










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.14 n.3 Pretoria Sep. 2020
http://dx.doi.org/10.7196/sajch.2020.v14i3.1720
RESEARCH
A 5-year retrospective analysis of infant death at Salt River Mortuary, Cape Town
L J HeathfieldI, II; L J MartinIII; R RamesarIV
IPhD, PG Dip (Health Prof Educ); Division of Forensic Medicine and Toxicology, Faculty of Health Sciences, University of Cape Town, South Africa
IIPhD, PG Dip (Health Prof Educ); MRC/UCT Research Unit for Genomic and Precision Medicine, Division of Human Genetics, Institute of Infectious Diseases and Molecular Medicine, Department of Pathology, University of Cape Town, South Africa
IIIDip For Med (Path), MMed Path (Foren), FC For Path; Division of Forensic Medicine and Toxicology, Faculty of Health Sciences, University of Cape Town, South Africa
IVPhD, MBA; MRC/UCT Research Unit for Genomic and Precision Medicine, Division of Human Genetics, Institute of Infectious Diseases and Molecular Medicine, Department of Pathology, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Infant death is a distressing occurrence and unfortunately remains high in many parts of the world, including South Africa (SA). Despite much research into risk factors for infant death elsewhere, limited SA data are available, particularly pertaining to the city of Cape Town.
OBJECTIVE. To investigate the burden and profile of infant deaths admitted for medico-legal investigation in Cape Town, SA, with a focus on sudden unexpected death in infants (SUDI).
METHODS. A retrospective study of infant deaths admitted to Salt River Mortuary, Cape Town, SA, between 2013 and 2017 is reported.
RESULTS. A total of 1 608 infant deaths were reported over the 5-year study period (total caseload, N=17 730). Of the reported infant deaths, 1 199 (74.56%) cases were admitted as SUDI. Cause of death had been established for the majority of SUDI cases (89%) at autopsy, although 137 cases were undetermined or still under investigation at the time of study and pending ancillary investigations. Many risk factors for SUDI were observed, with co-sleeping documented in 94.65% of the cases. Co-sleeping was significantly associated with a side-sleeping position in infection-related deaths (p<0.001). More than half of the SUDI cases were exposed to tobacco smoke.
CONCLUSION. These results strongly advocate for the need for awareness campaigns in developing countries to educate caregivers about risk factors for infant death, particularly surrounding the risks of infection. Remarkable decreases in infant death in other countries have been noted following targeted awareness campaigns.
Infant death is a global concern and much research has been undertaken to better understand its causes and risk factors.[1-4] The infant mortality rate is recognised as an appropriate indicator to measure population health, as it reflects factors that affect the population at large.[5] The South African (SA) infant mortality rate remains high, with an estimated 29.9 deaths per 1 000 live births recorded in 2018.[6]
In response to this burden, several projects have been established in the Western Cape, SA, to better understand infant death. These include the local mortality surveillance system, which was implemented in 2007,[7] and the Child Death Review project, which was initially piloted in Cape Town and Durban (KwaZulu-Natal) from 1 January 2014, and has now been implemented across the Western Cape and also in some areas of KwaZulu-Natal.[8] Data from these projects showed that lower respiratory tract infections accounted for most infant deaths in parts of Cape Town, and -44.3% of these were associated with prematurity.[7,8]
These findings are contrary to what is reported from developed countries, where sudden infant death syndrome (SIDS) is deemed the leading cause of infant death and has a reported incidence of -0.33 per 1 000 live births.[9,10] SIDS is defined as the death of an infant younger than 1 year, whose cause of death remains unexplained after death scene investigation, clinical history review and a full autopsy[11] A substantial decline in SIDS rates has been observed in countries who adopted 'Back to Sleep' campaigns in the 1990s and early 2000s.[9,12] However, although absolute numbers decreased, SIDS still remains a global burden and concern.''
There is limited research pertaining to SIDS in SA. A retrospective analysis of cases of sudden unexpected death in infants (SUDI) at the Tygerberg Medico-legal Laboratory (Cape Town) and Pretoria Medico-legal Laboratory (Gauteng) between 2000 and 2004 showed that 161 (40.25%) SUDI cases were diagnosed as SIDS in Tygerberg, compared with 10 (9.17%) in Pretoria.[14] Similar results were also observed in another retrospective study, which analysed SUDI data for the period 2005 - 2009 from five of the seven major academic medico-legal mortuaries in the country. The results showed that of the SUDI cases, between 0% and 14.9% were classified as SIDS, with the highest rates seen at Tygerberg.[15] The large difference in SIDS diagnoses was attributed to, among other factors, the lack of a uniform national investigation protocol.[14,15] It has also been highlighted that death scene investigation is largely neglected in SA, despite its essential role in and value to a SUDI investigation.[16,17]
There is little representation of infant death cases from Salt River Mortuary (Cape Town) in the literature. It is imperative that the causes and risk factors of infant death are captured accurately so that locally relevant interventions can be implemented. The aim of this study was therefore to review infant deaths investigated at Salt River Mortuary to better understand forensic investigation procedures, circumstances at death, demographics and risk factors in the immediate local community.
Methods
This study received institutional ethical approval (ref no. HREC 445/2015). All infant death cases admitted to Salt River Mortuary for forensic investigation between 1 January 2013 and 31 December 2017 were reviewed, including those thought to be due to unnatural causes as defined in the National Health Act No. 61 of 2003.[18] Cases of individuals younger than 1 year at the time of death were extracted from the internal autopsy database. The unique case numbers were then used to retrieve the medico-legal case folders from the archives to collect data pertaining to each case. The case numbers were subsequently replaced by a unique study number to preserve confidentiality.
For each case, information pertaining to demographics, environment, death scene, circumstances surrounding death, risk factors, forensic investigation and cause of death was collected. For most cases, particularly those admitted as 'SUDI', additional documentation was available; this included the infant's clinic card (locally known as the 'Road to Health' card, which records vaccination, development milestones and clinical consults from birth), as well as scene documentation and a comprehensive family questionnaire for SUDI cases, which was specifically designed in accordance with international guidelines.[19]
Autopsies of SUDI cases (1 day - 1 year old) were classified as follows:
• Full: External and internal examination with ancillary investigations (i.e. ancillary investigations needed to determine cause of death)
• Partial: External examination with partial internal examination or minimally invasive ancillary tests
• External: Only external examination.
At Salt River Mortuary, ancillary tests mainly include histopathology, toxicology and microbiology, and to a lesser extent, virology and biochemistry. All autopsies include a full-body X-ray scan using the Xmplar-DR system (Lodox Systems, SA). In addition to death scene investigation and clinical history review, a full autopsy with all ancillary investigations was required for a diagnosis of SIDS to be considered.[11]
Data were entered into an Excel spreadsheet version 13 (Microsoft Corp., USA) and a subset was checked by an independent researcher as a quality measure. Graphs were generated using GraphPad Prism v.6 (GraphPad Software, USA) or Excel version 2013 (Microsoft Corp., US) and statistics were performed using the built-in statistics functions in these software packages. Descriptive statistics were used to summarise the data. Variables that were unavailable or not recorded for specific cases were recorded as 'missing' and those entries were excluded from statistical analysis. The X2 test was used to test for significant differences between categorical variables, with a significance level of p<0.05 being used.
As is often the case in retrospective reviews, some data were found to be missing - either owing to misplaced documentation or questions that were not answered during the postmortem investigation process. Although the number of SUDI cases and the associated demographic information are comprehensive, the lack of data available was a limitation during the study, particularly with regard to understanding the risk factors associated with SUDI.
Results
All infants
A total of 17 730 cases were admitted to Salt River Mortuary between 2013 and 2017, of which 1 608 (9.07%) were infants younger than 1 year. Between 280 and 344 infant deaths were recorded per year (median: 321). Of the total number of infant deaths, 1 199 (74.56%) were admitted for medico-legal investigation under the category 'sudden unexpected death';[18] SUDI cases therefore represented 6.76% of the total caseload at the mortuary. The remaining infant death cases (25.54%) were admitted for investigation under the following categories:
• Act of omission or co-mission: Allegedly abandoned neonates (n=302; 18.78%)
• Application of external force: Alleged homicide or accidents (n=46; 2.86%)
• Procedure-related deaths (n=61; 3.79%).
Neonatal admissions were reviewed separately,[20] and therefore did not form part of this study.
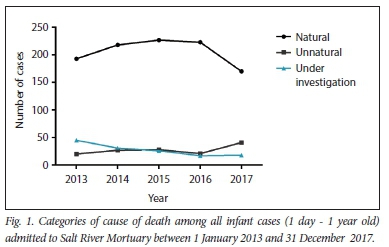
Following postmortem investigation, the causes of death of infants between 1 day and 1 year old were categorised as natural (64.18%), unnatural (27.30%) or being under investigation (8.52%). Significantly more deaths were classified as natural than unnatural or under investigation (p<0.0001)The overall trend over the 5-year period was that unnatural deaths increased, whereas natural deaths and cases under investigation decreased (Fig. 1).
SUDI cases
Demographics
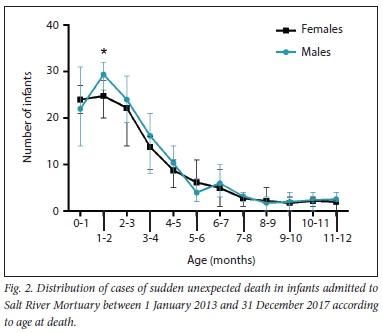
Slightly more of the SUDI cases were male (51.71%) than female (48.29%). The majority of cases were indigenous black African infants (57.88%), followed by infants from mixed ancestry (41.53%) and European descent (0.58%). No cases of Asian ancestry were noted. Most infants demised before 4 months of age (73.56%), with a peak of deaths at 1 - 2 months of age (Fig. 2). Significantly more male than female infants demised in this age group (p=0.046).
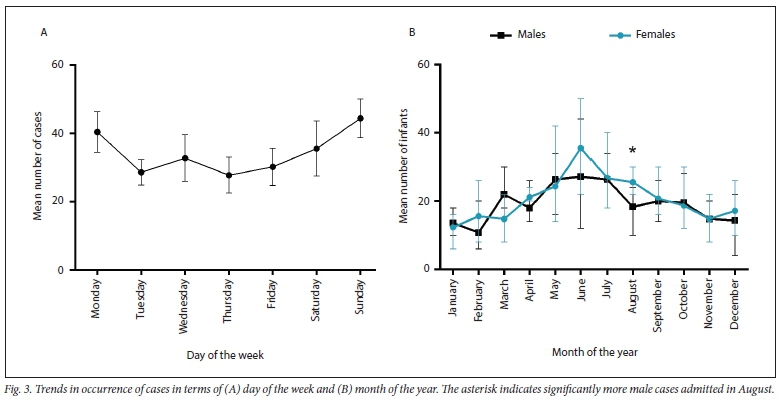
Approximately half of the SUDI cases occurred on weekends (50.21%), up until the early hours of Monday mornings (Fig. 3A). A peak in SUDI cases was observed during winter months (June - August), with the highest percentage of admissions in June (13.09%). Significantly more male SUDI cases (compared with female cases) were noted only in August (p=0.048) (Fig. 3B).
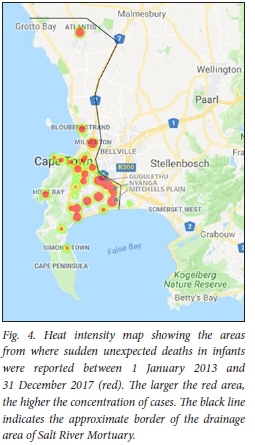
The highest percentage of SUDI cases was reported from Nyanga (19.02%), followed by Mitchells Plain (11.01%) and Gugulethu (10.26%). These townships comprise informal settlements, have a high population density and are generally considered to be low-income areas. The heat map in Fig. 4 shows the approximate locations and concentrations of SUDI reports.
Postmortem factors
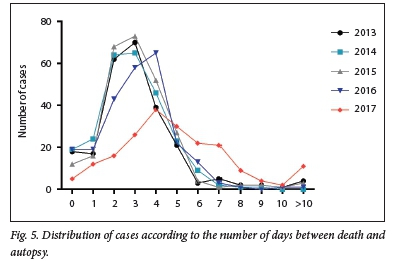
The majority of SUDI cases (78.83%) were autopsied within 4 days after death (mode: 3 days), with only -4% of cases being autopsied after 7 days (Fig. 5). The scope of autopsy for SUDI cases was full (19.32%), partial (15.84%) and external (64.84%) examinations. Histology was the most commonly performed ancillary investigation (30.39%), followed by microbiology (21.77%) and toxicology (11.72%). A full-body X-ray scan was performed in 94.91% of cases; only when the X-ray facility was not working were scans not performed.
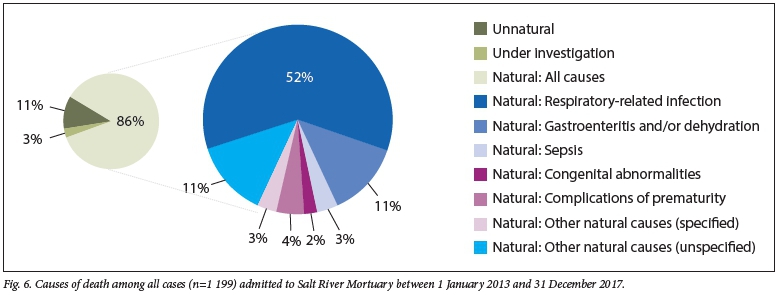
Postmortem examination showed that the causes of admitted SUDI cases were mostly natural (n=1032; 86%), with unnatural cause of death recorded in only 30 cases (3%); cause of death in the remaining 11% of cases (n=137) was still under investigation at the end of data collection (Fig. 6). Natural causes of death were mostly related to respiratory infections, followed by gastroenteritis or associated dehydration and unspecified natural causes of death (Fig. 6). Unnatural deaths were due to asphyxia (n/N=9/30; 30%), aspiration (n/N=18/30; 60%), and other causes (blunt force trauma, hypothermia or head injury) (n/N=3/30; 10%).
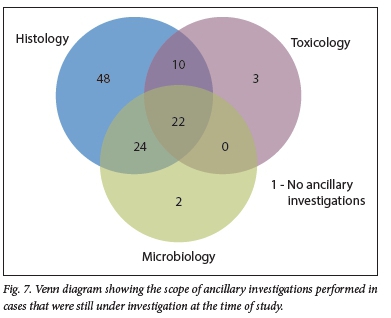
Of the SUDI cases that remained under investigation, information pertaining to the scope of postmortem investigation was available for 110 cases (Fig. 7). In addition to the external and internal autopsy, all three ancillary investigations (histology, toxicology, microbiology) were requested in 22 cases (20%). Of the remaining cases, one or two ancillary investigations were requested in 53 (48%) and 34 (31%) cases, respectively. No ancillary investigation was requested in 1 case (1%).
Risk factors
Numerous risk factors for SUDI were identified from the available documentation (Fig. 8). In the majority of cases (94.65%), infants co-slept in an adult bed, most commonly with one ortwo other individuals, but at times up to ten others. For infection-related deaths, co-sleeping was significantly associated with a side-sleeping position (p<0.001).
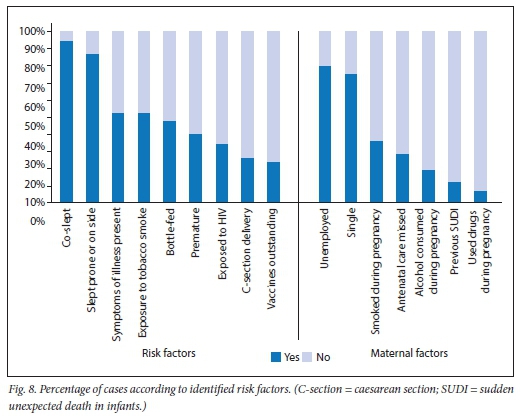
In 53.25% of SUDI cases, symptoms of illness were noted prior to death, yet mothers seldom took their infants to the clinic. Approximately one-third (34.90%) of infants were HIV exposed and almost a quarter (24.32%) had outstanding vaccinations. Premature infants represented 40.55% of cases. Although most infants were breastfed (51.82%), there was a significant association between infants who were bottle fed and gastroenteritis as the cause of death (p<0.001).
More than half of the infants in this study (53.11%) were exposed to tobacco smoke, mostly from their mothers (68.88%) or another family member in the household (32.12%). Most mothers were unemployed (80.22%) and single (75.43%). A previous SUDI was reported by 12.83% of mothers. Missed antenatal appointments, drinking alcohol and drug use were reported by 29.10%, 19.78% and 9.13% of mothers, respectively.
Discussion
The number of SUDI cases admitted to Salt River Mortuary (n=l 199) over the study period (2013 - 2017) is comparable to the number reported from Tygerberg Medico-legal Laboratory between 2005 and 2009 (n=l271).[15] However, the numbers are approximately double those reported from other major cities in SA[15] and substantially higher than in other countries.[12] To understand the reasons for this, the risk factors were explored. Most risk factors were in accordance with those reported internationally and locally in that slightly more male cases were reported, more deaths occurred during winter months and cases were mostly from regions with a lower socioeconomic profile.[15,21,22] However, most SUDI cases in the current study occurred in infants between the ages of 1 and 2 months, which is younger than the peak age of 2 - 4 months reported in developed countries.[21,23]
The peak of infant death has previously been explained with reference to a decreasing maternal IgG in the infant after birth.[24] We hypothesise that infants in crowded informal settlements, such as those seen in areas around Cape Town, are immunocompromised and that they experience a faster decrease in maternal IgG than infants in developed countries. In other words, vulnerable infants cannot cope with the volume of microorganisms and burden of disease associated with overcrowded living conditions,[25,26] and are thus succumbing to infections sooner than those is developed countries. This hypothesis would warrant testing by monitoring the decreasing levels of maternal IgG in newborns and investigating the microbiomes present in crowded and non-crowded living conditions.
The consequences of overcrowded living conditions can be observed in the high rate of infection-related causes of death (66%) among SUDI cases. Of these deaths, 52% were related to respiratory infections, 11% to gastroenteritis and 3% to sepsis. However, many infants survive these conditions every year, which raises the question of whether some infants are less able to cope with these pathogens than others. Such predispositions could be in the form of genetic variants, which could lead to a suboptimal immune response in some infants.[24] Possible genetic factors have not routinely been investigated in large-scale molecular autopsy studies, although some evidence for an association between SUDI and genetic variants in genes involved in immune functioning has been noted.[2729]
In the current study, only 26.56% of cases with respiratory causes of death had microbiology testing performed, and histology in 38.66%; the remainder of cases were diagnosed through a combination of chest X-ray and clinical history. It is plausible that in some of these cases the forensic pathologist decided not to perform the ancillary investigations owing to the time interval between death and postmortem, which would further complicate the already difficult interpretation of postmortem microbiology results. However, the majority of cases were refrigerated within 24 hours of declaration of death and an autopsy was performed within 4 days of death (Fig. 5), which has been shown to be a reliable timeframe for meaningful microbiology investigation provided there is refrigeration soon after death.[30,31]
The majority of infants in the study slept on their side, and side-sleeping was significantly associated with co-sleeping. Given the high rate of co-sleeping (94.65%) observed in this population, advocating for the use of a 'baby box' seems reasonable. The concept of the 'baby box' involves the infant being placed in a box on the floor next to the parents' or older siblings' bed and has been adopted in several countries since its introduction in Finland in 1938.[32-34] This intervention reduces the risk of the infant overheating or accidentally being smothered while sleeping in a bed with adults or older siblings,[33,34] although some cultural resistance towards the idea has been noted.[35]
However, the co-sleeping practices in this cohort may not be as modifiable as expected. In an ongoing study at the academic institution affiliated with the mortuary, conversations with mothers of SUDI cases have revealed that letting an infant sleep in a box on the floor would not be advisable because of possible rodent infestation in the home. Rodents can easily climb into a box on the floor or even eat through a plastic or cardboard box.[36] In addition to the lack of space or cots, rodent infestation appeared to be a burden in informal dwellings[37] and may contribute to infants co-sleeping with parents or siblings in these homes. A so-called 'Pepi-Pod', which is a polypropylene container with low sides and a fitted mattress, may offer a solution to the problem of co-sleeping, as it can be placed on a bed shared with parents or siblings without compromising the infant's space for breathing or the surrounding temperature.[32]
We observed a significant association between gastroenteritis as a cause of death and the absence of breastfeeding. This result is consistent with findings from other studies that reported breastfeeding to be protective against gastroenteritis and other infections.[38-40] Howie et al. [39] showed that infants who were breastfed for at least 13 weeks experienced significantly less diarrhoeal disease than those who were bottle fed.
Although Golding et al.[40] showed that breastfeeding may be protective against lower respiratory tract infections, this was not observed in the current study, as most infants who demised from such infections were breastfed; in fact, the majority of SUDI cases were exclusively breastfed (51.82%). This statistic is probably not a function of the mothers' knowledge about the protective factors of breastfeeding, but rather of the expense associated with milk or formula feed given the high rate of unemployed (80.22%) and single (75.43%) mothers noted in this study. This is further supported by findings from the last full SA census (2011), which revealed 47% of the population in Cape Town earning less than the minimum wage and 78.6% of individuals not having completed secondary school.[41]
A total of 12.83% of mothers in this study reported a previous SUDI, which is higher than what has been reported in other studies.[42,43] This may suggest recurrent risk factors in households (e.g. substance use, co-sleeping, etc.), but it could also suggest genetic factors. As genetic variants are inherited, it is plausible that genetic variants that contributed to SUDI in one infant may also affect a sibling. Some genetic variants can cause sudden disease without obvious signs or symptoms being observed (e.g. inherited channelopathies) and are therefore challenging to diagnose during a conventional postmortem investigation. Several forensic facilities abroad have introduced molecular autopsies to analyse pathogenic mutations causative of inherited cardiac disease, with promising resolution.[44,45] Introducing a molecular autopsy relevant to the SA setting should be explored to contribute to a better understanding of the causes of death in SUDI cases, particularly in those where the cause remains undetermined.
Some identified risk factors are mo difiable and need to be addressed urgently. These include mothers' attendance at antenatal care, adhering to the vaccination schedule and taking infants to the local clinic promptly when they show symptoms of illness. The latter is particularly important in the case of premature infants, even when mild symptoms of ill health are observed. Educational campaigns to inform mothers about risk factors and the importance of medical care are recommended. Such campaigns have been shown to contribute to reductions in infant death in other countries,[9] and given the high rate of SUDI reported in this study, it is a public health issue that requires resources and commitment by government.
Study limitations
As is often the case in retrospective reviews, some data were found to be missing -either owing to misplaced documentation or questions that were not answered during the postmortem investigation process. Although the number of SUDI cases and the associated demographic information are comprehensive, the lack of data available was a limitation during the study, particularly with regard to understanding the risk factors associated with SUDI.
Conclusion
These are the first data reported for SUDI cases from Salt River Mortuary. Our findings suggest that many infant deaths are avoidable and that some risk factors underpinning SUDI are modifiable. The burden of infection-related deaths motivates the need for prospective, molecular-based studies to better understand the immunological response of infants. The results from this study also highlight the need for campaigns to educate mothers and caregivers about risk factors of infant death. Although it is imperative that SUDI cases are investigated consistently within and across mortuaries, we should also recognise that interventions surrounding risk factors may reduce the burden of infant death in the first place. Forensic pathologists and scientists are encouraged to recognise their duties to public health and aim to translate these findings into community-based interventions, particularly pertaining to modifiable risk factors.
Declaration. This manuscript was submitted as part of a PhD in Human Genetics at the University of Cape Town.
Acknowledgements. The authors thank Mia Kruger and Gavin Pharo for assistance during data collection and Kyle Kulenkampff for technical assistance with Fig. 4.
Author contributions. LJH was responsible for project administration, developed the research methodology, collected, curated and analysed the data, and wrote the manuscript. LJM and RR contributed to sourcing resources, supervised the project and reviewed earlier drafts of the manuscript.
Funding. This research was funded by a Research Councils UK Newton Fund PhD Partnership award, the National Health Laboratory Service Development Trust Grant and the University Research Committee, University of Cape Town.
Conflicts of interest. None.
References
1. Trachtenberg FL, Haas EA, Kinney HC, Stanley C, Krous HF. Risk factol changes for sudden infant death syndrome after initiation of Back-to-Sleep campaign. Pediatrics 2012;129(4):630-638. https://doi.org/10.1542/peds.2011-1419 [ Links ]
2. Côté A, Russo P, Michaud J. Sudden unexpected deaths in infancy: What are the causes? J Pediatr 1999;135(4):437-443. https://doi.org/10.1016/s0022-3476(99)70165-4 [ Links ]
3. Opdal SH, Rognum TO. The sudden infant death syndrome gene: Does it exist? Pediatrics 2004;114(4):e506-512. https://doi.org/10.1542/peds.2004-0683 [ Links ]
4. Daltveit AK, Irgens LM, 0yen N, et al. Circadian variations in sudden infant death syndrome: Associations with maternal smoking, sleeping position and infections. The Nordic Epidemiological SIDS Study. Acta Paediatr 2003;92:1007-1013. [ Links ]
5. Reidpath DD. Infant mortality rate as an indicator of population health. J Epidemiol Community Health 2003;57(5):344-346. [ Links ]
6. Central Intelligence Agency. Country comparison: Infant mortality rate, https://www.cia.gov/library/publications/the-world-factbook/rankorder/2091rank.html (accessed 11 November 2019). [ Links ]
7. Groenewald P, Bradshaw D, Neethling I, et al. Linking mortuary data improves vital statistics on cause of death of children under five years in the Western Cape Province of South Africa. Trop Med Int Health 2016;21(1):114-121. https://doi.org/10.llll/tmi.12624 [ Links ]
8. Mathews S, Martin L, Scott C, Coetzee D, Lake L. Every child counts: Lessons learned from the South African Child Death Review pilot. A research brief. Cape Town: University of Cape Town, 2015. [ Links ]
9. Hauck FR,Tanabe KO. International trends in sudden infant death syndrome: Stabilization of rates requires further action. Pediatrics 2008;122(3):660-666. https://doi.org/10.1542/peds.2007-0135 [ Links ]
10. Byard RW, Krous HF. Sudden infant death syndrome: Overview and update. Pediatr Dev Pathol 2003;6(2):112-127. https://doi.org/10.1007/sl0024-002-0205-8 [ Links ]
11. Krous HF, Beckwith JB, Byard RW, et al. Sudden infant death syndrome and unclassified sudden infant deaths: A definitional and diagnostic approach. Pediatrics 2004;114(l):234-238. https://doi.Org/10.1542/peds.114.l.234 [ Links ]
12. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome and other sudden unexpected deaths in infancy: Need for better diagnostic standardization. Curr Pediatr Rev 2010;6(1):95-101. [ Links ]
13. Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: Final data for 2006. Natl Vital Stat Rep 2009;57(14):1-134. [ Links ]
14. Du Toit-Prinsloo L, Dempers JJ, Wadee SA, Saayman G. The medico-legal investigation of sudden, unexpected and/or unexplained infant deaths in South Africa: Where are we - and where are we going? Forensic Sci Med Pathol 2011;7(l):14-20. https://doi.org/10.1007/sl2024-010-9184-7 [ Links ]
15. Du Toit-Prinsloo L, Dempers J, Verster J, et al. Toward a standardized investigation protocol in sudden unexpected deaths in infancy in South Africa: A multicenter study of medico-legal investigation procedures and outcomes. Forensic Sci Med Pathol 2013;9(3):344-350. https://doi.org/10.1007/sl2024-013-9427-5 [ Links ]
16. Dempers JJ, Coldrey J, Burger EH, et al. The institution of a standardized investigation protocol for sudden infant death in the eastern métropole, Cape Town, South Africa. J Forensic Sci 2016;61(6):1508-1514. https://doi.org/10.1111/1556-4029.13204 [ Links ]
17. Bennett T, Martin LJ, Heathfield LJ. Global trends in the extent of death scene investigation performed for sudden and unexpected death of infant (SUDI) cases : A systematic review. Forensic Sci Int 2019;301:435-444. https://doi.org/10.1016/j.forsciint.2019.06.013 [ Links ]
18. South Africa. National Health Act No. 61 of 2003. [ Links ]
19. Centers for Disease Control and Prevention. Sudden unexplained infant death investigation (SUIDI) reporting form, https://www.cdc.gov/sids/pdf/suidi-form2-l-2010.pdf (accessed 11 November 2019). [ Links ]
20. Du Toit C, Martin LJ, Heathfield LJ. Investigation into abandoned neonates admitted to Salt River Forensic Pathology Mortuary, Cape Town. Forensic Sci Int 2018;292:232-241. https://doi.Org/10.1016/j.forsciint.2018.09.031 [ Links ]
21. Blair PS, Sidebotham P, Berry PJ, Evans M, Fleming PJ.Major epidemiological changes in sudden infant death syndrome: A 20-year population-based study in the UK. Lancet 2006;367(9507):314-319. https://doi.org/10.1016/s0140-6736(06)67968-3 [ Links ]
22. Molteno CD, Ress E, Kibel MA. Early childhood mortality in Cape Town. S AfrMedJ 1989;75(12):570-574. [ Links ]
23. Fleming P, Blair P, Bacon C, Berry P. Sudden unexpected deaths in infancy. The CESDI SUDI studies 1993 - 1996. London: Stationary Office, 2000. [ Links ]
24. Blackwell CC, Moscovis SM, Gordon AE, et al. Cytokine responses and sudden infant death syndrome: Genetic, developmental, and environmental risk factors. J Leukoc Biol 2005;78(6):1242-1254. https://doi.org/10.1189/jlb.0505253 [ Links ]
25. Webb PM, Knight T, Greaves S, et al. Relation between infection with Helicobacter pylori and living conditions in childhood: Evidence for person tc person transmission in early life. BMJ 1994;308(6931):750-753. https://doi.org/10.1136/bmj.308.6931.750 [ Links ]
26. Le Roux DM, Myer L, Nicol MP, Zar HJ. Incidence of childhood pneumonia: Facility-based surveillance estimate compared to measured incidence in a South African birth cohort study. BMJ Open 2015;5(12):e009111. https://doi.org/10.1136/bmjopen-2015-009111 [ Links ]
27. Ferrante L, Opdal SH, Vege A, Ro gnum TO. IL-1 gene cluster polymorphisms and sudden infant death syndrome. Hum Immunol 2010;71(4):402-406. https://doi.Org/10.1016/j.humimm.2010.01.011 [ Links ]
28. Opdal SH, Rognum TO. The IL6-174G/C polymorphism and sudden infant death syndrome. Hum Immunol 2007;68(6):541-543. https://doi.org/10.1016/j.humimm.2007.02.008 [ Links ]
29. Opdal SH, Opstad A, Vege Â, Ro gnum TO. IL-10 gene polymorphisms are associated with infectious cause of sudden infant death. Hum Immunol 2003;64( 12):1183-1189. https://doi.Org/10.1016/j.humimm.2003.08.359 [ Links ]
30. Tuomisto S, Karhunen PJ, Vuento R, Aittoniemi J, Pessi T. Evaluation of postmortem bacterial migration using culturing and real-time quantitative PCR. J Forensic Sci 2013;58(4):910-916. https://doi.org/10.llll/1556-4029.12124 [ Links ]
31. Tsokos M, Püschel K. Postmortem bacteriology Ín forensic pathology Diagnostic value and interpretation. Leg Med 2001;3(l):15-22. https://doi.org/10.1016/sl344-6223(01)00002-5 [ Links ]
32. Young J, CraÍgÍe L, Hine H, Kosiak M. Safe sleep advice to safe sleep action: Trial of an innovative Safe Infant Sleep Enabler -The Pepi-Pod. Women Birth 2013;26(Suppll):S40. https://doi.Org/10.1016/j.wombi.2013.08.219 [ Links ]
33. Ross LA. Baby boxes: Improving wellbeing outcomes Ín Scotland. J Health Visit 2017;5(4):172-175. [ Links ]
34. Wennergren G, Nordstrand K, Aim B, et al. Updated Swedish advice on reducing the risk of sudden infant death syndrome. Acta Paediatr 2015;104(5):444-448. https://doi.org/10.llll/apa.12966 [ Links ]
35. Moon RY, Hauck FR, Colson ER. Safe infant sleep interventions: What Ís the evidence for successful behavior change? Curr Pediatr Rev 2016;12(l):67-75. https://doi.org/10.2174/1573396311666151026110148 [ Links ]
36. Meerburg BG, Singleton GR, Kijlstra A. Rodent-borne diseases and their risks for public health. Crit Rev Microbiol 2009;35(3):221-270. https://doi.org/10.1080/10408410902989837 [ Links ]
37. Mathee A, Barnes B, Naidoo S, Swart A, Rother HA. Development for children's environmental health Ín South Africa: Past gains and future opportunities. Dev South Afr 2018;35(2):283-293. https://doi.0rg/l0.l080/0376835X.2017.1419857 [ Links ]
38. Feachem RG, KobÜnsky MA. Interventions for the control of diarrhoeal diseases among young children: Promotion of breast-feeding. Bull World Health Organ 1984;62(2):271-291. [ Links ]
39. Howie PW, Forsyth JS, Ogston SA, Clark A, Florey CD. Protective effect of breast feeding against infection. BMJ 1990;300(6716):11-16. https://doi.org/10.1136/bmj.300.6716.11 [ Links ]
40. Golding J, Emmett PM, Rogers IS. Does breast feeding protect against non-gastric infections? Early Hum Dev 1997;49(Suppl):Sl05-Sl20. https://doi.org/10.1016/s0378-3782(97)00056-x [ Links ]
41. Statistics South Africa. City of Cape Town. 2011. http://www.statssa.gov.za/?page_id=1021&id=city-of-cape-town-municipality (accessed 18 June 2018). [ Links ]
42. Hunt CE. Sudden infant death syndrome and other causes of infant mortality Am J Respir Crit Care Med 2001;164(3):346-357. [ Links ]
43. Oyen N, Skjaerven R, Irgens LM. Population-based recurrence risk of sudden infant death syndrome compared with other infant and fetal deaths. Am J Epidemiol 1996;144(3):300-305. https://doi.org/10.1093/oxfordjournals.aje.a008925 [ Links ]
44. Hertz CL, Christiansen SL, Ferrero-Miliani L, et al. Next-generation sequencing of 34 genes Ín sudden unexplained death victims in forensics and Ín patients with channelopathic cardiac diseases. Int J Legal Med 2015;129(4):793-800. https://doi.org/10.1007/s00414-014-1105-y [ Links ]
45. Ackerman MJ. State of postmortem generic testing known as the cardiac channel molecular autopsy Ín the forensic evaluation of unexplained sudden cardiac death in the young. Pacing Clin Electrophysiol 2009;32(Suppl 2):S86-S89. https://doi.Org/10.llll/j.1540-8159.2009.02393.x [ Links ]
 Correspondence:
Correspondence:
L J Heathfield
laura.heathfield@uct.ac.za
Accepted 10 December 2019


{kind=link}
{kind=link}