










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.15 n.2 Pretoria Jun. 2021
http://dx.doi.org/10.7196/sajch.2021.v15.i2.1715
RESEARCH
Individual and community-level factors associated with symptoms of acute lower respiratory infections among children under 5 years of age in Eswatini
M S SimelaneI, II; K VermaakI
IPhD; School of Built Environment and Development Studies, University of KwaZulu-Natal, Durban, South Africa
IIPhD; Department of Statistics and Demography, Faculty of Social Sciences, University of Eswatini, Kwaluseni, Eswatini
ABSTRACT
BACKGROUND: Despite initiatives and efforts implemented over the years that would impact positively on child health, acute lower respiratory infections (ALRIs) remain a serious challenge for under-5s
OBJECTIVE: To investigate the individual- and community-level factors associated with child ALRIs in Eswatini
METHODS: Using the combined data for 2010 and 2014 Eswatini Multiple Indicator Cluster Surveys, data for 4 265 children under 5 years of age were analysed. Univariable, bivariable and multivariable multilevel logistic regression analyses were conducted
RESULTS: We found that the prevalence of ALRIs was 11.1% (95% confidence interval (CI) 10.0 - 12.4). Higher odds of ALRIs were observed among children who had reported diarrhoea in the same time period (adjusted odds ratio (aOR) 1.75; 95% CI 1.37 - 2.23) compared with those who did not report diarrhoea, and those born to women with no formal education (aOR 2.16; 95% CI 1.13 - 4.16) and those with primary education (aOR 2.60; 95% CI 1.34 - 5.04) compared with those born to women with tertiary education. Place of residence was a community-level variable associated with higher odds of ALRIs among children from urban areas (aOR 1.59; 95% CI 1.15 - 2.20) compared with rural residents. Those from Manzini (aOR 2.19; 95% CI 1.59 - 3.12), Shiselweni (aOR 1.73; 95% CI 1.23 - 2.44) and Lubombo (aOR 1.77; 95% CI 1.25 - 2.51) were more likely to be infected with ALRIs compared with those from the Hhohho region. In addition, higher odds of ALRIs were observed in children from communities with a low proportion of households with electricity (aOR 1.46; 95% CI 1.10 - 1.95) compared with those from communities with high access to electricity
CONCLUSIONS: We found that individual- and community-level factors were associated with child ALRIs across communities in Eswatini. Programmes and policies that aim to mitigate child morbidity due to ALRIs should integrate the individual and community factors
Acute lower respiratory infections (ALRIs) continue to be a public health challenge and persistently affect children under 5 years of age, primarily in developing countries.[1] ALRIs are due to bacterial, fungal, or viral infections of the respiratory tract, leading to breathing difficulties, fatigue, wheezing, pain on swallowing, fever, cough, nasal discharge and sputum production.[2] Coupled with diarrhoea and newborn sepsis, ALRIs remain the leading cause of morbidity and mortality among children under 5 years of age.[3] Despite initiatives and efforts implemented over the years to impact positively on child health, including the introduction of Sustainable Development Goals (SDGs) post 2015 to 2030,[4] ALRIs remain a serious challenge for under-5s. They have resulted in ~2.38 million deaths in 2016 across all ages, while among under-5s, they were the leading cause of death.[5,6] Substantial child morbidity and mortality are concentrated in sub-Saharan Africa (SSA) and South Asia.[5,7] In 2015, it was observed that in 15 developing countries over 50% of child deaths were due to ALRIs, with 9 situated in SSA.[8]
Studies conducted elsewhere reported associations between the age of the child, sex of the child, breastfeeding status, low birthweight, indoor and outdoor air pollution, nutritional status, overcrowding, household wealth index and type of cooking material and ALRIs.[9-11] The socioeconomic inequality across communities and regions has long been recognised in the literature as contributing to the unequal risk of exposure to ALRIs.[12,13] Consideration of individual-level data independent of the population context may be misleading.[12] However, very few studies have incorporated a design-based methodology by applying multilevel approaches that control for the clustering of ALRIs across communities, especially in Eswatini.[9,14] The empirical gap in the literature needs to be addressed with more focus on most affected countries such as Eswatini.
The magnitude of ALRIs is still very high in Eswatini, 8.7% in 2010, and 9.8% in 2014.[15,16] Investigation of risk factors is fundamental to realise the SDGs agenda to ensure wellbeing for all. Therefore, the study aimed to investigate the effects of the individual- and community-level factors on ALRIs, through multilevel logistic regression. Children are born and raised in households that are nested within the community;[12] therefore, understanding the complex nature of the factors and their effects on child ALRIs in Eswatini is critical for the management and prevention of ALRIs.
Methods
This study was a secondary analysis of the combined data from the 2010 and 2014 Eswatini Multiple Indicator Cluster Surveys (EMICSs). The Multiple Indicator Cluster Survey (MICS) is an international initiative by the United Nations Children's Fund (UNICEF) to assist countries in collecting and analysing data for monitoring the situation of children, women, and men in developing countries. It is a cross-sectional household survey conducted every 3 - 5 years to enable countries to capture rapid changes in key indicators, such as those related to health, education and development. In the EMICS, data were collected using standardised survey tools through face-to-face interviews among nationally representative samples of households.[15,16]
Sampling design and study samples
The EMICS was representative and collected information on households, men, women, and children. The sampling frame of the enumeration was based on the 2007 Eswatini Population and Housing Census.[17] A two-staged sampling technique and a systematic sampling technique were applied. First, enumeration areas (EAs), also known as the primary sampling units (PSUs), were selected. Second, households were selected, stratified by rural and urban residence and the four regions of the country, which are Manzini, Hhohho, Shiselweni, and Lubombo. To collect data for under-5s, a standardised questionnaire was used to obtain information for each child in the selected households. The mother or caregiver was the respondent for the child questionnaire.
For the 2010 EMICS, 5 475 households were selected from 345 EAs. Among the sampled households, a total of4 834 were successfully interviewed, which included 4 956 women aged 15 - 49 years and 4 646 men aged 15 - 59 years. The overall household response rate was 95%. In the 2010 sample, during the interviews questionnaires were completed regarding 2 647 children aged under 5 years.
In the 2014 EMICS, a total of 347 EAs and 5 211 households were selected for the survey. Within each region, urban and rural areas were identified as the main sampling strata. Within each EA, a sample of 15 households was selected systematically using probability proportional to size (PPS) and a specified number of census EAs were chosen systematically using PPS.[15] A total of 4 762 women (aged 15 - 49 years) and 1 459 men (aged 15 - 59 years) were successfully interviewed. A detailed description of the sampling design is available in the 2014 MICS report.[15]
In the 2014 EMICS, during the interviews questionnaires were completed regarding 2 693 children aged under 5 years. However, for the combined 2010 and 2014 surveys, only 4 265 under-5s with complete data on ALRI symptoms were included in the analysis.
Study variables
Outcome variables. The study outcome variable was symptoms of ALRIs 2 weeks before the MICS. In this analysis, we considered ALRIs symptoms if the mother/caregiver reported that the child had a cough with rapid breathing or difficulty breathing, and the symptoms were due to a problem in the chest or both a problem in the chest and a blocked nose.[14-16,18] The variable was coded as binary: (1) for those with symptoms, (0) for those without symptoms.
Explanatory variables. The explanatory variables included child and maternal factors, household and community factors.[11,19,20] Individual-level variables were child age in months, sex, child diarrhoea status, child stunting status, maternal education, maternal age, parity, marital status, source of cooking fuel, household electricity, type of toilet, floor material, number of people sleeping per room, number of children under 5 years, household wealth index. The household wealth index had been calculated in the EMICS dataset and was categorised into five quartiles, namely the poorest, poor, middle, rich and richest.[15,16] Wealth indices use information about household durable assets, such as housing materials, toilet or latrine access, phone ownership, or agricultural land and livestock, which are regularly collected in most household surveys to create an index of household wealth.[21]- The principal component analysis (PCA) was used to develop the household wealth index.[21] Community-level variables were area of residence, region of residence, community poverty (proportion of households in the communities classified in the poorest and poor wealth quantiles), community maternal education (proportion of mothers with at least secondary level education in the community), electricity use in the community (proportion of households with electricity in the community), and improved cooking fuel in the community (proportion of households with improved fuel for cooking in the community). Based on the literature, the individual-level variables were aggregated by cluster and categorised as low (1), medium (2) and high (3),[9,22] or low (1) and high (2).[23]
Statistical analysis
Descriptive statistics were performed to assess the distribution of the sample and the magnitude of child ALRIs. A bivariable analysis through the x2 test was performed to test for crude association between each explanatory factor and ALRIs. The variance inflation factor (VIF) was used to test for strongly correlated explanatory factors, and no factors were strongly correlated to each other (see Appendix 1, supplementary Table 2, online only). Owing to the hierarchical nature of the dataset, a multilevel model that controls for clustering of the ALRIs across communities was used. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were used to establish the fixed effects of the models. Random effects, important to establish the random variation of ALRIs across communities, were denoted by the intraclass correlation (ICC) and the proportion of change in the variance (PCV). Four models were fitted to analyse the data. Model 1: An empty model to produce a random variation of the intercept (random effects) and the ICC. Model 2 included only individual-level variables. Model 3 included only community-level factors. Model 4 included individual- and community-level variables in one model. The entire analysis took into account survey weights and was done in Stata 15 (Stata Corp., USA).
Ethical considerations
The protocol was approved by the University of KwaZulu-Natal's Humanities and Social Science Research Ethics Committee and the Eswatini National Health and Human Research Review Board.
Results
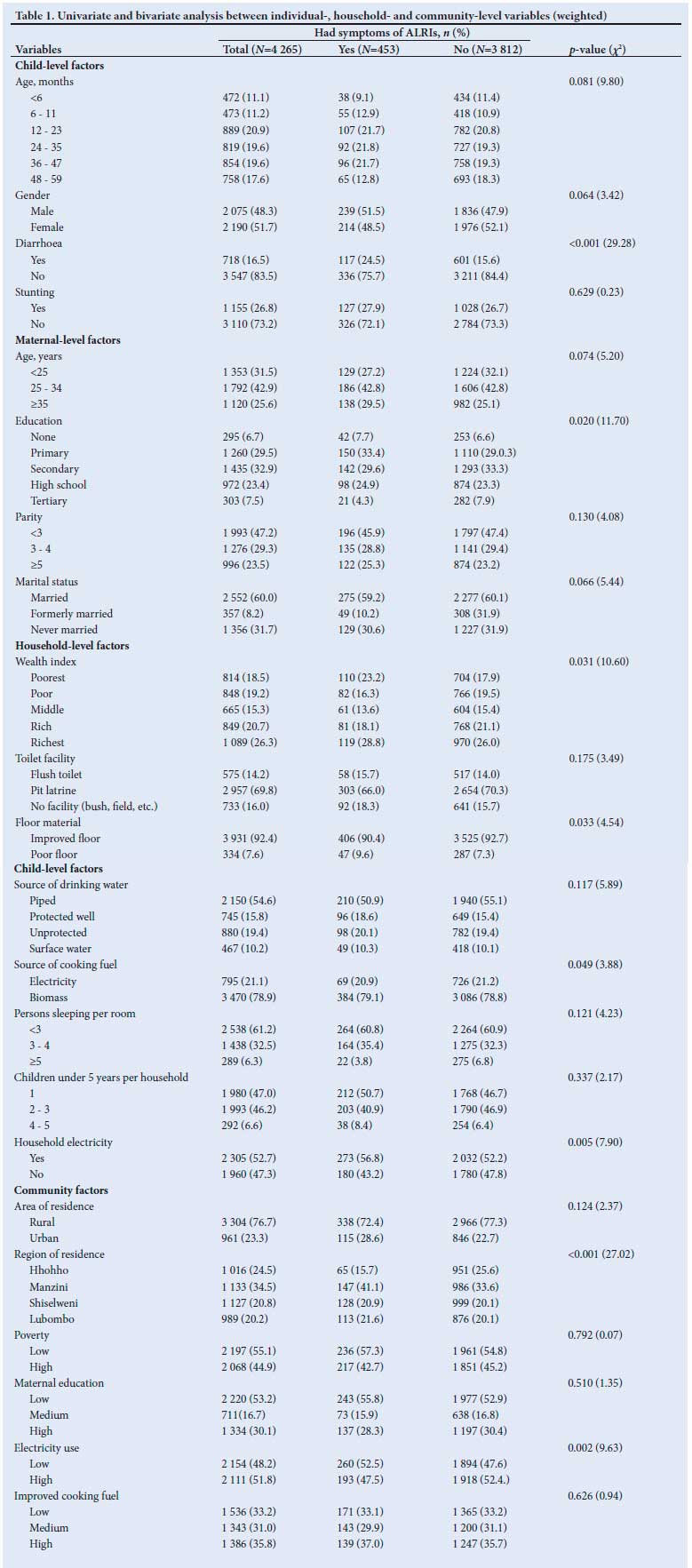
Table 1 shows the distribution of the study sample and the overall prevalence of ALRIs by each explanatory variable. Of the total sample (n=4 265) included in the analysis, there was a relatively equal distribution of children from 12 months of age and above, when compared with children 6 - 11 months and <6 months. Slightly more than half of the children were female and a quarter were reported to be stunted, while a quarter were born to mothers aged 35 years and above and one-third of mothers had secondary education level. Almost half of the children were born to mothers with parity of less than three children. About six in 10 of the children were born to mothers who were married, and slightly more than a quarter were from the richest households category. More than half of the children were from households with access to piped water for drinking, with improved floor material and which used biomass for cooking. The majority were from rural areas.
Overall the ALRIs prevalence was 11.1% (95% CI 10.0 - 12.4).
Significant differences in the prevalence of ALRIs were noted regarding child diarrhoea status 2 weeks before the survey, maternal education, household floor material, household electricity, household wealth index, region of residence and proportion of households with electricity in the community (all p<0.05).
Multilevel analysis
The results of the models are shown in Table 2. Even after controlling for individual- and community-level factors (model 4), children who had a history of diarrhoea were 75% more likely to have ALRIs (aOR 1.75; 95% CI 1.37 - 2.23) compared with those who had no history of diarrhoea. Higher odds of ALRIs were observed among children born to women with no formal education (aOR 2.60; 95% CI 1.34 - 5.04) and those with primary level education (aOR 1.91; 95% CI 1.08 - 3.37) compared with those born to women with tertiary education. Even after controlling for individual- and community-level factors, children from households in urban areas were 59% more likely to have ALRIs (aOR 1.59; 95% CI 1.15 - 2.20) compared with children from rural areas. Consistent with model 2, higher odds of ALRIs were found among children from Manzini (aOR 2.19; 95% CI 1.59 - 3.12), Shiselweni (aOR 1.73; 95% CI 1.23 - 2.44), and Lubombo (aOR 1.77; 95% CI 1.25 - 2.51) compared with the Hhohho region. In the final model, children from communities with a low proportion of households with electricity had higher odds of having ALRIs (aOR 1.53; 95% CI 1.15 - 2.04) compared with those from communities with high access to electricity.
The results also revealed a significant variation of child ALRIs across communities (t=0.389; p<0.05 (model 1)). The empty model (model 1) further showed the ICC of 4.39%, indicating that the variation of child ALRIs could be attributed to the difference in the composition of the communities where the children resided. After controlling for individual-level factors (model 2), the total variance of child ALRIs remained significant and reduced, indicating that individual-level factors explained a fraction of the variance. The PCV showed that the individual-level factors explained 7.30% of the variance in the odds of having ALRIs. In model 3, only the community factors were entered; the total variance became insignificant but reduced. The PCV of model 3 showed that the community-level factors could explain about 46.09% of the community variance. After including both individual- and community-level factors in one model (model 4), the variance reduced but became insignificant. The PCV of the final model (model 4) showed that 54.13% of the total variance of child ALRIs across communities could be explained by the individual- and community-level factors combined. Among the four models, model 4 had an Akaike information criterion (AIC) of 2 843.35, indicating the model to be parsimonious when compared with the other models.
Discussion
Our study reported a prevalence of ALRIs that is 11.1% (95% CI 10.0 - 12.4). Compared with other nationwide demographic and health surveys, our prevalence was similar to Cameroon (11.3%) but lower than Zambia (34.2%), Tanzania (35.2%), and Lesotho (35.2%).[24] The monitoring of illnesses, including ALRIs, is in line with the SDGs, especially goal number 3, target 3.2, to end preventable diseases and deaths of under-5-year-old children by the year 2030[25,26] and reduce child mortality to below 25 deaths per 1 000 live births.[25]
Evidence from the literature showed increased odds of child ALRIs among children who had a history of diarrhoea.[27,28] In cross-sectional studies done in Kushtia, Bangladesh and Ethiopia, children who presented with a history of diarrhoea had higher odds of having ALRIs.[28,29] We found that the odds of developing ALRIs were nearly two times higher among children who were reported to have had diarrhoea compared with children who had no history of having diarrhoea. A possible explanation could be that concomitant illnesses may have lowered the children's immunity, making them susceptible to diseases such as ALRIs.[30]
As expected, we found that children born to mothers with no formal education and those with primary education level had higher odds of having ALRIs. Our study is consistent with the literature.[20,27] Formal education may assist mothers to improve their child care and hygiene practices that help to prevent diseases, including ALRIs.[31] Educated women possibly practise better health-seeking behaviour compared with uneducated women, which might help improve child health.[31]
Low socioeconomic status consistently shows poor health outcomes among children compared with those from higher socioeconomic status.[32] Poor households may have many risk factors for ALRIs, such as poor sanitation and cooking materials.[32] However, we found no significant association between household wealth status and ALRIs. In a cross-sectional study conducted in Ethiopia, there was no significant difference between the risk of ALRIs between children from the poorest and economically affluent households.[33]
We found that children who were resident in urban areas were more likely to have ALRIs compared with those in rural areas. One possible reason is that the atmosphere in urban areas has significantly higher levels of man-made air pollutants from the combustion of car engines, use of aged diesel vehicles, and combustion of biomass, which predispose children to ALRIs. Evidence suggests that as areas become less urban, the air quality improves.[34] In Rwanda, an assessment of the atmosphere in Kigali urban boundary showed that the concentration of pollutants includes dust (20%), fly ashes (25%), kerosene (13%), diesel soot (29%) and organic material (12%).[35]
Consistent with previous literature,[28,35] we found a significant variation of ALRIs across the administrative regions. We found that being a resident from Manzini, Shiselweni and the Lubombo regions was associated with higher odds of ALRs. This could be due to the fact that the three regions are less developed compared with the Hhohho region. Similarly, in Nigeria and Ethiopia, there was a significant association between the region of residence and ALRIs.[28,36]
Children from communities with a low connection to electricity were found to have increased odds of having ALRIs. Investment in household infrastructure, such as electricity, has huge health benefits for the community, such as the reduction in indoor air pollution.[36] A cross-sectional study done in Nigeria, however, found no significant association between communities with low and high connectivity to electricity.[22]
Study strengths and limitations
The results should be interpreted with a few noted limitations. The outcome of interest (ALRIs) were self-responses from the mother or caregiver, which can result in misclassification of children on the basis of ALRIs symptoms. The study aggregated the communitylevel factors at the EA; this may have resulted in some children being misclassified. Some variables could be essential to understand the association and variation of ALRIs but were not investigated since they were not available in the dataset or because it had substantial missing data. For example, child HIV status and environmental factors, such as climate in specific regions, were not available in the dataset while there were substantially missing data for vitamin A and child birth size questions. Regardless of the limitations in our study, the MICS was a nationally representative survey. We used design-based modelling that accounted for the complex sampling approach of the survey and it controlled the clustering of ALRIs at the cluster level.
Conclusions
In summary, the study findings indicate that the odds of ALRIs in children under 5 years of age in Eswatini is high among children with a history of diarrhoea, born to women with no formal education or primary education, resident in urban areas, from the Manzini, Shiselweni and Lubombo regions, and communities with a low proportion of households with electricity. The findings on individual and community determinants of ALRIs within the context of Eswatini were able to advance our knowledge. This will allow policymakers and researchers to evaluate the effectiveness of existing interventions and programmes that aim to improve the health of young children.
Declaration. This work was done under the Population Studies Doctoral Programme in the School of Built and Development Studies, University of KwaZulu-Natal (UKZN).
Acknowledgements. The authors would like to thank the Eswatini Central Statistics Office and UNICEF for providing access to the datasets.
Author contributions. MSS conceived the research idea, performed the statistical analysis, and prepared the initial draft of the manuscript. KV critically reviewed the manuscript and contributed to the study design and manuscript writing. Both authors reviewed and approved the final manuscript.
Funding. The authors would like to acknowledge the financial support for the doctoral work from the UKZN. However, the views, opinions, assumptions, or any other information presented in this article are solely those of the authors.
Conflicts of interest. None.
References
1. Black R, Cousens S, Johnson HL, et al., Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010;375(9730):1969-1987. https://doi.org/10.1016/s0140-6736(10)60549-1 [ Links ]
2. Banda W, Mazaba-Liwewe M, Mulenga D, Siziya S. Risk factors associated with acute respiratory infections among under-five children admitted to Arthur's Children Hospital, Ndola, Zambia. Asian Pacific J Health Sci 2016;3:153-159. [ Links ]
3. Simon JL, Daelmans B, Boschi-Pinto C, Aboubaker S, Were W. Child health guidelines in the era of sustainable development goals. BMJ 2018;362. https://doi.org/10.1136/bmj.k3151 [ Links ]
4. Blomstedt Y, Bhutta ZA, Dahlstrand J, et al. Partnerships for child health: Capitalizing on links between the sustainable development goals. BMJ 2018;360. https://doi.org/10.1136/bmj.k125 [ Links ]
5. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980 - 2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390(10100):1151-1210. https://doi.org/10.1016/S0140-6736(17)32152-9 [ Links ]
6. Walker C, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta Z. Global burden of childhood pneumonia and diarrhoea. Lancet 2013;38(9875):1405-1416. https://doi.org/10.1016/s0140-6736(13)60222-6 [ Links ]
7. Black R, Morris S, Bryce J. Where and why are 10 million children dying every year? Lancet 2003;361(9376):2226-2234. https://doi.org/10.1016/s0140-6736(03)13779-8 [ Links ]
8. International Vaccine Access Center (IVAC). Pneumonia and diarrhea progress report: Sustainable progress in the post-2015 era. Baltimore: IVAC, 2015. https://www.jhsph.edu/ivac/wp-content/uploads/2018/04/IVAC-2015-Pneumonia-Diarrhea-Progress-Report.pdf (accessed 14 August 2020). [ Links ]
9. Adesanya OA, Chiao C. A multilevel analysis of lifestyle variations in symptoms of acute respiratory infection among young children under five in Nigeria. BMC Public Health 2016;16(1):880. https://doi.org/10.1186%2Fs12889-016-3565-0 [ Links ]
10. Taksande A, Mayuri Y. Risk factors of acute respiratory infection (ARI) in under-fives in a rural hospital in Central India. J Pediatr Neon Individ Med 2016;5(1): e050105. https://doi.org/10.7363/050105 [ Links ]
11. Alam M, Bhuia MR, Lovely NS, Kabir H, Das S. Acute respiratory infection and its determinants for Bangladesh under-5 children. J Progressive Sci Technol 2013;11:125-132. [ Links ]
12. Bellan SE, Pulliam JRC, Scott JC, Dushoff J, the MMED Organising Committee. How to make epidemiological training infectious. PLoS Biology 2012;10(4):e1001295. https://doi.org/10.1371%2Fjournal.pbio.1001295 [ Links ]
13. The World Bank Group. World development indicator Gini index. http://data.worldbank.org/indicator/SI.POV.GINI2015 (accessed 2 April 2019). [ Links ]
14. Anteneh Z, Hassen H. Determinants of acute respiratory infection among children in Ethiopia: A multilevel analysis from Ethiopian Demographic and Health Survey. Int J Gen Med 2020;13:17-26. https://doi.org/10.2147/IJGM.S233782 [ Links ]
15. Eswatini Central Statistical Office and UNICEF. Eswatini Multiple Indicator Cluster Survey 2014. Final Report. Mbabane, Eswatini: Central Statistical Office and UNICEF, 2016. [ Links ]
16. Eswatini Central Statistical Office and UNICEF. Eswatini Multiple Indicator Cluster Survey 2010. Final report. Mbabane, Eswatini: Central Statistical Office and UNICEF, 2011. [ Links ]
17. Eswatini Central Statistics Office. Eswatini Population and Housing Census Report. Mbabane: Government of Eswatini, 2007. [ Links ]
18. Adedokun ST, Adekanmbi VT, Uthman OA, Lilford RJ. Contextual factors associated with health care service utilisation for children with acute childhood illnesses in Nigeria. PLoS ONE 2017;12(3):e0173578. https://doi.org/10.1371/journal.pone.0173578 [ Links ]
19. Cárdenas-Cárdenas LM, Castañeda-Orjuela CA, Chaparro-Narváez P, Hoz-Restrepo FDl. Individual and climate factors associated with acute respiratory infection in Colombian children. Cadernos de Saúde Pública 2017;33(10):E00028216. https://doi.org/10.1590/0102-311X00028216. PMID.29091168. [ Links ]
20. Adesanya OA, Darboe A, Mendez Rojas B, Abiodun, Beogo I. Factors contributing to regional inequalities in acute respiratory infections symptoms among under-five children in Nigeria: A decomposition analysis. Int J Equity Health 2017;16(1):140. https://doi.org/10.1186%2Fs12939-017-0626-7 [ Links ]
21. Poirier MJP, Grépin KA, Grignon M. Approaches and alternatives to the wealth index to measure socioeconomic status using survey data: A critical interpretive synthesis. Soc Indicat Res 2020;148(1):1-46. https://doi.org/10.1007/s11205-019-02187-9 [ Links ]
22. Adedini SA, Odimegwu C, Imasiku E, Ononokpono D, Ibisomi L. Regional variations in infant and child mortality in Nigeria: A multilevel analysis. J Biosoc Sci 2015;47(2):165-187. https://doi.org/10.1017/s0021932013000734 [ Links ]
23. Huda TM, Chowdhury M, El Arifeen S, Dibley MJ. Individual and community-level factors associated with health facility delivery: A cross- sectional multilevel analysis in Bangladesh. PLoS ONE 2019;14(2):e0211113. https://doi.org/10.1371/journal.pone.0211113 [ Links ]
24. Seidu AA, Dickson KS, Ahinkorah BO, Amu H, Darteh EKM, Kumi-Kyereme A. Prevalence and determinants of acute lower respiratory infections among children under-five years in sub-Saharan Africa: Evidence from demographic and health surveys. SSM Popul Health 2019;8:100443. https://doi.org/10.1016/j.ssmph.2019.100443 [ Links ]
25. United Nations. Sustainable Development Goals Report. New York: United Nations, 2019. [ Links ]
26. World Health Organization. Sustainable development goals (SDGs): Goal 3. Target 3.2: By 2030, end preventable deaths of newborns and children under 5 years of age. Manila: WHO Regional Office for the Western Pacific, 2016. [ Links ]
27. Amugsi DA, Aborigo RA, Oduro AR, Asoala V, Awine T, Amenga-Etego L. Socio-demographic, and environmental determinants of infectious disease morbidity in children under 5 years in Ghana. Glob Health Action 2015;8(1):29349. https://doi.org/10.3402/gha.v8.29349 [ Links ]
28. Mena T. Multilevel logistic regression analysis of factors associated with acute respiratory infection (ARI) among under-five children in Ethiopia. World J Adv Healthcare Res 2020;4(1):44-51. [ Links ]
29. Rahman S. A study on the relationship between nutritional status and prevalence of pneumonia and diarrhoea among preschool children in Kushtia. Ped Res Int J 2014;10:805309. https://doi.org/10.5171/2014.805309 [ Links ]
30. Glennie SJ, Nyirenda M, Williams NA, Heyderman RS. Do multiple concurrent infections in African children cause irreversible immunological damage? Immunology 2012;135(2):125-132. https://doi.org/10.1111/j.1365-2567.2011.03523.x [ Links ]
31. Mondal RK, Majumder M, Rayhan S. The impact of maternal education on child health: Evidence from Bangladesh. Asian J Soc Sci Human 2014;3:19-27. [ Links ]
32. Chen E, Martin AD, Matthews KA. Understanding health disparities: The role of race and socioeconomic status in children's health. Am J Public Health 2006;96(4):702-708. https://doi.org/10.2105/AJPH.2004.048124 [ Links ]
33. Jabessa S. Multilevel analysis of acute respiratory infection symptoms among under-five children in Ethiopia. J Biometrics Biostats 2015;6(4):251. https://doi.org/10.4172/2155-6180.1000251. [ Links ]
34. Strosnider H, Kennedy C, Monti M, Yip F. Rural and urban differences in air quality, 2008-2012, and community drinking water quality, 2010 - 2015. MMWR Surveill Summ 2017;66(13):1-10. https://doi.org/10.15585/mmwr.ss6613a1 [ Links ]
35. Henninger SM. When air quality becomes deleterious. A case study for Kigali, Rwanda. J Environ Protect 2013;4(8):7. https://doi.org/10.4236/jep.2013.48A1001 [ Links ]
36. Akinyemi JO, Morakinyo OM. Household environment and symptoms of childhood acute respiratory tract infections in Nigeria, 2003 - 2013: A decade of progress and stagnation. BMC Infect Dis 2018;18(1):296. https://doi.org/10.1186/s12879-018-3207-5 [ Links ]
 Correspondence:
Correspondence:
M S Simelane
smasimelane@uniswa.sz
Accepted 30 September 2020


{kind=link}
{kind=link}