the SEM model, we were able to unravel direct and indirect pathways through which these associations act.
In conclusion, this study has shown that a high maternal BMI at the start of pregnancy has deleterious effects on both fetal and neonatal body composition outcomes. Additionally, increasing daily step count and decreasing sedentary behaviour could have beneficial effects on both maternal health as well as on delivery outcomes and neonatal size. Walking is therefore recommended as a safe and accessible means to improve pregnancy health, while also potentially decreasing risk of GDM and obesity.
Declaration. The authors assert that all procedures contributing to this work comply with the ethical standards of the Human Research Ethics Committee of the University of the Witwatersrand and with the Helsinki Declaration of 1975, as revised in 2008; and have been approved by the Human Research Ethics Committee of the University of the Witwatersrand.
Acknowledgements. None.
Author contributions. All authors contributed to the study conception and design. Material preparation and data collection were performed by AP and SVW. Data analysis was performed by AP. Funding and resources were provided by SAN. The first draft of the manuscript was written by AP, and all authors read and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding. GHR Project:17/63/154 - The NIHR Global Health Research Group on leveraging improved nutrition preconception, during pregnancy and postpartum in sub-Saharan Africa through novel intervention models, Southampton 1000 DaysPlus Global Nutrition, at the University of Southampton.
Conflicts of interest. None.
References
1. Hanson MPG. Developmental origins of noncommunicable disease: population and public health implications. Am J Clin Nutr 2011;94:1754S-1758S. [ Links ]
2. Prioreschi A, Wrottesley SV, Said-Mohamed R, Nyati L, Newell M-L, Noms SA. Understanding how maternal social and biological factors are related to fetal growth in an urban South African cohort. J Dev Origins Health Dis 2020:1-9. https://doi.org/10.1017/s2040174420000045 [ Links ]
3. Macaulay S, Munthali RJ, Dunger DB, Noms SA. The effects of gestational diabetes mellitus on fetal growth and neonatal birth measures in an Africancohort. Diabet Med 2018;35( 10): 1425-1433. https://doi.org/10.1111/dme.13668 [ Links ]
4. Wrottesley SV, Ong KK, Pisa PT, Noms SA. Maternal traditional dietary pattern and antiretroviral treatment exposure are associated with neonatal size and adiposity in urban, black South Africans. Br J Nutr 2018;120(5):557-566. https://doi.org/10.1017/s0007114518001708 [ Links ]
5. Watson ED, Brage S, White T, et al. The influence of objectively measured physical activity during pregnancy on maternal and birth outcomes in urban black South African women. Matern Child Health J 2018;22(8):1190-1199. https://doi.org/10.1007/s10995-018-2504-3 [ Links ]
6. Wrottesley S, Prioreschi A, Kehoe S, Ward K, Noms S. A maternal 'mixed, high sugar' dietary pattern is associated with fetal growth. Matern Child Health J 2019;16(2):e12912. https://doi.org/10.1111/mcn.12912 [ Links ]
7. Donnelly JM, Lindsay KL, Walsh JM, Horan M, Molloy EJ, McAuliffe FM. Fetal metabolic influences of neonatal anthropometry and adiposity. BMC Pediatrics 2015;15:175. https://doi.org/10.1186/s12887-015-0499-0 [ Links ]
8. Van Poppel MNM, Simmons D, Devlieger R, et al. A reduction in sedentary behaviour in obese women during pregnancy reduces neonatal adiposity: The DALI randomised controlled trial. Diabetologia 2019;62(6):915-925. https://doi.org/10.1007/s00125-019-4842-0 [ Links ]
9. Beetham KS, Giles C, Noetel M, Clifton V, Jones JC, Naughton G. The effects of vigorous intensity exercise in the third trimester of pregnancy: A systematic review and meta-analysis. BMC Pregn Childbirth 2019;19(1):281. https://doi.org/10.1186/s12884-019-2441-1 [ Links ]
10. Bauer I, Hartkopf J, Kullmann S, et al. Spotlight on the fetus: How physical activity during pregnancy influences fetal health: A narrative review. BMJ Open Sport Exerc Med 2020;6(1): e000658. https://doi.org/10.1136/bmjsem-2019-000658 [ Links ]
11. Baena-García L, Ocón-Hernández O, Acosta-Manzano P, et al. Association of sedentary time and physical activity during pregnancy with maternal and neonatal birth outcomes. The GESTAFIT Project. Scand J Med Sci Sports2019;29(3):407-414. https://doi.org/10.1111/sms.13337 [ Links ]
12. Badon SE, Littman AJ, Chan KCG, Williams MA, Enquobahrie DA. Maternal sedentary behavior during pre-pregnancy and early pregnancy and mean offspring birth size: A cohort study. BMC Preg Childbirth 2018;18(1):267. https://doi.org/10.1186/s12884-018-1902-2 [ Links ]
13. Fazzi C, Saunders DH, Linton K, Norman JE, Reynolds RM. Sedentary behaviours during pregnancy: A systematic review. Int J Behav Nutr Phys Act 2017;14(1):32. https://doi.org/10.1186/s12966-017-0485-z [ Links ]
14. Bisson M, Tremblay F, St-Onge O, et al. Influence of maternal physical activity on infant's body composition. Pediatr Obes Aug 2017;12 Suppl 1:38-46. https://doi.org/10.1111/ijpo.12174 [ Links ]
15. Perkins C, Pivarnik J, Paneth N, Stein A. Physical activity and fetal growth during pregnancy. Obstet Gynecol 2007;109(1):81-87. [ Links ]
16. Griffiths PL, Johnson W, Cameron N, Pettifor JM, Noms SA. In urban South Africa, 16 year old adolescents experience greater health equality than children. Econ Hum Biol 2013;11(4):502-514. https://doi.org/10.1016/j.ehb.2013.05.004 [ Links ]
17. Kagura J, Adair LS, Pisa PT, Griffiths PL, Pettifor JM, Noms SA. Association of socioeconomic status change between infancy and adolescence, and blood pressure, in South African young adults: Birth to Twenty Cohort. BMJ Open 2016;6(3): e008805. https://doi.org/10.1136/bmjopen-2015-008805 [ Links ]
18. Krukowski RA, West DS, DiCarlo M, et al. Are early first trimester weights valid proxies for preconception weight? BMC Preg Childbirth 2016;16:357. [ Links ]
19. World Health Organization. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy. 2013. WHO/NMH/MND/13.2 http://www.who.int/diabetes/publications/Hyperglycaemia_In_Pregnancy/en/ (accessed 29 August 2018). [ Links ]
20. Van Hees VT, Fang Z, Langford J, et al. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J Appl Physiol 2014;117(7):738-744. https://doi.org/10.1152/japplphysiol.00421.2014 [ Links ]
21. Macaulay S, Buchmann EJ, Dunger DB, et al. Reliability and validity of last menstrual period for gestational age estimation in a low-to-middle-income setting. J Obstet Gynaecol Res 2019;45( 1):217-225. https://doi.org/10.1111/jog.13801 [ Links ]
22. Papageorghiou AT, Ohuma EO, Altman DG, et al. International standards for fetal growth based on serial ultrasound measurements: The Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. Lancet 2014;384:869-879. [ Links ]
23. Cole T, Donaldson M, Ben-Shlomo Y. SITAR-a useful instrument for growth curve analysis. Int J Epidemiol 2010;39(6):1558-1566. [ Links ]
24. Kayem G, Grange G, Breart G, Goffinet F. Comparison of fundal height measurement and sonographically measured fetal abdominal circumference in the prediction of high and low birth weight at term. Ultrasound Obstet Gynecol 2009;34(5):566-571. https://doi.org/10.1002/uog.6378 [ Links ]
25. Bamberg C, Hinkson L, Henrich W. Prenatal detection and consequences of fetal macrosomia. Fetal Diag Ther 2013;33(3):143-148. https://doi.org/10.1159/000341813 [ Links ]
26. Villar J, Puglia FA, Fenton TR, et al. Body composition at birth and its relationship with neonatal anthropometric ratios: The newborn body composition study of the INTERGROWTH-21st project. Pediatr Res 2017;82(2):305-316. https://doi.org/10.1038/pr.2017.52 [ Links ]
27. Stubert J, Reister F, Hartmann S, Janni W. The risks associated with obesity in pregnancy. Dtsch Arztebl Int 2018;115(16):276-283. https://doi.org/10.3238/arztebl.2018.0276 [ Links ]
28. Prioreschi A, Wrottesley S, Draper CE, et al. Maternal and early life nutrition and physical activity: Setting the research and intervention agenda for addressing the double burden of malnutrition in South African children. Glob Health Action 2017;10(1):1301085. https://doi.org/10.1080/16549716.2017.1301085 [ Links ]
29. Poston L, Caleyachetty R, Cnattingius S, et al. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diab Endocr 2016;4(12):1025-1036. https://doi.org/10.1016/s2213-8587(16)30217-0 [ Links ]
30. Rahman MM, Abe SK, Kanda M, et al. Maternal body mass index and risk of birth and maternal health outcomes in low- and middle-income countries: A systematic review and meta-analysis. Obes Rev 2015;16:758-770. [ Links ]
31. Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: Physiology or pathophysiology? Physiol Rev 2014;94(4):1027-1076. https://doi.org/10.1152/physrev.00029.2013 [ Links ]
32. Watson ED, Brage S, White T, et al. The influence of objectively measured physical activity during pregnancy on maternal and birth outcomes in urban black South African women. Matern Child Health J 2018; 22(8):1190-1199. https://doi/10.1007/s10995-018-2504-3 [ Links ]
33. Pathirathna ML, Sekijima K, Sadakata M, Fujiwara N, Muramatsu Y, Wimalasiri KMS. Effects of physical activity during pregnancy on neonatal birth weight. Sci Rep 2019;9(1):6000. https://doi.org/10.1038/s41598-019-42473-7 [ Links ]
34. Nakamura A, van der Waerden J, Melchior M, Bolze C, El-Khoury F, Pryor L. Physical activity during pregnancy and postpartum depression: Systematic review and meta-analysis. J Affect Disord 2019;246:29-41. https://doi.org/10.1016/j.jad.2018.12.009 [ Links ]
35. Pearson JT, Watson ED, Lambert EV, Micklesfield LK. The role of physical activity during pregnancy in determining maternal and foetal outcomes. S Afr J Sports Med 2015;27(4):93-96. https://doi.org/10.17159/2078-516x/2015/v27i4a440 [ Links ]
36. Connolly CP, Conger SA, Montoye AHK, et al. Walking for health during pregnancy: A literature review and considerations for future research. J Sport Health Sci 2019;8(5):401-411. https://doi.org/10.1016/jjshs.2018.11.004 [ Links ]
37. Anjana RM, Sudha V, Lakshmipriya N, et al. Physical activity patterns and gestational diabetes outcomes - the wings project. Diabetes Res Clin Pract 2016;116:253-262. https://doi.org/10.1016/j.diabres.2016.04.041 [ Links ]
 Correspondence:
Correspondence:
A Prioreschi
alessandra.prioreschi@wits.ac.za
Accepted 2 February 2021.


{kind=link}
{kind=link}
{kind=link}