










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.15 no.3 Pretoria Set. 2021
http://dx.doi.org/10.7196/SAJCH.2021.v15.i3.1777
RESEARCH
Incidence of preterm births in a referral teaching hospital in Ghana: What is the role of maternal age, parity, gravidity and stress during pregnancy?
E OtiekuI; AP FennyII; A-K LabiIII; U EnemarkIV
IMPhil; Institute of Statistical, Social and Economic Research, University of Ghana, Accra, Ghana
IIPhD; Institute of Statistical, Social and Economic Research, University of Ghana, Accra, Ghana
IIIPhD; Department of Medical Microbiology, University of Ghana Medical School, University of Ghana, Accra, Ghana
IVPhD; Department of Public Health, Faculty of Health, Aarhus University, Denmark
ABSTRACT
BACKGROUND. Preterm births (PTBs) notably contribute to neonatal morbidity and mortality in neonatal intensive care units (NICUs). Therefore, an examination of maternal risk factors is essential in reducing the incidence of PTB.
OBJECTIVE. To estimate maternal risk factors of PTBs with subsequent admission to the NICU.
METHODS. We interviewed 357 mothers who gave birth at the Korle-Bu Teaching Hospital (KBTH) and their neonates admitted to the hospital's NICU. A binary multivariate logistic regression model was used to analyse the odds ratios of each predictor variable.
RESULTS. The incidence of PTBs associated with admission to the NICU was 70%. From our estimation model, maternal parity emerged as the single most influential risk factor of preterm neonates who subsequently had to be admitted to the NICU, contributing to a significant 17.3% of the model fit compared with 12.9% for maternal stress and 1% for maternal age. Approximately 35% of the mothers did not attend the minimum number of antenatal care (ANC) visits (four) recommended by the Ghana Ministry of Health, which may have increased their risk of PTB.
CONCLUSION. The most appropriate intervention to reduce the high risk of PTB is for expectant mothers to attend ANC during their pregnancy. Health professionals rendering ANC services should also educate mothers on how to avoid or manage stress during pregnancy to reduce the incidence of PTB.
The anticipated joy of a newborn's birth often outweighs expectant mothers' discomfort during delivery. However, the birth of preterm neonates may bring emotional and psychological stress related to uncertain survival of the neonate and the costs associated with caring for preterm neonates in an intensive care unit (ICU).[1-3] By standard international definition, preterm neonates are those born before 37 weeks' gestation.[4,5] Such neonates are usually classified as extremely preterm (<28 weeks of gestation), very preterm (28 - 32 weeks' gestation) and late preterm (32 - 36 weeks' gestation). In 2010, preterm births (PTBs) were estimated at 14.9 million globally and considered the second highest cause of under-five mortality after pneumonia.[5]
The incidence of PTBs varies across regions and population groups (e.g. 5.8% in Jordan,[6] 9.2% in the USA,[7] and 18.3% in Kenya[8]). The average incidence in low-income countries is 11.8%, 11.3% in lower middle-income countries and 9.3% in high-income countries.[9] However, the incidence of PTBs is likely to be underestimated in low-resourced countries in Asia and Africa because of limited data and a notable number of unreported home deliveries that occur because of poverty and other factors.[9]
PTBs are often medically associated with a number of factors related to uterine complications and multiple pregnancies.[10,11] However, some studies also suggest a strong association between maternal history and the incidence of PTB,[12,13] with the age of the mother identified as a notable factor.[14-16] For example, a recent study in Jordan found that women younger than 20 years and those older than 35 years have a higher risk of PTB.[7]Empirically, there is little or no statistical evidence of the association between maternal parity and the risk of PTB in Ghana. Nonetheless, studies elsewhere show an unclear association between these factors.[13,17]
Empirically, there is little or no statistical evidence of the association between maternal parity and the risk of PTB in Ghana. Nonetheless, studies elsewhere show an unclear association between these factors.[13,17]
The underlying hypothesis is that expectant mothers with previous experience of managing a pregnancy and who experienced successful full-term delivery are likely to recognise the signs of PTB.[13]
Similarly, studies have found that lower uptake of antenatal care results in a high risk of PTB.[7] In Ghana, a minimum of four antenatal clinic visits are recommended by the ministry of health, in line with recommendations by the World Health Organization, to help prevent adverse birth outcomes, including PTB.[18,19]
The global epidemiology report on PTBs suggests that maternal stress during pregnancy contributes to spontaneous PTB and associated under-five mortality.[5] However, it is unclear how maternal stress during pregnancy should be defined and how it is associated with PTB, especially in low- and middle-income countries.[5,17,20] Clarifying the definition and investigating the association between maternal stress and PTB in Ghana can therefore add to existing knowledge. For example, if such an association exists, the study could help provide additional strategies to reduce the global incidence of PTB.
The neonatal ICU (NICU) at the Korle-Bu Teaching Hospital (KBTH) in Ghana is a small unit operated under the Department of Child Health. It has an average daily capacity of 100 neonates and absorbs more than 80% of neonates born with complications at KBTH. The unit runs a 24-hour service with an average doctor-to-neonate ratio of 1:20 and a nurse-to-neonate ratio of 1:10. The NICU is under increasing pressure to admit a higher number of complicated cases, but resources are limited and the unit operates at capacity.[9] Preventing the need for admission to the NICU is therefore of interest. As PTBs account for a large part of NICU admissions, identification of modifiable predictors of PTB will help to provide distinct recommendations to reduce the incidence of preterm neonates having to be admitted to the NICU and consequently reduce pressure on the unit and expense burdens for mothers. Data reported in the current analysis were collected as part of an earlier study on the cost of neonatal sepsis at the NICU of KBTH.[21] The focus on maternal factors (i.e. maternal age, parity, gravidity and stress) as predictors of PTB in the analysis reported here relates to limited information being available on how these factors affect the risk of PTB and admission to the NICU in the Ghanaian setting.
Methods
Study population and sample size
The study population comprised mothers whose neonates were admitted to the NICU. KBTH is Ghana's major tertiary referral hospital and admits patients only upon referral from another institution or for critical emergencies. All mothers of neonates admitted to the NICU between October 2017 and January 2018 were prospectively enrolled in the study. Of the 357 women who gave birth at KTBH, 251 delivered live preterm neonates, who were admitted to the NICU. Informed consent was sought from all the participants.
Data collection
Data on mothers' age, parity, gravidity, number of ANC visits and employment status at the time of pregnancy were obtained from the clinical admissions and discharge records at the NICU. Data on maternal stress during pregnancy and the completed number of ANC contacts with healthcare professionals were obtained during postpartum interviews with participants as part of a questionnaire originally designed to obtain data on the cost of neonatal sepsis. We used four indicators to measure maternal stress, namely whether mothers had experienced any of the following: (i) unwanted pregnancies; (ii) economic hardship; (iii) family pressure of any kind; or (iv) lack of spousal support during pregnancy.[20]
Statistical analysis
A binary logistic regression estimation model (version 13; Stata Corp., USA) was used to estimate the risk of preterm deliveries in the sample, expressed as an odds ratio (OR). We constructed a binomial variable for preterm delivery as the dependent variable. All neonates delivered after <37 weeks' gestation were classified as preterm and assigned a code of 1. Those born at or later than 37 weeks' gestation were classified as term births and assigned a code of 0.
We considered maternal stress as a predictor of PTB. It was defined to mean stress gained from an unwanted pregnancy, economic hardship, family pressure of any kind, or lack of spousal support during the pregnancy. We created a stress severity score (SSS) to measure the degree of stress experienced by the mother during her pregnancy, ranging from little stress (SSS1) to severe stress (SSS4). A score of zero was used as a reference point to denote no stress.
A gravidity score (G1 - G5) was used to denote the number of times a participant has been pregnant, with the number of pregnancies indicated by the subscript number. Maternal parity was coded similarly (P0 - P4) to indicate the number of times a participant has delivered a live baby or stillborn by 24 weeks of gestation or later. A parity score of P0 means a participant has no history of delivering a live or stillborn baby.
Maternal age was coded as follows: 0 for women aged 20 - 35 years; 1 for women younger than 20 years; and 2 for women older than 35 years. The age group 20 - 35 years was taken as the reference group.
We improved the fitness of the model by also including other predictors of PTB, such as maternal history of preterm deliveries (yes=1; no=0), sex of the neonate (male=1; female=0), and whether or not respondents attended the minimum number of recommended ANC visits (yes=1; no=0).
The approach to the model was twofold. We first derived OR at α=0.05 and a 95% confidence interval (CI), following the estimation example of Abdel-Razaq et al.,[7]and then hypothesised that each predictor variable (mother's age, gravidity, stress and parity) would have a unique association with the dependent variable (PTB). As a result, both forward and backward stepwise logistic regression was performed to test for significant change in the model fit. In the forward stepwise approach, predictors were selected based on their level of association with PTB, starting with maternal stress as the modifiable predictor and followed by parity, maternal age and the three remaining adjusted variables. In the backward selection, we omitted predictors with no or little association with PTB from the model in descending order of significance to identify which predictors contributed most to the fit of the model.
Ethical considerations
The study protocol was approved by the KBTH Institutional Review Board (ref. no. KBTH-IRB/ 00036/2017 and KBTH-IRB/00025/2017).
Results
Descriptive statistics
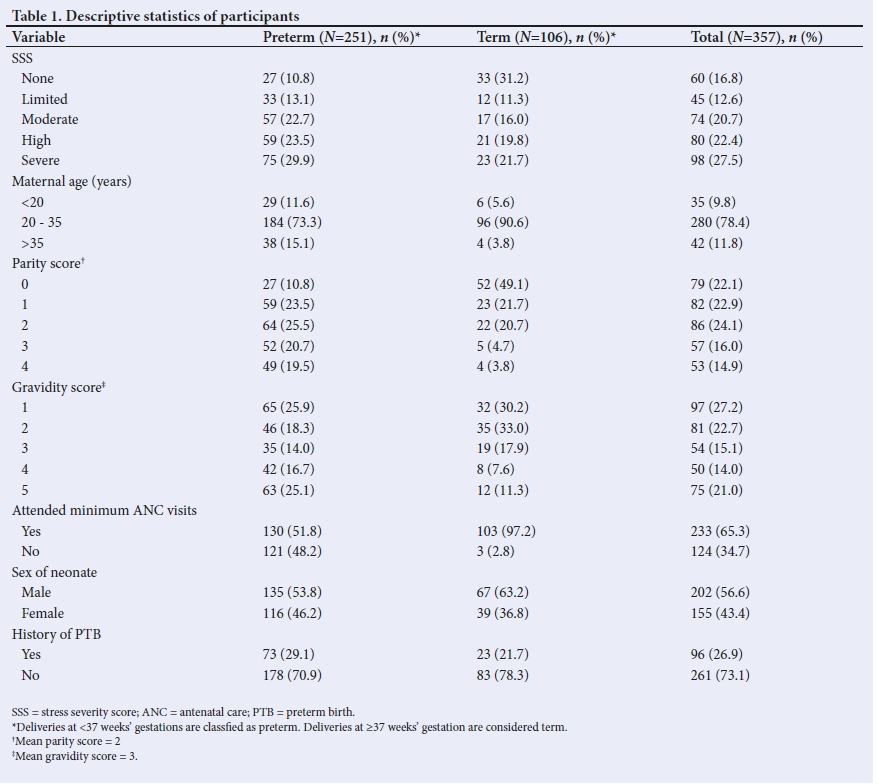
Approximately 70% of neonates admitted to the NICU during the study period were born preterm, with 83.6% of these being late preterm (32 - 36 weeks of gestation). The estimated average birth weight of preterm neonates was 2.1 kg. Approximately 65% of the respondents completed the recommended four antenatal clinic visits (Table 1). However, almost all mothers (97.2%) who delivered term neonates attended all four ANC visits, compared with 51.8% of mothers with preterm deliveries. Economic hardship was reported as a source of stress during pregnancy by 37.2% of the participants. Lack of spousal support was reported as a source of stress by 25.1% of participants and family pressure by 14.7%. Unwanted pregnancy was reported as a source of stress by 6.2% of the participants. Slightly more than a quarter of participants (27.5%) experienced severe stress, meaning they were exposed to all four stress factors; 16.8% of participants experienced no stress. The average gravidity and parity scores were 2 and 3, respectively.
Of the mothers with PTBs, 29.9% experienced severe stress, whereas 10.8% reported having experienced no stress. The highest proportion of preterm deliveries (73.3%) was reported among women aged 20 - 35 years.
Multivariate logistic regression
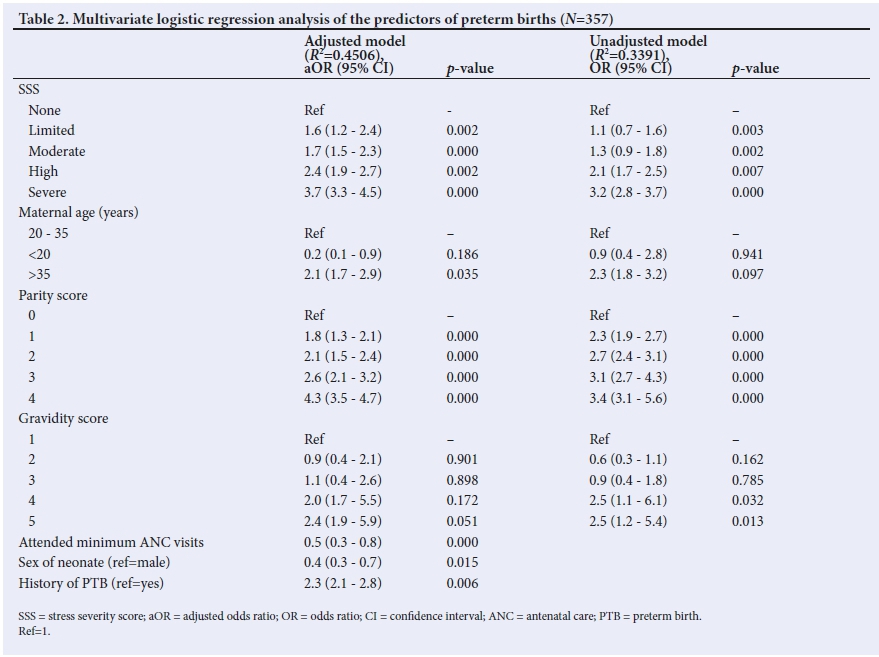
In both the adjusted and unadjusted models, maternal stress and maternal parity were positively associated with PTB (Table 2). With reference to maternal parity, the highest adjusted OR (aOR) was recorded among mothers with a parity score of 4 (aOR 4.3). Similarly, the aOR for mothers who reported severe maternal stress during pregnancy (aOR 3.7) compared with that of mothers who reported no or limited stress (aOR 1.6) suggests a significant positive association between PTB and maternal stress. Maternal history of PTB (aOR 2.3) and a gravidity score of 5 (aOR 2.4) also had a significant positive association with PTB. The regression analysis shows that attending the recommended minimum of four ANC visits significantly reduces the risk of PTB (aOR=0.5).Maternal age >35 years emerged as a significant positive predictor of PTB in the adjusted model (aOR=2.1) but not in the unadjusted model (Table 2). The predictors included in the adjusted model accounted for 45.1% of the model fit (R2=0.4506) compared with 33.9% in the unadjusted model (R2=0.3391). Stepwise logistic regression showed maternal parity alone to account for a significant proportion (17.3%) of the adjusted model fit, compared with 11.8% for maternal stress, 3.8% for gravidity and 1% for maternal age.
Discussion
The high incidence of PTBs has increasingly gained attention in epidemiological and public health discourses owing to its association with under-five morbidity and mortality. Evidence from the present study reinforces reports on the multidimensional risk factors of PTB.[7,19,22] Consistent with other studies,[23] we found that maternal age >35 years was positively associated with the delivery of preterm neonates who were subsequently admitted to the NICU. However, unlike a recent study from Jordan, we found no statistically significant association between maternal age <20 years and PTB.
The comparative difference may be ascribed to differences in environmental and demographic factors such as maternal height, race, body mass index, alcohol consumption and smoking habits, which may influence the risk of PTB. Our data and findings suggest that to avoid the risk of PTB, expectant mothers should consider childbirth before they reach the age of 35 years. This suggestion is consistent with that of reports that indicate that pregnancies between the ages of 20 and 35 years are likely to avert dysfunctions of the uterus, which often result in PTB among pregnant women older than 35.[18-20]
We examined parity as a risk factor of PTB. Unlike the findings from the study in Jordan,[7] we found an increase in parity score to be positively associated with the risk of PTB, which may be a result of the physical burden of multiple pregnancies. It may also be possible that mothers with high parity scores thought they could manage the pregnancy based on their previous experience of pregnancy, and so did not attend the minimum recommended number of ANC visits. It could also be that some mothers may have been busy caring for their other children or seeing to their business, and for that reason were unable to use antenatal services optimally. Our results suggest that attending the minimum number of antenatal visits lowers the risk of PTB and associated admission to the NICU.
Our study also investigated whether exposure to stress from unwanted pregnancies, economic hardship, family pressure or lack of spousal support increases or reduces the risk of PTB, with a positive relationship between maternal stress and the risk of PTB being expected. Unlike the findings by Dunkel Schnetter and Tanner,[20] our results suggest that the risk of PTB increases with the severity of maternal stress during pregnancy. Although maternal stress can also be associated with term neonates admitted to the NICU with complications, we contend that women whose preterm neonates are admitted to the NICU may generally have had higher levels of stress exposure. However, we have no a priori reason to believe that prior stress exposure would differ by reason for admission and our study cannot prove an association between stress exposure and PTB more generally, except to note that because PTBs account for the majority of admissions of neonates into the NICU, reducing maternal stress could also reduce the number of neonates admitted to the NICU.
Study strengths and limitations
In this study, we were able to deconstruct the degree and relative effect of maternal age, parity and stress in the fit of a logistic regression model. Our approach thus differs from existing studies that do not report model fit to establish the extent of the stochastic error term. As such, the study presents unique findings on maternal risk factors of PTB in Ghana and subsequent admission to the NICU. It adds to the literature on alternative measures of maternal stress as a risk factor of PTB and shows that both maternal stress and parity increase the risk of PTB. Unlike other related studies, we evaluated the extent of the fit of our model fit for both adjusted and unadjusted predictors of PTB. The lack of secondary clinical data on other potential risk factors, such as maternal diabetes, smoking or hypertension, may have contributed to the model fit of only 45%. Reports of exposure to stress during pregnancy were obtained retrospectively and, combined with being faced with their infants' admission to the NICU, which in itself is stressful, mothers may have been subject to recall bias. However, we believe this bias to be non-differential as it would apply to all mothers interviewed. Although a nationwide study at referral hospitals would be desirable to generalise the finding, it was not possible because the data reported here were leveraged from another, broader study on the cost of neonatal sepsis.
Conclusion
Despite many factors other than what we studied also contributing to the high risk of preterm deliveries in Ghana, and developing countries more broadly, our predictors explain a significant 45% of the chances of neonates admitted to the NICU at KBTH being preterm. From this, we conclude that the most appropriate intervention to reduce the high risk of PTB is for expectant mothers to attend at least four ANC visits so that any anomaly that could result in PTB can be identified and treated in time. In addition, our findings suggest women should consider childbirth before they reach the age of 35 years to avoid PTB. However, we encourage future studies of this kind to use population-based data to allow more generalisable results.
Declaration. None.
Acknowledgements. We acknowledge the support of our data collection team, NICU staff and especially the matron in charge, who provided an office space for conducting interviews.
Author contributions. EO conceptualised the study and prepared the initial manuscript. APF and KL supervised data collection and reviewed the manuscript. UE contributed to the discussion and interpretation of findings. All authors approved the final manuscript submitted for publication.
Funding. Financial support for data collection was received from the Danish Ministry of Foreign Affairs (DANIDA).
Conflicts of interest. None.
References
1. Obeidat HM, Bond EA, Callister LC. The parental experience of having an infant in the newborn intensive care unit. J Perinat Educ 2009;18(3):23-29. https://doi.org/10.1624/105812409X461199 [ Links ]
2. Callery P. Mothers of infants in neonatal nurseries had challenges in establishing feelings of being a good mother. Evid Based Nurs 2002;5(3):91-92. https://doi.org/10.1136/ebn.5.3.91 [ Links ]
3. Jackson K, Ternestedt B-M, Schollin J. From alienation to familiarity: Experience of mothers and fathers of preterm infants. J Adv Nurs 2003;43(2):120-129. https://doi.org/10.1046/j.1365-2648.2003.02686.x [ Links ]
4. World Health Organization. Recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet Gynecol Scand 1977;56:247-253. [ Links ]
5. Blencowe H, Cousens S, Chou D, et al. Born too soon: The global epidemiology of 15 million preterm births. Reprod Health 2013;10(Suppl 1):S2. https://doi.org/10.1186/1742-4755-10-S1-S2 [ Links ]
6. Abdel-Razeq NM, Khader YS, Batieha AM. The incidence, risk factors, and mortality of preterm neonates: A prospective study from Jordan (2012-2013). Turk J Obstet Gynecol 2017;14:28-36. https://doi.org/10.4274/tjod.62582 [ Links ]
7. Hamilton BE, Martin JA, Osterman MJ. Births: Preliminary data for 2015. Natl Vital Stat Rep 2016;65:1-15. [ Links ]
8. Wagura P, Wasunna A, Laving A, Wamalwa D, Nganga P. Prevalence and factors associated with preterm birth at Kenyatta National Hospital. BMC Pregnancy Childbirth 2018;18:107. https://doi.org/10.1186/s12884-018-1740-2 [ Links ]
9. Purisch SE, Gyamfi-Bannerman C. Epidemiology of preterm birth. Semin Perinatol 2017;41(7):387-391. https://doi.org/10.1053/j.semperi.2017.07.009 [ Links ]
10. Donoghue D, Lincoln D, Morgan G, Beard J. Influences on the degree of preterm birth in New South Wales. Aust N Z J Public Health 2013;37(6): 562-567. https://doi.org/10.1111/1753-6405.12132 [ Links ]
11. Tedesco RP, Passini R Jr, Cecatti JG, Camargo RS, Pacagnella RC, Sousa MH. Estimation of preterm birth rate, associated factors and maternal morbidity from a demographic and health survey in Brazil. Matern Child Health J 2013;17:1638-1647. https://doi.org/10.1007/s10995-012-1177-6 [ Links ]
12. Phaloprakarn C, Manusirivithaya S, Boonyarittipong P. Risk score comprising maternal and obstetric factors to identify late preterm infants at risk for neonatal intensive care unit admission. J Obstet Gynaecol Res 2015;41(5):680-688. https://doi.org/10.1111/jog.12610 [ Links ]
13. Mohammad K, Abu Dalou A, Kassab M, Gamble J, Creedy DK. Prevalence and factors associated with the occurrence of preterm birth in Irbid governorate of Jordan: A retrospective study. Int J Nurs Pract 2015;21(5):505-510. https://doi.org/10.1111/ijn.12335 [ Links ]
14. Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet 2008;371(9606):75-84. https://doi.org/10.1016/S0140-6736(08)60074-4 [ Links ]
15. Muglia LJ, Katz M. The enigma of spontaneous preterm birth. N Engl J Med 2010;362:529-535. https://doi.org/10.1056/NEJMra0904308 [ Links ]
16. Berkowitz GS, Blackmore-Prince C, Lapinski RH, Savitz DA. Risk factors for preterm birth subtypes. Epidemiology 1998;9(3):279-285. https://doi.org/10.1097/00001648-199805000-00011 [ Links ]
17. Delnord M, Blondel B, Prunet C, Zeitlin J. Are risk factors for preterm and early-term live singleton birth the same? A population-based study in France. BMJ Open 2018;8(1):e018745. https://doi.org/10.1136/bmjopen-2017-018745 [ Links ]
18. World Health Organization. WHO antenatal care randomised trial: Manual for the implementation of the new model. Geneva: WHO, 2002:37. [ Links ]
19. Dickson KS, Darteh EK, Kumi-Kyereme A. Providers of antenatal care services in Ghana: Evidence from Ghana demographic and health surveys 1988-2014. BMC Health Serv Res 2017;17:1-9. https://doi.org/10.1186/s12913-017-2145-z [ Links ]
20. Dunkel Schnetter C, Tanner L. Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Curr Opin Psychiatry 2012;25(2)141-148. https://doi.org/10.1097/yco.0b013e3283503680 [ Links ]
21. Fenny AP, Otieku E, Labi A-K, Asante FA, Enemark U. Costs and extra length of stay because of neonatal bloodstream infection at a teaching hospital in Ghana. Pharmacoecon Open 2021;5:111-120. https://doi.org/10.1007/s41669-020-00230-x [ Links ]
22. Nkyekyer K, Enweronu-Laryea C, Boafor T. Singleton preterm births in Korle Bu Teaching Hospital, Accra, Ghana - origins and outcomes. Ghana Med J 2006;40:93-98. [ Links ]
23. McDonald SD, Han Z, Mulla S, Beyene J, Knowledge Synthesis Group. Overweight and obesity in mothers and risk of preterm birth and low birthweight infants: Systematic review and meta-analyses. BMJ 2010;341(7765):c3428. https://doi.org/10.1136/bmj.c3428 [ Links ]
 Correspondence:
Correspondence:
E Otieku
otieku@yahoo.com
Accepted 10 December 2020.


{kind=link}
{kind=link}