










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.14 no.1 Pretoria Abr. 2020
http://dx.doi.org/10.7196/SAJCH.2020.v14.i1.01666
RESEARCH
Congenital anomalies of the kidney and the urinary tract in a South African paediatric nephrology setting
N C OkoronkwoI; C LevyII; T KhumaloIII; G MoonsamyIV
IMBBS, FWACP, MSc; A Mudi, MB BCh, MMed, FCPaed, Cert Nephrol (Paed); Division of Paediatric Nephrology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IIMB BCh, MMed, FCPaed, Cert Nephrol (Paed); Division of Paediatric Nephrology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IIIMB BCh, MMed, FCPaed, Cert Nephrol (Paed); Division of Paediatric Nephrology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IVMB BCh, MMed, FCPaed, Cert Nephrol (Paed) Division of Paediatric Nephrology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Congenital anomalies of the kidney and the urinary tract (CAKUT) are responsible for 34 - 59% of chronic kidney disease (CKD) and for 30 - 50% of cases of end-stage renal disease (ESRD) in children.
OBJECTIVE. The aim of this study was to document the frequency and types of CAKUT in our centre.
METHODS. Patients aged between 2 weeks and 18 years with CAKUT, who attended the paediatric nephrology division of the Charlotte Maxeke Johannesburg Academic Hospital over a 10-year period, were retrospectively reviewed. The different types of CAKUT were classified into anomalies of the kidney, anomalies of the collecting system, anomalies of the bladder, and anomalies of the urethra.
Results. Over the study period (January 2005 - December 2014), 138 patients presented with CAKUT, giving a proportion for CAKUT of 20% of the total number of patients seen. However, 4 records were excluded from analysis because the patients were lost to follow-up. There were 109 male and 25 female patients, giving a male:female ratio of 4.4:1. The median age (interquartile range (IQR)) at presentation was 8.4 (IQR 1.9 - 47.7) months. The most common type of CAKUT was anomalies of the urethra (n=60; 45%), while the least was anomalies of the bladder (n=10; 7%). The percentage of primary vesicoureteral reflux (VUR) in our study was 4.5%. Posterior urethral valve was the only form of urethral anomaly documented in the study.
CONCLUSION. The percentage of CAKUT in our setting is significant. Anomalies of the urethra were the most common CAKUT while anomalies of the bladder were the least. The frequency of VUR in South African children is much lower than that described in developed countries. Children with CAKUT should be on regular medical follow-up to prevent both early and late complications.
Congenital anomalies of the kidney and the urinary tract (CAKUT) result from faulty development of the renal system which may occur in isolation (confined to the kidney and urinary tract), or may manifest as part of a syndrome with additional congenital malformations outside the kidney.[1] It occurs in 3 - 6 per 1 000 live births, and also constitutes about 20 - 30% of all anomalies identified in the prenatal period.[2-4] CAKUT comprises a wide range of renal system structural and functional malformations that may occur at the level of the kidney (e.g. hypoplasia and dysplasia), collecting system (e.g. hydronephrosis and mega-ureter), bladder (e.g. ureterocoele, vesicoureteral reflux and vesicoureteral junction obstruction (VUR)) or urethra (e.g. posterior urethral valves (PUV)).[1] The prevalence of CAKUT among the general paediatric population ranges between 3.5 and 26.6%.[5,6]
With improved prenatal screening, many cases of CAKUT are diagnosed by antenatal ultrasonography performed at 18 - 20 weeks' gestation.[7,8] Most common antenatal manifestations of CAKUT include oligohydramnios or variations in gross morphology of the kidney, ureter or bladder. Postnatal manifestations can be the presence of a palpable abdominal mass, single umbilical artery, feeding difficulties, decreased urinary output, deficient abdominal wall musculature, and undescended testes in a male infant or multi-organ birth defects.[7] Ultrasonography, contrast radiography (e.g. voiding cysto-urethrogram and intravenous urography), cystoscopy and Technetium 99 mercaptoacetyltriglycine (Tc99- MAG3) scanning can also be used to diagnose CAKUT.[9] The diagnosis of urinary tract infection (UTI) in children is often a marker for CAKUT in the postnatal period.[5] Most children with CAKUT are referred to the renal clinic because of UTI symptoms. Those without symptoms do not come to the clinic. The diagnosis of CAKUT in the latter group is often missed in an otherwise seemingly healthy paediatric population. Unfortunately, such patients may subsequently present later with chronic kidney disease (CKD).
It is standard practice to screen for CAKUT in certain groups of children with UTI. These include children with delayed or unsatisfactory response to treatment of the first febrile UTI, presence of abdominal mass or abnormal voiding, and causative organism other than Escherichia coli.[9-11] A major significance of CAKUT as a clinical entity is in predisposing patients to UTI. Some forms of CAKUT may also predispose to renal scarring, calculi formation, hypertension and CKD even in the absence of recurrent UTI.[12-14]
CAKUT is responsible for 34 - 59% of CKD and for 30 - 50% of cases of end-stage renal disease (ESRD) in children.[2-4]
Although some studies have been done on CAKUT, its prevalence, pattern among general paediatric populations, antenatal diagnosis, reviews and outcomes, methods of diagnosis, and recently its genetic aetiology,[1-7-12-15] there is a paucity of literature on the prevalence of CAKUT and the different types, as seen in the South African (SA) population.
Methods
This study was conducted in the Division of Paediatric Nephrology of the Charlotte Maxeke Johannesburg Academic Hospital in Johannesburg, SA, which is a large teaching hospital attached to a major SA university. This division provides comprehensive paediatric nephrology services to children referred from its surrounding area. The study was a 10-year (January 2005 - December 2014) descriptive retrospective review of all patients between 2 weeks and 18 years of age with documented CAKUT, who attended the Division of Paediatric Nephrology within the study period.
Relevant information for the study for patients who satisfied the criteria for CAKUT were extracted from files stored in the paediatric nephrology division of the hospital. CAKUT was documented initially according to the exact diagnosis on the patients' files, and was later classified into anomalies of the kidney, anomalies of the collecting system, anomalies of the bladder, and anomalies of the urethra. All the urethral anomalies reported were of the posterior urethral valves (PUVs), and hence the latter term was used in place of 'anomalies of the urethra'.
The Chief Executive Officer of the hospital granted permission for the study. Ethical clearance (ref. no. M150709) was obtained from the Human Research Ethics Committee and the Postgraduate Committee of the University of the Witwatersrand before commencement of the study.
Data analysis was done using the statistical software STATA version 13 (StataCorp., USA). A A-value <0.05 was taken as statistically significant, with a confidence interval of 95%.
Results
Over the study period, 691 patients were seen at the clinic, of whom 138 were diagnosed with CAKUT; this gave a prevalence of 20% for CAKUT in children referred to our Division of Paediatric Nephrology over the study period. Four records were excluded from analysis because the patients were lost to follow-up. Of the remaining 134 patients, 109 were male and 25 female, giving a male:female ratio of 4.4:1 (Table 1). The median age at presentation was 8.4 months (interquartile range (IQR) 1.9 - 47.7) and the median duration of follow-up was 39 months (IQR 12.5 - 81.7).

Fig. 1 shows the distribution of the different classes of CAKUT among the study population. Anomalies of the urethra were the most common, while anomalies of the bladder were the least common anomaly seen.

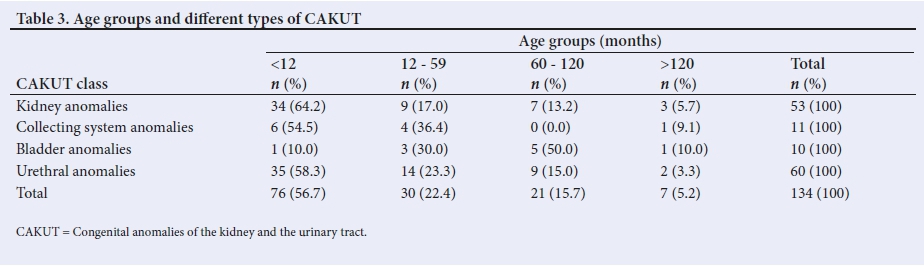
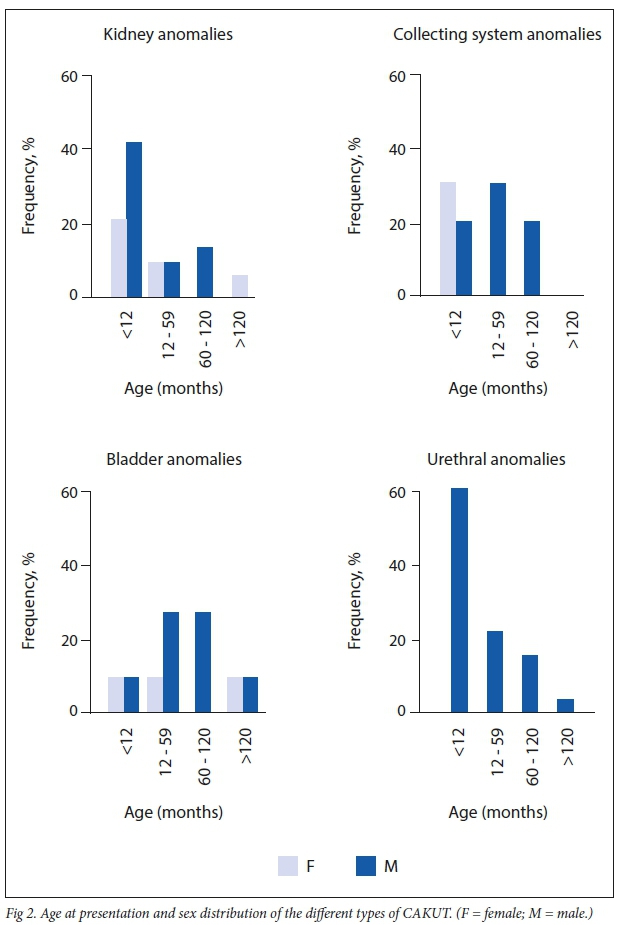
A detailed breakdown of the different types of CAKUT found in the study population is shown in Table 2. Fifty-seven percent (n=76/134) of the patients with CAKUT were <1 year old when they first presented to the clinic, and 21% (n=28/134) presented above the age of 5 years. Table 3 shows the age distribution of the different classes of CAKUT, and Fig. 2 summarises sex and age at presentation of the different types of CAKUT.

Discussion
CAKUT constitutes about 20 - 30% of all anomalies identified in the pre-natal period[2-4] and its reported prevalence among the general paediatric population ranges between 3.5 and 43%.[5,6]
The percentage (20%) of CAKUT in the present study falls within the range of results (3.5 - 43%) reported from other studies around the world.[5-7,16,17] The study that reported a prevalence rate of 43% was from a unit in Iraq; this was a case control study in a general paediatric setting where 128 children (64 with UTI, and 64 without UTI) were screened for CAKUT using abdominal ultrasound.[5] Other studies obtained their study populations from the general paediatric setting, including urology clinics, and prospectively screened all children who presented to hospital for CAKUT, and not only those with UTIs or renal pathologies.[5,6]
Although our study reflects the frequency of CAKUT in a select group ofpatients (i.e. those referred to a specialist paediatric nephrology clinic) in whom we could expect to find a higher percentage of CAKUT compared with the general paediatric population, there are a number of reasons that our results may nevertheless underestimate the true frequency of CAKUT in our population. Firstly, it is well recognised that some forms of CAKUT remain asymptomatic throughout life and may never be detected except through screening.[5,13,15] Our clinic sees only children who have been referred for a nephrology evaluation and it is likely that many children in the general paediatric population which our unit serves may have asymptomatic CAKUT and so would not have been diagnosed and referred for investigation. Secondly, patients with CAKUT who were seen primarily at the urology or paediatric surgery clinics at our hospital may not have been referred to us for follow-up, despite this being the protocol in place. Thirdly, some cases of CAKUT may not have had an ultrasound performed by our clinic, despite this being the protocol in place, and some of the routine abdominal ultrasounds that were performed during the study period may have missed some cases of CAKUT owing to technical error. Lastly, in our study, 159 different anomalies were documented for the 134 patients.
However, as part of our study protocol, we labelled any patient with >2 types of CAKUT as having only 1 type of CAKUT; this was based on the methodology used in a study reported from Egypt.[18] We chose the 'primary' CAKUT and ignored the extra anomaly which was assumed to have developed secondarily to the 'primary' CAKUT.
PUV was the most common type of CAKUT in our study. Most reports estimate the incidence of PUV to be in the range of 1:5 000 - 1:8 000 live births. However, estimates have varied as widely as 1:2 000 and 1:25 000 live births[19] In a study from Australia,[19] a live-birth incidence of 1.28 per 10 000 was reported in which 53% of cases were suspected on antenatal ultrasound and, of the remaining cases, 45% were detected in the neonatal period, with 50% of all postnatal cases presenting with UTI.
The frequency of PUV in our study was close to 45%, which is in keeping with findings from the study from Egypt where PUV was the most common (36.4%) among the 107 different types of CAKUT reviewed by Soliman et al.[18] In contrast, 2 other studies showed 'kidney anomalies' as being the leading type of CAKUT,[15,20] and a study from Iraq documented 'bladder anomalies' as the most common CAKUT.[5]
Differences in the classification of CAKUT, methodology and study design make it difficult to compare our study results with those of other studies. While Gupta et al.[13] used both children and adults as their study population, Bondagji reviewed only antenatally diagnosed CAKUT within a perinatal population.[20]
The reason for the high percentage of PUV in our study could be due to their tendency to present early with symptoms of obstructive uropathy and UTI, whereas patients with other forms of CAKUT, e.g duplex collecting system, are often asymptomatic and so may not be referred for investigation.[15]
Previous review articles on VUR suggest the general occurrence of VUR in healthy children to be 1 - 2%.[21-221 However, previous studies report a frequency of 0 - 30%.[231 Studies from developed countries have found high rates of VUR in the general paediatric population. [23-24]A study from Finland[23] reported a prevalence rate of 35% among 406 children with UTI, and a Canadian study1241 found a rate of 17.2% and 31% in a general paediatric population with normal kidneys and in children with UTI, respectively. The frequency of primary VUR in our study was 4.5%, which is in keeping with the 2 previous studies from SA.[25-26]
Male subjects were more likely to develop CAKUT than female, which is in keeping with previous studies from the developing world.[13,18,20,27-30]The male:female ratio in our study was 4.4:1 and gender was significantly associated with development of CAKUT (p<001), which highlights the need to have a high index of suspicion for CAKUT in every male child who presents with urinary symptoms.
The median (IQR) age at presentation in our study was 8.4 (1.9 - 47.7) months.This finding was of real concern as it reflects late presentation of many patients with CAKUT for investigation. Ideally, significant congenital anomalies should be diagnosed during the prenatal period and then followed up postnatally.
Comparing some forms of CAKUT in our study with those of other local SA studies, it is obvious that the differences in study duration, sources of data and antenatal screening protocols in the different research centres affected the numbers and ages at presentation of types of CAKUT documented.
Peterson et al reviewed 181 cases of PUV among boys <14 years old who presented to the CHBAH over a 29-year period. They found that 139 (77%) of the patients with PUV were diagnosed within the first year of life, whereas only 35 (58%) of our patients presented before 12 months' age. Our study population consisted only of patients who presented to the paediatric nephrology unit, while that of Peterson et al. included those who presented to both the general paediatric and urology units.
Ocheke et al.[32] documented 100 cases of pelvic ureteric junction (PUJ) obstruction over a 7-year period at the Red Cross War Memorial Children's Hospital, Cape Town, SA. The number of PUJ obstruction cases in their study is far higher than the 10 cases we recorded over 10 years; this can be explained by the fact that some of their study population were recruited from their urology unit. Again, 84% of their patients with PUJ obstruction were diagnosed within the first week of life, while only 60% of our patients with PUJ obstruction presented within the first year of life.
Leahy et al.[33] recorded 44 cases of prune belly syndrome (PBS) in their paediatric nephrology unit at the CHBAH. Eighty-six percent of the study population presented before 12 months of life; this figure is in contrast to our study where a much lower number of cases of PBS (4) was documented and only 1 of them presented to our unit before 1 year of age. Again, their study durations were over 30 years (1984 - 2014), which may have affected such an obvious discrepancy in study results.
In our setting, a combination of poor rates of routine antenatal screening, and late booking for antenatal care, resulted in few cases being referred as a result of detection by antenatal anomaly screening programmes. In addition, in some cases, even when a diagnosis had been made antenatally, parents still did not bring their children to hospital until they developed symptoms. In some extreme cases, some mothers delayed coming to the nephrology clinic even after being referred from the general paediatric clinics - which underscores the need for proper counselling of parents by the referring doctor about their child's illness.
Conclusion
The percentage of CAKUT in SA is high. PUV was the most common type of CAKUT in our cohort of patients and, as opposed to reports from developed countries, VUR made up a very small part of our cohort. This finding emphasises the importance of doing home-grown research on our own populations rather than relying on reports of other patient populations which may differ from our own.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Science.
Acknowledgements. The authors thank all nurses and staff of the Paediatric Nephrology Division of Charlotte Maxeke fohannesburg Academic Hospital, especially the ward clerk, for their support during data collection. Author contributions. NCO conceived and designed the manuscript, helped in data acquisition, analysis and interpretation of data, and also wrote the manuscript. AM contributed in the design and revision of the manuscript and gave final approval of the version to be published. CL helped with data acquisition and interpretation of the analysed data, edited the manuscript and gave final approval of the version to be published. TK helped with data acquisition and interpretation of the analysed data and gave final approval of the version to be published. CM helped with data acquisition and interpretation of the analysed data and gave final approval of the version to be published.
Funding. None.
Conflicts of interests. CL has received speaker fees from Roche Pharmaceuticals. The other authors have no conflict to declare.
References
1. Song R, Yosypiv IV. Genetics of congenital anomalies of the kidney and urinary tract. Pediatr Nephrol 2011;26(3):353-364. [ Links ]
2. Yosypiv IV. Congenital anomalies of the kidney and urinary tract: A genetic disorder? Int J Nephrol 2012: 909083. https://doi.org/10.1155%2F2012%2F909083 [ Links ]
3. Lewis MA, Shaw J, Sinha M, Adalat S, Hussain F, Inward C. UK Renal Registry 11th annual report (December 2008): Chapter 13, Demography of the UK paediatric renal replacement therapy population. Nephrol Clin Practice 2009;111( 1):257-267. [ Links ]
4. Queisser-Luft A, Stolz G, Wiessel A, Schlaefer K, Spranger J. Malformation in newborns: Results based on 30,940 infants and fetuses from the Mainz congenital birth defect monitoring system (19901998). Arch Gynecol Obstet 2002;266:163-167. [ Links ]
5. Alkhateeb NE, Al Azzawi S, Al Tawil NG. Association between UTI and urinary tract abnormalities: A case-control study in Erbil Ciy/ Iraq. J Pediatr Urol 2014;10:1165-1169. https://doi.org/10.1016/j.jpurol.2014.05.006 [ Links ]
6. Balat A, Hill LL. Genitourinary abnormalities in children with urinary tract infections. Turk J Med Sci 1999;29:59-63. [ Links ]
7. Nakai H, Asanuma H, Shishido S, Kitahara S, Yasuda K. Changing concepts in urological management of congenital anomalies of kidney and urinary tract, CAKUT. Pediatr Inti 2003;45(5):634-641. [ Links ]
8. Twaij M. Urinary tract infection in children: A review of its pathogenesis and risk factors. J R Soc Promot Health 2000;120(4):220-226. [ Links ]
9. Hamid F, Islam R, Paul N, Nusrat N, Parveen R. Urinary tract infection in children: A review Delta Med Col J 2013;l(2):51-57. [ Links ]
10. Schlager TA. Urinary tract infections in children younger than 5 years of age: Epidemiology, diagnosis, treatment, outcomes and prevention. Pediatr Drugs 2001;3:219. [ Links ]
11. Zelikovic I, Adeiman RD, Nancarrow PA. Urinary tract infection in children - an update. West J Med 1992;157:554-561. [ Links ]
12. Jodal U, Winberg J. Management of children with unobstructed urinary tract infection. Pediatr Nephrol 1987;1:647-656. [ Links ]
13. Gupta R, Memon A, Al-Khawari H, et al. The prevalence and pattern of congenital anomalies of the urinary tract detected by intravenous urography in Kuwait. Int Urol Nephrol 2002;34:477-483. [ Links ]
14. Seikaly MG, Ho PL, Emmett L, Fine RN, Tejani A. Chronic renal insufficiency in children: The 2001 Annual Report of the NAPRTCS. Pediatr Nephrol 2003;18(8):796-804. [ Links ]
15. Ring E, Zobel G. Urinary infection and malformation of urinary tract in infancy. Arch Dis Child 1988;63:818-820. [ Links ]
16. Caiulo VA, Caiulo S, Gargasole C, et al. Ultrasound mass screening for congenital anomalies of the kidney and urinary tract. Pediatr Nephrol 2012;27:949-953. [ Links ]
17. Berry CA, Channtler C. Urogenital malformations and disease. Br Med Bull 1986;42:181-186. [ Links ]
18. Soliman NA, Ali RI, Ghobrial EE, Habib EI, Ziada AM. Pattern of clinical presentation of congenital anomalies of the kidney and urinary tract among infants and children. Nephrology 2015;20:413-418. https://doi.org/10.1111/nep.12414 [ Links ]
19. Thakkar D, Deshpande AV, Kennedy SE. Epidemiology and demography of recently diagnosed cases of posterior urethral valves. Pediatr Res 2014;76(6):560-563. https://doi.org/10.1038/pr.2014.134 [ Links ]
20. Bondagji NS. Antenatal diagnosis, prevalence and outcome of congenital anomalies of the kidney and urinary tract in Saudi Arabia. Urol Ann 2014;6(1):36-40. https://doi.org/10.4103/0974-7796.127021 [ Links ]
21. Mak RH, Kuo HJ. Primary ureteral reflux: Emerging insights from molecular and genetic studies. Curr Opin Pediatr 2003;15(2):181-185. https://doi.org/10.1097/00008480-200304000-00007 [ Links ]
22. Eccles MR, Jacobs CH. The genetics of primary vesico-ureteric reflux. Am Acad Med Singapore 2000;29(3):337-345. [ Links ]
23. Venhola M, Hannula A, Huttunen NP, Renko M, Pokka T, Uhari M. Occurrence of VUR in children. Acta Pediatr 2010;99:1875-1878. https://doi.org/10.1111/j.1651-2227.2010.01909.x [ Links ]
24. Sergent M. What is the normal prevalence of vesicoureteral reflux? Pediatr Rad 2000;30(9):587-593. [ Links ]
25. Jeena P, Coovadia H, Adhikari MA. Probable association between urinary tract infection (UTI) and common disease of infancy and childhood: A hospital-based study of UTI in Durban, South Africa. J Trop Paediatr 1996;42:112-115. [ Links ]
26. Cremin B. Observations on vesico-ureteric reflux and intrarenal reflux: A review and survey of material. Clin Rad 1979;30:607-621. [ Links ]
27. Saxena SR, Laurence BM, Shaw DG. The justification for early radiological investigations of urinary tract infection in children. Lancet 1975;2(7931):403-404. [ Links ]
28. Bahna SL, Torp KH. The sex variable in childhood urinary tract infection. Acta Paediatr Scand 1975:64:581-586. [ Links ]
29. Barakat AJ, Drougas JG. Occurrence of congenital abnormalities of kidney and urinary tract in 13,775 autopsies. Urology 1991;38:347-350. [ Links ]
30. Saha A, Batra P, Chaturvedi P, Mehera B, Tayade A. Antenatal detection of renal malformations. Indian Pediatr 2009;46:346-348. [ Links ]
31. Peterson KL, Moore DP, Kala UK. Posterior urethral valves in South African boys: Outcome and challenges. S Afr Med J 2018;108(8):667-670. https://doi.org/10.7196/SAMJ.2018.v108i8.12934 [ Links ]
32. Ocheke IE, Antwi S, Gajjar P, McCulloch MI. Pelvi-ureteric junction obstruction at Red Cross Childrens Hospital, Cape Town: A 6-year review. Arab J Nephrol Transplant 2014;7(1):33-36. [ Links ]
33. Leahy SD, Kala U, Peterson KL. Prune belly syndrome: A South African perspective. Afr J Nephrol 2018;21(1):39-44. https://doi.org/10.21804/21-1-2957 [ Links ]
 Correspondence:
Correspondence:
N C Okoronkwo
nnekaceo@rocketmail.com
Accepted 20 May 2019


{kind=link}
{kind=link}