










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.15 n.3 Pretoria Sep. 2021
http://dx.doi.org/10.7196/SAJCH.2021.v15.i3.1757
RESEARCH
Short-term outcomes of very low-birthweight infants with intraventricular haemorrhage who received respiratory support in a middle-income country neonatal unit
D GoolabI; L TookeII; S le RouxIII; Y JoolayIII
IDCH (SA); Department of Neonatology, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIMMed (Paeds), Cert Neonatol (SA); Department of Neonatology, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIIMPH; Division of Epidemiology and Biostatistics, School of Public Health and Family Medicine, University of Cape Town, South Africa
IVMPhil (Neonatol), Cert Neonatol (SA) Department of Neonatology, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Prematurity is a major risk factor for intraventricular haemorrhage (IVH). Premature infants often require respiratory support. There is little information on neonates with IVH on respiratory support in low- and middle-income countries.
OBJECTIVE. To describe the characteristics and short-term outcomes of very-low-birthweight (VLBW) infants with IVH receiving respiratory support in a tertiary neonatal unit with resource limitations.
METHODS. This was a matched retrospective observational study. The population included VLBW infants with IVH, who received positive pressure respiratory support between January 2014 and December 2016. Severe IVH was compared with mild IVH.
RESULTS. One hundred and fifty infants were included in the study; 56 (37%) received continuous positive airway pressure (CPAP) only and 94 (63%) mechanical ventilation. Severe IVH was associated with surfactant therapy across both ventilation groups (p=0.03). Infants with severe IVH had prolonged oxygen requirements at 28 days (79% v. 38%; p=0.01) (odds ratio (OR) 6.11; 95% confidence interval (CI) 1.19 - 31.34; p=0.03) v. those with mild IVH. Severe IVH and the presence of coagulopathy were the strongest predictors of death in both ventilation groups (p <0.0001). Pulmonary haemorrhage was the most common cause of death in severe IVH and blood culture-confirmed sepsis in mild IVH. Periventricular leukomalacia (PVL) was associated with severe IVH in invasive ventilation (OR 6.67; 95% CI 1.11 - 40.17).
CONCLUSION. VLBW infants with severe IVH who are mechanically ventilated or with coagulopathy have a high mortality, with pulmonary haemorrhage being the prominent cause of death. These prognostic factors may assist in end-of-life care in resource-limited settings.
Intraventricular haemorrhage (IVH) is a frequent complication in preterm infants.[12] Severe IVH (characterised as grades 3 and 4) is associated with a higher rate of mortality, significant morbidities and long-term neurological impairment.[3] The incidence of IVH increases with decreasing gestational age, with prematurity being the most important risk factor, as evidenced by multiple studies.[1, 2, 4]
Respiratory support as a risk factor for IVH has shown conflicting reports. Randomised control trials have demonstrated that the use of prophylactic continuous positive airway pressure (CPAP) in preterm infants at birth does not show a significant difference in the incidence of IVH compared with low-flow nasal cannula/ oxyhoodP-[6] or mechanical ventilation at birth[7-9] However, observational research suggests that infants requiring mechanical ventilation are associated with a significant increase in IVH, with early and prolonged ventilation being important determinants for severe IVH.[10]
Respiratory support is frequently required in preterm infants. Published literature on the subject is mainly from resource-rich settings, limiting the applicability in middle-income and developing countries where a high burden of preterm births exists.[11] These settings would benefit from studies in similar resource contexts, providing the necessary perspective to develop reduction strategies, with appropriate application of distributive justice.
Objectives
To describe the occurrence of IVH and short-term outcomes in very-low-birthweight (VLBW) infants receiving positive pressure respiratory support in a single tertiary centre in a middle-income African country.
Methods
This was a matched retrospective observational study. The source population included all VLBW neonates with IVH, requiring either CPAP (non-invasive) or mechanical ventilation (invasive) admitted to Groote Schuur Hospital (GSH) between January 2014 and December 2016. Neonates with major congenital abnormalities or other severe comorbidities, such as congenital syphilis or congenital cytomegalovirus infection, were excluded from the study to allow more accurate analysis. From the eligible group, all those with a diagnosis of severe IVH (Grade 3 and 4) were chosen as cases. The remaining infants, all with mild IVH (grade 1 and 2), were allocated as comparative controls. Controls were individually matched to each case (1:1) within the following strata: (i) birthweight category (<750 g; >750 g up to 1 000 g; >1 000 g to 1 250 g; and >1 250 g; (ii) type of respiratory support (non-invasive v. invasive); and (iii) year of birth. The matching process therefore yielded two groups for comparison: (i) all infants with severe IVH and (ii) matched infants with mild IVH.
Patients were described according to maternal, birth and admission characteristics. Definitions of specific characteristics include cardiopulmonary resuscitation (CPR), defined as chest compressions for any duration, adrenaline not being part of the definition; sepsis, defined as a positive blood culture; coagulopathy, defined as international normalised ratio (INR) >1.2 or platelets <100 and necrotising enterocolitis (NEC) defined as NEC at all stages according to Bell's criteria.
Short-term outcomes analysed included mortality, length of hospital stay, periventricular leukomalacia (PVL), post-haemorrhagic hydrocephalus (PHH), retinopathy of prematurity (ROP) and chronic lung disease (CLD). PHH was defined by increasing ventricle size according to serial cranial ultrasounds in infants with severe IVH. CLD was assessed as oxygen requirements at 28 days of age and 36 weeks' corrected gestation. Disability was defined as death and/or at least one of PVL, PHH, ROP and CLD.
Data collection
Since mid-2013, details of all VLBW newborn infants admitted to GSH have been retrospectively entered into the Vermont Oxford Network (VON) database. The database consists of extensive clinical details from birth until discharge/death and was utilised as a source for population characteristics and outcomes. Patients' folders were extracted for additional information not available from the database.
Clinical care in the neonatal unit
GSH is a tertiary level hospital with ~500 VLBW infants admitted to the 75-bed neonatal unit per annum. The neonatal intensive care unit (NICU) consists of 20 neonatal beds which can be utilised for either mechanical ventilation (maximum of 8) or nasal CPAP. A further 20 high-care beds can provide oxygen therapy via low- or high-flow nasal cannulae.
Clinical decision making for VLBW infants was guided by evidence-based standardised protocols, in keeping with the resource-limited setting of this study.
Mechanical ventilation was considered only for infants with a birthweight of at least 800 g and a gestational age of 27 completed weeks. However, the senior neonatologist on duty could decide on mechanical ventilation of a patient if there was a significant discrepancy with birthweight and gestational age. Those with severe IVH were ineligible for mechanical ventilation. Surfactant use was limited to those on CPAP or mechanical ventilation with persistent fraction of inspired oxygen (FiO2) requirements above 30% or failing to wean. Cranial sonography was routinely conducted on all VLBW infants before day 3 of life, again at age 3 - 5 weeks, and at discharge or corrected term gestation (depending on which came first). IVH was graded according to Volpe's classification. Scan frequency would be increased according to clinical condition. Cranial ultrasounds are done by medical staff trained in this skill and reviewed by certified neonatologists.
Analytical approach
Descriptive statistics were used to summarise all relevant characteristics, using standard comparative methods. Data were analysed for the full cohort and within strata of ventilation strategy, using Stata 14.0 (Statacorp., USA).
Potential risk factors for the outcomes of severe v. mild IVH were evaluated, using a case-control approach. Data were analysed using crude and adjusted conditional logistic regression, controlling for matched pairs.
Outcomes following IVH were evaluated using a matched cohort approach with severe IVH being the main exposure. Survival analysis was used to assess risk of mortality, overall and within strata of (i) ventilation strategy and (ii) eligibility for treatment escalation. Exposure time (expressed as child-years) was measured from birth to death/discharge from the neonatal unit. Between-group comparisons were made using Kaplan-Meier curves (log-rank test), incidence rate ratios and Cox proportional hazards regression (robust standard errors to account for clustering; proportional hazards assumption checked with Schoenfeld residuals). Morbidity outcomes were compared between severe and mild IVH using logistic regression (robust standard errors).
We estimated that a sample size of 150 (1:1) would have 80% power to detect a 1.6 times or greater mortality hazard ratio among severe v. mild IVH (α=0.05, two-sided).
Ethical considerations
Data collection was done by the primary author and all records were kept anonymous. Patients' records on the VON database are structured on number allocations, ensuring confidentiality. Furthermore, the database is password protected and only accessible to designated users involved in data capturing.
The study was approved by the Human Research Ethics Committee, Faculty of Health Sciences, University of Cape Town (HREC ref. no. 725/2017).
Results
Study demographics
The study population comprised 150 infants (75:75, severe v. mild IVH), of whom 56 (37%) received non-invasive and 94 (63%), invasive ventilation. Inborn patients comprised 112 (75%) of the 150 patients.
Maternal and infant characteristics
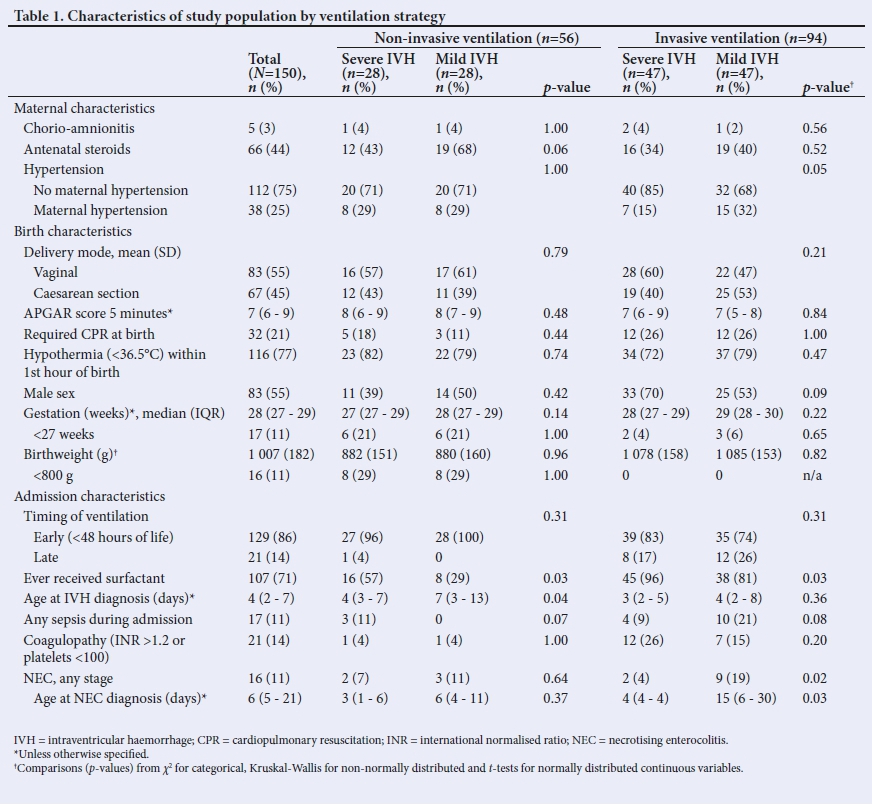
The median/interquartile range (IQR) gestation at birth was 28 (27 - 29) weeks. In the non-invasive ventilation group, 28 (50%) of the infants were not considered eligible for mechanical ventilation and inotropes based on their birthweight and gestational age (Table 1). This was re-considered periodically as the infant became older. Infants who received non-invasive ventilation had lower mean birthweight (880 g v. 1 081 g; p<0.0001) and lower median gestation at birth (27.9 v. 28.6 weeks; p=0.001) compared with infants who received invasive ventilation.
A greater proportion of infants with severe (compared with mild) IVH received surfactant therapy during their admission (81% v. 61%; p=0.007). This result extended across both ventilation groups (p=0.03). From those with severe IVH and surfactant administration, 22/61 (36%) received antenatal steroids compared with 18/46 (39%) with mild IVH. Other study population characteristics are shown by ventilation strategy, in Table 1.
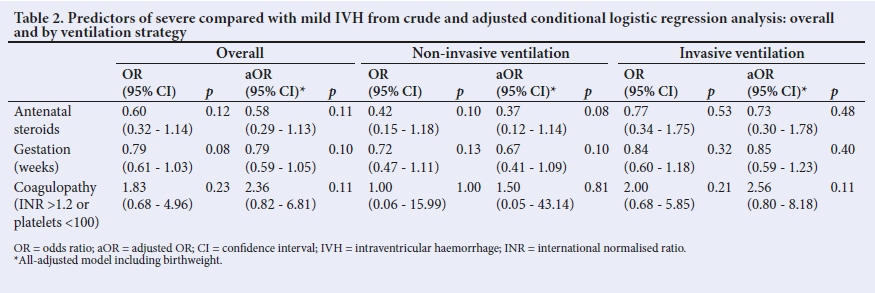
Although precision was limited, we identified some factors predictive of severe IVH (Table 2). These included gestation at birth (per week increase, odds ratio (OR) 0.79 (95% CI 0.61 - 1.03; p=0.08), antenatal steroid use (v. none, OR 0.60 (95% CI 0.32 -1.14; p=0.12) and, after adjusting for the above, coagulopathy (v. none, adjusted OR (aOR) 2.36 (95% CI 0.82 - 6.81; p=0.11). The strength of these associations differed within strata of ventilation strategy. After adjustment, the strongest predictor for severe IVH was no antenatal steroid use among non-invasively ventilated patients; and coagulopathy among invasively ventilated patients. Despite the wide confidence intervals (reflecting lack of precision due to small sample size), the point estimates reflect strong associations which are of clinical significance.
Outcomes
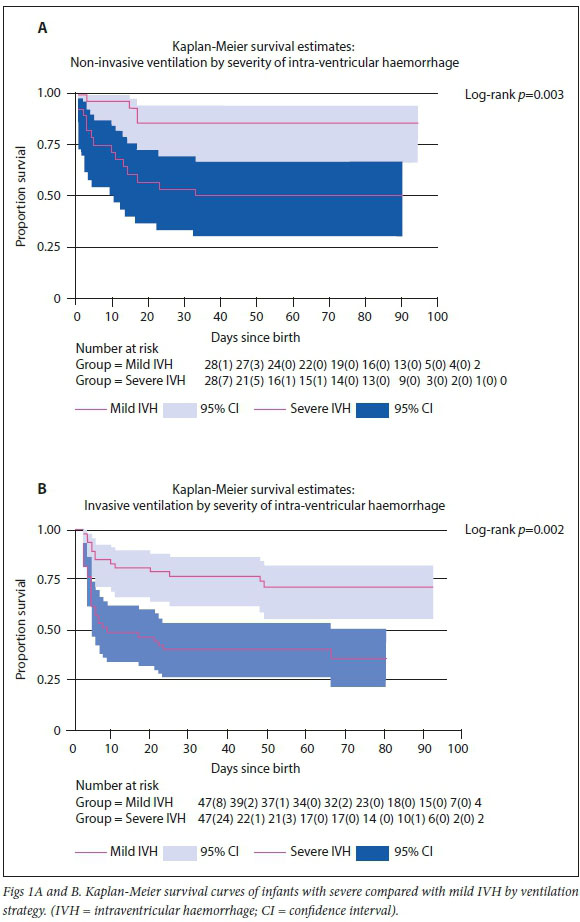
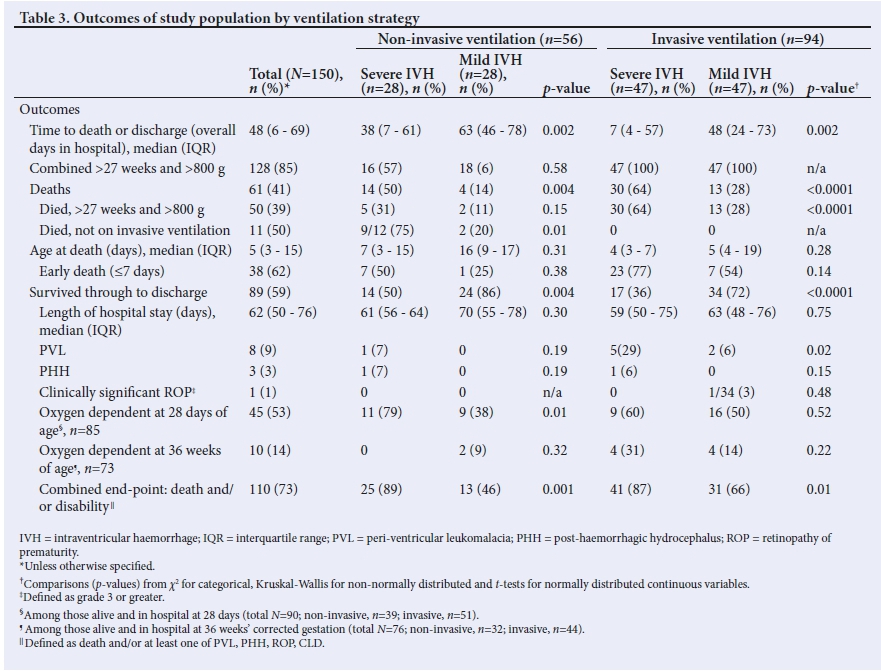
Overall, 61 (41%) of 150 infants died (Table 3). Severe IVH was associated with substantially increased mortality risk. Fig. 1 demonstrates this association within the non-invasive ventilation (incidence rate ratio (IRR) 5.88; 95% CI 1.85 - 24.53) and invasive ventilation (IRR 3.96; 95% CI 2.00 - 8.26) strata. These results were further reflected in crude and adjusted Cox regression models (Table 3). After adjusting for antenatal steroid use, infant sex, birthweight, coagulopathy and ventilation type, the relative hazard for death comparing severe to mild IVH was 4.32 (95% CI 1.99 - 9.37; p<0.0001) in non-invasive ventilation and 2.82 (95% CI 1.47 - 5.40; p=0.002) in invasive ventilation.
In the sub-group of infants not for mechanical ventilation (Table 3), n=11/22 (50%) died: n=9/12 (75%) infants with severe IVH compared with n=2/10 (20%) infants with mild IVH. Supplementary Table 1 (http://www.sajch.org.za/public/files/1764.pdf) demonstrates the increased mortality rate per child-years in severe IVH compared with mild IVH, with an IRR of 9.74 (95% CI 2.02 - 92.64). Mortality rates and IRR for severe v. mild IVH for the sub-group of infants who were eligible for mechanical ventilation are shown in Supplementary Table 2 (http://www.sajch.org.za/public/files/1764.pdf), with similar IRRs.
The age at death was earlier in severe IVH compared with mild IVH across both ventilation groups. Sixty-eight percent (n=30/44) of deaths in the severe IVH group occurred within the first seven days. The timing of death between severe and mild IVH was not significant (Table 3).
Although severity of IVH and presence of coagulopathy during admission were consistently the strongest predictors of death (Table 4), the effects of birthweight, resuscitation at birth and sepsis varied. The protective effects of patients with higher birthweight were most evident in the non-invasive ventilation group (aHR 0.64; 95% CI 0.45 - 0.9; p=0.01). CPR was associated with a reduced hazards ratio among those who received invasive ventilation (aHR 0.44; 95% CI 0.20 - 0.98; p=0.04). Sepsis was a strong risk factor for mortality in the non-invasive ventilation group (HR 4.55; 95% CI 2.25 - 9.23; p<0.0001).
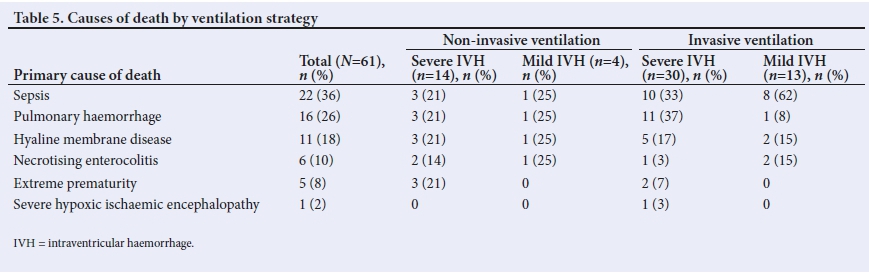
Causes of death are presented in Table 5. The most common cause of mortality was blood culture-confirmed sepsis (n=22/61; 36%), which was followed by pulmonary haemorrhage (n=16/61; 26%), hyaline membrane disease (n=11/61; 18%), NEC (n=6/61; 10%), extreme prematurity (<1000 g) (n=5/61; 8%) and severe hypoxic ischaemic encephalopathy (n=1/61; 2%). Pulmonary haemorrhage was the most common cause of death in those with severe IVH (n=14/44; 32%) and blood culture-confirmed sepsis in those with mild IVH (n=9/17; 53%).
NEC developed in 16/150 (11%) patients. Patients with severe IVH and NEC were more likely to die early (<7 days), which differed in comparison with those with mild IVH who were less likely to die from NEC.
Morbidity data are presented in Table 3. Median length of hospital stay was 62 (IQR 50 - 76) days among survivors, with no significant difference by IVH severity; this differed compared with time to death/ discharge which was considerably earlier in infants with severe IVH when grouped according to ventilation group, reflecting the higher mortality rate and shorter time to death among those with severe compared with mild IVH.
PVL was associated with severe IVH in invasive ventilation (OR 6.67; 95% CI 1.11 - 40.17) in infants who survived through to discharge. PHH was not specifically associated with severe or mild IVH. Data for ROP were only consistently available for 2016, with one case of clinically significant ROP recorded (non-invasive ventilated infant with mild IVH). Among survivors, a higher proportion of infants with severe IVH had prolonged oxygen requirements at 28 days (79% v. 38%, £=0.01) (OR 6.11; 95% CI 1.19 - 31.34,/>=0.03) than those with mild IVH.
Discussion
Preterm birth represents a significant burden in low- and middle-income countries, with extreme prematurity being the leading cause of death.[1] A central hospital in Johannesburg, with similar practices to our neonatal unit, analysed causes of mortality of VLBW infants. The use of surfactant and CPAP improved survival, but extreme prematurity was still the primary cause of death in VLBW infants.[12]
To maintain distributive justice in our setting, severely premature infants do not receive invasive ventilation based on a standardised protocol. Consequently, infants receiving invasive ventilation for respiratory failure, cardiac failure, sepsis or pulmonary haemorrhage do not also have extreme prematurity. This protocol explains the association between a lower mean birthweight and gestation with non-invasive ventilation in our study. Also contributing to mortality in the non-invasive severe IVH group would be the ineligibility of these infants to qualify for mechanical ventilation. This also explains why prematurity is an uncommon cause of death in the invasive ventilation group.
Resource limitations which led to fewer extreme preterm infants in the invasive ventilation group may have influenced certain predictors of mortality. CPR at birth in preterm infants is associated with a higher mortality.[13] This detrimental effect of CPR was not demonstrated when assessing predictors of mortality. Prolonged resuscitation attempts can lead to decisions restricting invasive ventilation in these patients.
Prophylactic surfactant in comparison with selective surfactant, in patients with routine CPAP, has been researched.[7, 9, 14] The SUPPORT study showed a decrease in severe IVH in patients who had received prophylactic surfactant but this was not significant.[9] Dunn et al[7] showed an increase in severe IVH in the same group, but also not significant. A 2012 Cochrane review demonstrated an overall marginal decrease in IVH on patients receiving prophylactic surfactant, with or without routine CPAP.[14]
Our results reflect the neonatal policies at GSH, which does not practice prophylactic surfactant but rather administers it as rescue therapy. Therefore, unstable patients were more likely to receive surfactant. Given the instability of these patients, they were more likely to develop or already have severe IVH and other comorbidities, which could explain the high number of severe IVH and high mortality rates in this group. The timing of surfactant was not recorded in relation to the timing of the bleed. Further studies on surfactant rescue therapy would be needed to determine its effects in a resource-constrained setting.
Expectedly, overall mortality showed a significant association with severe IVH with no difference across ventilation groups.[15] Aly et al.[10] found mechanical ventilation to be an important predictor of severe IVH. Mechanical ventilation has significant haemodynamic effects on the infant, which could affect cerebral blood flow[2] Prolonged positive pressure ventilation also increases blood-brain barrier permeability and contributes to the development of IVH[2] Our study demonstrated that severe IVH was an important predictor of mortality, with higher mortality rates per child-years compared with mild IVH. Accuracy was weakened owing to the wide confidence interval in the group not eligible for ventilation. When analysed in the subgroup of infants eligible for escalation, we found invasive ventilation with severe IVH to also predict mortality with a higher, although similar, IRR compared with non-invasive ventilation.
In patients receiving invasive ventilation with severe IVH, pulmonary haemorrhage was the most common cause of death, with most having coagulation abnormalities. Coagulopathy were shown to be a poor prognostic factor for mortality overall and within ventilation categories; this highlights a vulnerable group in our neonatal unit that may benefit from closer monitoring in an ICU setting. According to the evidence, prophylactic fresh frozen plasma (FFP) is not recommended over therapeutic FFP. Tran et al[16] was able to identify preterm infants at risk for coagulopathy and severe IVH but FFPs were not beneficial in preventing IVH or decreasing mortality. Prophylactic use of FFPs based on a risk stratification profile in preterm infants was not recommended in this retrospective study done at GSH[17]
There was a higher incidence of NEC in mild IVH with the majority surviving, while those with severe IVH had a lower incidence of NEC but higher mortality. This finding can be explained by the shorter lifespan and increased mortality rates in infants with severe IVH. NEC was diagnosed close to the date of death; however, our study did not find it to be an independent predictor of mortality. In other studies, NEC has not been identified as an independent risk factor for IVH.P]
Premature infants who survived through to discharge had similar lengths of stay despite receiving invasive or non-invasive ventilation. Oxygen requirements at 28 days of life was more common in infants who received non-invasive ventilation and had severe IVH. This is probably because of the lower birthweight and gestation of infants in this group and their additional burden of comorbidities. However, there was no difference in bronchopulmonary dysplasia (assessed at 36 weeks' corrected gestation) in either ventilation group between infants with severe or mild IVH.
PHH and PVL are known complications of IVH[18] This could not be demonstrated in our study as the low numbers did not allow accurate analysis. Incomplete ROP records prevented analysis of these data.
Study limitations
The study was limited by its retrospective design, which may increase the risk of bias. The use of matched controls resulted in exclusion of some data; the smaller sample size resulted in imprecision for some estimates. The design also did not include matching the cases to inborn status. Despite this limitation, strong relationships remained robustly evident, and our findings have substantial clinical implications. Extremely premature infants did not qualify for mechanical ventilation based on GSH policies, a reflection of our resource-limited setting. Therefore, the combined effects of mechanical ventilation and severe IVH could not be determined for these infants. Limited data on ROP precluded analysis for this critical outcome. Finally, the study was performed in a single tertiary neonatal population, which may limit generalisability. However, a major strength of the study is its real-world setting, which provides greater generalisability than data from clinical trials.
Conclusion
Our study demonstrated that mechanical ventilation and severe IVH were important predictors of mortality. The most common cause of death in severe IVH was pulmonary haemorrhage with an associated coagulopathy in this group. This finding provides a useful clinical adjunct when determining prognostication and counselling regarding these patients.
Infants receiving surfactant had a high rate of severe IVH. The high incidence was attributed to their instability qualifying them for surfactant therapy. This group would benefit from closer monitoring. Future studies can focus on the relationship between severe IVH and respiratory support, following the administration of surfactant.
Understanding outcomes of preterm infants in low- and middle-income settings may be improved by the development and maintenance of quality improvement databases in order to facilitate patient management protocols and research in this context.
Declaration. None.
Acknowledgements. None.
Author contributions. YJ conceptualised the study and design, supervised all processes of the study, provided support with data interpretation and assisted in revision of the article. DG did data collection, interpretation and drafting of the manuscript. LT managed the VON database, provided data, and assisted with supervision. SLR provided data analysis and interpretation. YJ, DG, LT and SLR reviewed and approved the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Ballabh P. Intraventricular hemorrhage in premature infants: Mechanism of disease. Pediatr Res 2010;67( 1):1-8. https://doi.org/10.1203/pdr.0b013e3181c1b176 [ Links ]
2. Ballabh P. Pathogenesis and prevention of intraventricular hemorrhage. Clin Perinatal 2014;41(1):47-67. https://doi.org/10.1016/j.clp.2013.09.007 [ Links ]
3. Bolisetty S, Dhawan A, Abdel-Latif M, et al. Intraventricular hemorrhage and neurodevelopmental outcomes in extreme preterm infants. Pediatrics 2014;133(1):55-62. https://doi.org/10.1542/peds.2013-0372 [ Links ]
4. Volpe JJ. Intracranial hemorrhage: Neurology of the newborn. 5 th ed. Philadelphia: WB Saunders, 2008:481-588. [ Links ]
5. Tapia JL, Urzua S, Bancalari A, et al. Randomised trial of early bubble continuous positive airway pressure for very low birth weight infants. J Pediatr 2012;161(1):75-80. https://doi.org/10.1016/jjpeds.2011.12.054 [ Links ]
6. Sandri F, Ancora G, Lanzoni A et al. Prophylactic nasal continuous positive airways pressure in newborns of 28-31 weeks gestation: Multicentre randomised controlled clinical trial. Arch Dis Child Fetal Neonatal Ed 2004;89(5):F394-F398. https://doi.org/10.1136/adc.2003.037010 [ Links ]
7. Dunn MS, Kaempf J, de Klerk A, et al. Vermont Oxford Network DRM Study Group. Randomised trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011;128(5):e1069-e1076. https://doi.org/10.1542/peds.2010-3848 [ Links ]
8. Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med 2008;358(7):700-708. https://doi.org/10.1056/nejmoa072788 [ Links ]
9. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med 2010;362(21):1970-1979. https://doi.org/10.1056/nejmoa0911783 [ Links ]
10. Aly H, Hammad TA, Essers J, Wung JT. Is mechanical ventilation associated with intraventricular hemorrhage in preterm infants? Brain Dev 2012;34(3):201-205. https://doi.org/10.1016/j.braindev.2011.04.006 [ Links ]
11. Harrison MS, Goldenberg RL. Global burden of prematurity. Semin Fetal Neonatal Med 2016;21(2):74-79. https://doi.org/10.1016/j.siny.2015.12.007 [ Links ]
12. Ballot DE, Chirwa T, Ramdin T, et al. Comparison of morbidity and mortality of very low birth weight infants in a central hospital in Johannesburg between 2006/2007 and 2013. BMC Pediatrics 2015;15(1):20. https://doi.org/10.1186/s12887-015-0337-4 [ Links ]
13. Handley SC, Sun Y, Wyckoff MH, Lee HC. Outcomes of extremely preterm infants after delivery room cardiopulmonary resuscitation in a population-based cohort. J Perinatal 2015;35(5):379-383. https://doi.org/10.1038/jp.2014.222 [ Links ]
14. Rojas Reyes MX, Morley CJ, Soll R. Prophylactic versus selective use of surfactant in preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev 2012(3). https://doi.org/10.1002/14651858.cd000510 [ Links ]
15. Christian EA, Jin DL, Attenello F, et al. Trends in hospitalisation of preterm infants with intraventricular hemorrhage and hydrocephalus in the United States, 2000-2010. J Neurosurg Pediatr 2016;17(3):260-269. https://doi.org/10.3171/2015.7.peds15140 [ Links ]
16. Tran TT, Veldman A, Malhotra A. Does risk-based coagulation screening predict intraventricular haemorrhage in extreme premature infants? Blood Coagulation Fibrinolysis 2012;23(6):532-536. https://doi.org/10.1097/mbc.0b013e3283551145 [ Links ]
17. Raban MS, Harrison MC. Fresh frozen plasma use in a neonatal unit in South Aftica. J Trop Pediatr 2015;61(4):266-271. https://doi.org/10.1093/tropej/fciv027 [ Links ]
18. Bassan H. Intracranial hemorrhage in the preterm infant: Understanding it, preventing it. Clin Perinatal 20091;36(4):737-762. https://doi.org/10.1002/14651858.CD000510.pub2 [ Links ]
 Correspondence:
Correspondence:
Y Joolay
yaseen.joolay@uct.ac.za
Accepted 15 December 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}