










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.14 no.1 Pretoria Abr. 2020
http://dx.doi.org/10.7196/SAJCH.2020.v14.i1.1621
RESEARCH
Children's ability to consent to medical management in South Africa
J van HeerdenI; R DelportII; M KrugerIII
IMMed (Paed), FCP Paed; Department of P aediatric Haematology and Oncology, Antwerp University Hospital, Belgium
IIPhD; Department of Family Medicine, Faculty of Medicine and Health Sciences, University of Pretoria, South Africa
IIIMMed (Paed), M Phil, PhD; Department of Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University and Tygerberg Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND. The South African Children's Act No. 38 of 2005 requires paediatric medical consent from 12 years of age.
OBJECTIVE. To determine children's ability to provide informed consent for medical treatment.
METHODS. Assessment used hypothetical treatment storyboards and structured interviews for assessment of 100 children (aged 10 -17 years), and 25 adult controls, using a standardised scoring tool to test understanding, ability to deliberate treatment choices, and provide rational reasons. Statistical analysis involved multivariate analyses of variance (MANOVAs) and analysis of variance (ANOVA).
RESULTS. The female:male ratios for children and adults were 1:0.92 and 1:0.98, respectively. Children >12 years were competent with regard to treatment choices (p<0.001), while 10-year-olds could deliberate reasonable outcomes, similar to adults (p<0.001). However, only children 12 years and older could provide rational reasons, where abstract concepts were not involved, whereas children who were >14 years old were able to provide rational reasons involving abstract concepts. The actual understanding of choices, compared with adults, was only observed in children older than 14 years (p<0.001). Gender was not a statistically significant denominator.
CONCLUSION. Children of 12 years and older are competent to make medical decisions, but the understanding of medical treatment choices under the age of 14 years is not clear.
Respect for persons is demonstrated in healthcare by obtaining patients' individual informed consent for any procedure or medical treatment.[1,2]
A person should therefore be able to understand the risks, deliberate the outcome, and provide rational reasons for his or her choice.[3] Research indicates that children older than 14 years have thought processes similar to those of adults.[1] In accordance with the United Nations Convention of the Rights of Children, assent for children's participation in decisionmaking processes is required on matters that relate to them.[4] While assent actively involves children in the decision-making process, it leaves the responsibility or the final decision up to parents or legal guardians, which ensures a level of protection for children as well as their parents.[5,6]
Many factors influence the choices that individuals make, including confidence in their own ability to choose.[7] The early stimulation of children to participate in decision-making reinforces this ability, while the process teaches them to reason through subject matter and to develop logical skills, which improves their autonomy.[8] If only their elders make decisions, it may negatively influence the development of maturity in children.[9-11] Westernised cultures promote decision-making by children as it facilitates a child's sense of confidence in his or her choices, whereas non-Westernised cultures may have strict hierarchical structures where elders make many of the community's decisions.[12,13]
There is a need to determine maturity or Gillick competence in children (established by the case of Gillick v West Norfolk and Wisbech Area Health Authority, 1986).[14] In the Gillick case, the court determined that the child had developed sufficient understanding to make an informed decision through age and life experience.[15] Currently, the Gillick principle is applied to determine children's maturity of cognitive development, as the differences in their evolving cognitive development may display immature decision-making, immature risk assessment, obstructive behaviour in adolescence, as well as unrealistic expectations or undue influence of peer pressure.[2]
Jean Piaget determined that children between the ages of 7 and 11 years were in the concrete operational stage, during which they acquire the concept of conservation, but cannot reason abstractly or test hypotheses systematically.[16] From the age of 11 years, children start to think abstractly, reason logically and draw conclusions from the information available, as well as apply these processes to hypothetical situations. Piaget and Kohlberg demonstrated that formal thinking only starts at an age of11 to 12 years and reaches equilibrium at 14 years, whereas Carol Gilligan established formal thinking to be present in late adolescence.[14] Many developmental psychologists believe that emotional, psychological and physical maturity may develop earlier ,and constant re-evaluation of children's competency is, therefore, required when making important decisions.[8]
There is no gold standard test to determine competency in children.[9,17] Children are particularly vulnerable in healthcare decision-making because they want to please parents, peers and medical staff, thereby basing decisions on perceived hopes rather than facts.[18,19] When dealing with children, the procedures should be explained to them in easily understandable language.[10] Readability of consent forms needs to be ensured not only with regard to the number of syllables in words, the length of sentences and the number of words in paragraphs, but also in terms of cultural context.[20] Weithorn and Campbell determined the competency of children in relation to healthcare decision-making in the USA, using a tool known as the Measure of Competency to Render Informed Treatment Decisions (MOC), and found that 14-year-old children do not differ from adults in their decision-making ability.[2]
According to the amendments to the South African Children's Act (Act No. 38 of 2005), children as young as 12 years have the right to consent to medical treatment.[21] They also have the right to request a termination of pregnancy according to the Choice on Termination of Pregnancy Act 92 of 1996 without parental consent.[22,23] To our knowledge, the competency of children from 12 years onwards to consent to medical procedures has not yet been investigated in South Africa (SA). The main objective of this pilot study was to determine whether children from 12 years of age onwards in SA were able to give informed consent to medical treatment as provided by legislation.
Objective
To determine the ability to provide informed consent for medical treatment in children from various age groups.
Methods
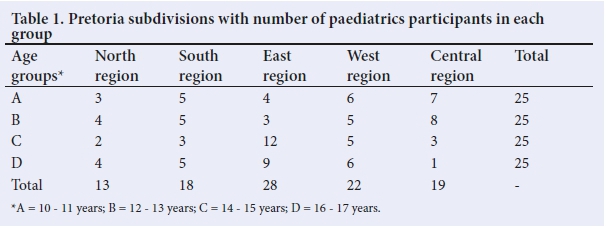
This was a prospective study, conducted between October 2008 and September 2009 with 100 participants, 10 years and older, from various socioeconomic backgrounds, randomly recruited from government schools by educators in five different regions of Pretoria, SA, together with 25 adult controls with a mean age of 41 (range 19 to 78) years (Table 1). Adults were randomly recruited from the same government schools to reflect similar backgrounds as the children. Children and adults were selected with the same mother tongue or first language as the interviewer to avoid suboptimal understanding of the treatment storyboards. Children and adults diagnosed, being treated or with a family member diagnosed with the same illness as the diseases in the hypothetical storyboards, were excluded from the study. The children were divided into four age groups comprising 25 participants each: 10 - 11 years (group A); 12 - 13 years (group B); 14 - 15 years (group C); and 16 - 17 years (Group D). Ethics approval was granted by The University of Pretoria Faculty of Health Sciences Research Ethics Committee. The Gauteng Department of Education provided permission to recruit children in public schools. Parents provided informed consent and children assent for participation.
The MO C, developed by Weithorn and Campbell, [2] was used as the study tool (with approval from Prof. Weithorn) for four hypothetical treatment dilemmas, namely diabetes, epilepsy, depression and enuresis, together with a structured interview questionnaire and scoring system. The treatment dilemmas, based on epilepsy, diabetes, enuresis and depression, focused on treatment or management alternatives. The tool was validated for language and comprehension, using two children in each age bracket, after adjustment to SA standards and current medical opinion, and involving the assistance of qualified paediatric subspecialists. Language complexity was adapted according to age level as determined during the validation process.
There were two types of questions for the Scale for Understanding (Scale 4): the first tested the participant's recall of facts, while the second tested the participant's appreciation of or inference about the subject matter. The participants earned points as follows: two points for full understanding; one point for partial understanding; and zero points for no understanding. A participant earned one point on the Scale for Evidence of Choice for choosing a treatment, while failing to choose a treatment would earn the participant no points. For the Scale for Reasonable Outcome (Scale 2), the judgments of 'reasonableness' by professional experts, comprising internationally 20 medical experts and 4 SA paediatricians, had been coded into a five-point rating scale, where a rating of 1 was 'completely unreasonable' and 5 was 'completely reasonable'.[2] Each option had to be rated independently, and mean scores were calculated for each age group and each treatment alternative. For the Scale for Rational Reasons (Scale 3), points could be earned for providing the correct answer to predetermined choices. Points were allocated for understanding the nature of the medical conditions, possible personal injury owing to the illnesses, the effects that a medical condition could have on the quality of life, and the influence on functionality. Furthermore, points could be earned for correctly interpreting the effect of medication on the medical condition and realising that medications might have side effects. Two of the investigators scored all the answers independently. The interviewer performed the first set of scoring during the interview and that was subsequently validated with the aid of audio transcripts. The answers were scored by a second scorer according to the transcripts.
Statistix 9.0 (Analytical Software, USA) was used to perform the statistical analysis. Variables were regarded as nominal and the Pearson correlation co-efficient employed to evaluate agreement between the two scorers by calculating Σ for all disease conditions. χ2 tests were used for heterogeneity or independence on all scales to determine agreement among choices. Scores for the scales of Reasonable Outcome, Rational Reasons, and Understanding were analysed with multivariate analyses of variance (MANOVAs) for each of the four dilemmas. Separate MANOVAs, 4 χ 2 (age χ sex) by three dependent variables (MOC scales), were performed. A comparison was made between groups through analysis of variance (ANOVA), using the adult group as the control group for Dunnett's multiple comparisons. The interscorer agreement was tested using the X test for heterogeneity.
Results
The study recruited 100 children and 25 adults, with an equal number of children in each age group. The female:male ratios for children and adults were 1:0.92 and 1:0.98, respectively (Table 2). The interscorer agreement ranged between 86% and 100% (Table 3), using the χtest for heterogeneity, an acceptable interscorer agreement.[2]
There were significant linear trends in the various storyboards among the age groups (p<0.005) as demonstrated by Scheffé's F-test, using Wilks' lambda for the four MANOVAs: diabetes, F=2.88; epilepsy, F=7.63; depression, F=7.76; and enuresis, F=4.93. The sex of the participants had no statistically significant influence (F=0.2 - 1.4), nor did the sex:age correlation (F=0.52 - 1.8). Only age of the participants was used as a significant variable in differences for further analysis.
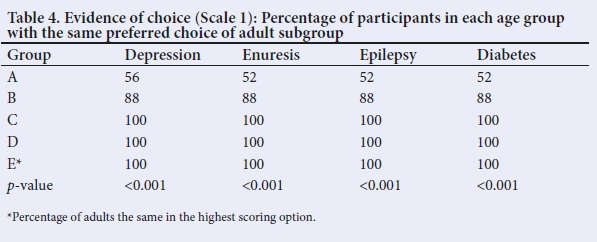
Scale for Evidence of Choice (Table 4)
All participants made a choice regarding a treatment preference. Only one child in the 10 - 11 year subgroup expressed a reluctance to make a decision. No age or sex difference applied in terms of the expression of a preference. There was a 52% correlation in the diabetes, enuresis and epilepsy storyboards, and a 56% correlation with adults in the depression storyboard regarding choice for the 10 - 11-year subgroup (p<0.001); 88% correlation for the 12 - 13-year subgroup (p<0.001); and 100% correlation for the older age groups (p<0.001). Children 12 years and older were therefore capable of making choices similar to those of adults.
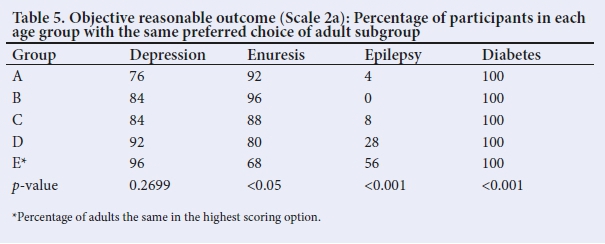
Scale for Reasonable Outcome (Table 5)
All participants chose insulin as the treatment option in the diabetes storyboard (100% correlation). There was a significant agreement between adults' and children's choices in the enuresis storyboard (p<0.05; ANOVA), but a significant difference between adults and children with regard to the treatment for epilepsy (p<0.001). The choice was between phenytoin, with visible hirsutism, versus sodium valproate, with potential liver damage. All the children's groups were in significant agreement regarding the treatment choice for epilepsy, choosing phenytoin (p<0.001). All age groups were in agreement (p<0.05) with their mean answers to the posed questions for depression, and the preferred depression treatment chosen was outpatient treatment, which differed from expert opinion (p<0.26; ANOVA). For the subjective scale (Table 6), all choices showed a statistically significant comparison (p<0.05 - p<0.001) in maturity to those of the adults in all storyboards. These results indicated a 100% agreement between children and adults regarding choice for the diabetes and depression storyboards, while all the children differed from the adults for epilepsy treatment, and only the 10 - 11-year subgroup differed in choice from the adults for enuresis treatment. A statistically significant linear trend was observed across the age groups in respect of the scale for objective reasonable outcome (p<0.001, using Scheffé's F-test for polynomial contrasts).
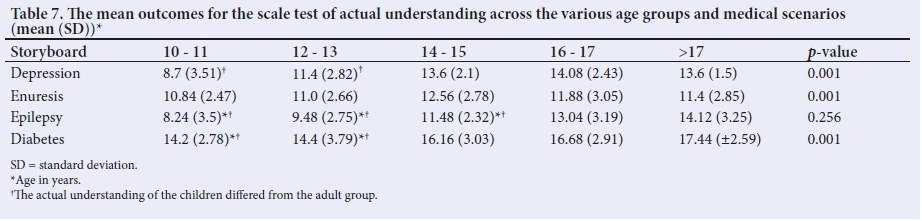
Scale for Understanding (Table 7)
All the children's groups, as well as the adults, had significantly similar understanding in the enuresis storyboard (p<0.001). However, understanding in the depression and diabetes storyboards for children under 13 years old differed significantly from the adults' understanding (p<0.001). All the children differed in their understanding from the adults in the epilepsy storyboard (p<0.001). Children under 13 years listed fewer factors (both physical and psychological aspects) and discussed the abstract elements of depression and diabetes to a lesser degree than adults. Significant linear trends were observed across the age groups (p<0.001, using the Scheffé's F-test for polynomial contrasts).
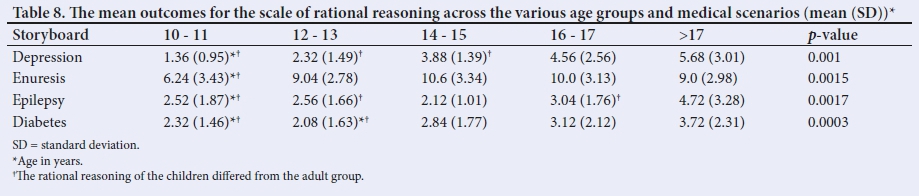
Scale for Rational Reasons (Table 8)
All the age groups differed significantly (p<0.001) from the adult group in the epilepsy storyboard. The children chose phenytoin, avoiding liver damage from sodium valproate. In the depression storyboard, all except the 16 - 17-year subgroup, differed from the adults for the depression storyboard (p<0.001) preferring home-based outpatient treatment rather than being hospitalised for depression. Both the 10 - 11- and 12 - 13-years age groups differed significantly from the adults (p<0.001) in the diabetes storyboard, while only the 10 - 11-year subgroup differed from the adults in the enuresis storyboard (p<0.001). In the diabetes storyboard, the younger children reasoned mainly in terms of physical discomfort, while excluding reasoning regarding psychological discomfort the way the older children and adults did. In the enuresis storyboard, the 10 - 11-year subgroup mainly discussed reasons for the bell and pad method, and to a degree for the use of medication, while the older age groups' reasoning included discussion about emotional distress that accompanies bedwetting.
Discussion
This study confirmed that children 12 years and older were capable of giving informed consent to medical procedures as they were able to choose a treatment, understand the information, deliberate the outcome, and provide rational reasons for their choice in concrete concepts. These findings are comparable with those of Weithorn and Campbell.[2] However, the present study proved that children possessed reasoning skills and actual understanding of complex abstract concepts, although not completely similar to those of adults. The study findings accordingly differ from those of Weithorn and Campbell. They found that children 12 - 13 years of age were unable to reason and understand at the same level as adults. As the Weithorn study was conducted in the late 1970s, one could postulate that the effects of globalisation and social media would have played a role in this current study.[24] Our study findings correspond with those of Flavell,[25] who argued that children of 12 - 14 years were adept at role assumption skills across a broad range of tasks and problems, and were capable of weighing up different options with mature decision-making. Grisso and Vierling'261 found that children aged 11 to 14 years were in a transition period with regard to the development of important cognitive abilities and perceptions of social expectations, and therefore suggested that independent consent by minors was justified if competence in individual children could be demonstrated.[25] Alderson reported that age was a relative concept in determining whether children could consent to procedures and that many other factors, for instance home environment, social circumstances, previous experience, the medical situation and the current age determinations of the law, played a greater role in determining competence.[26]
Of importance is the maturity of children concerning the choice for home-based care in the depression storyboard, which is not in agreement with adults and contradicts the recommendation, based upon evidence-based studies that proved a better outcome with home-based care, of the healthcare professionals.[27,28] A Cochrane review[29] stated that anxiety was markedly decreased with home-based care in low-risk diabetics. The children of all age groups further preferred a treatment option with a visible side-effect in the epilepsy storyboard rather than risk potential liver damage after long-term use; a finding in contrast with other studies, which reported that appearance was a major determinant of choices in treatment in adolescents.[30] Both positive and negative feedback from significant others are of great importance to adolescents owing to concerns over body image, physical attractiveness and social acceptance.[30,31] All of these factors affect children's decision-making.[30,31] This difference demonstrates that the study population has reasoning skills with maturity comparable to that of adults.
The difference in rational reasoning and actual understanding between the children's groups as well as with the adult group, does not influence the children's competence to participate in medical decision-making. This does, however, necessitate consent to be viewed in the context of factors guiding the decision-making process.[2]
Although the respondents did not suffer from chronic illnesses, a limitation to the study would be the effect of prior knowledge of medical treatment and of the diseases used in the storyboards, could influenc the responses provided by the respondents. Absence of previous acquaintance with the interviewer could also have affected responses.
Conclusion
In conclusion, children of 12 years and older are able to choose a treatment option and possess the necessary reasoning skills to deliberate their choice. However, only children >14 years possess actual understanding when dealing with more abstract concepts such as depression. Although this finding does correlate with the determinations of the SA law regarding decision-making, it is not clear whether the law is in keeping with the actual understanding of those choices. Our study indicates that the competency of children under the age of 14 years during emotionally complex decision-making is questionable which draws attention to the SA laws regarding the choice of termination of pregnancy. It stands to reason that basic choices regarding the administration of medicine and minor surgical interventions are in the abilities of decision-making for younger children, but that psychiatric treatments and interventions with severe consequences are outside the scope of younger children's abilities.
Declaration. None.
Acknowledgements. None.
Author contributions. JvH conducted the study, developed the protocol, conducted the interviews, collected and analysed the data, scored the answers, and wrote the manuscript. MK conceptualised and designed the study, supervised data analysis, independently scored the answers, and critically reviewed and revised the manuscript for important intellectual content. RD did the statistical analysis and critically reviewed the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Miller V, Drotar D, Kodish E. Children's competence for assent and consent: A review of empirical findings. Ethics Behaviour 2004;14(3):255-295. https://doi.org/10.1207/s15327019eb1403_3 [ Links ]
2. Weithorn L, Campbell S. The competency of children and adolescents to make informed treatment decisions. Child Dev 1982;53(6),1589-1598. [ Links ]
3. Hickey K. Minor's right in medical decision making. JONAS Healthc Law Ethics Regul 2007;9(3):100-104. https://doi.org/10.1097/01.NHL.0000287968.36429.a9 [ Links ]
4. Convention of the Rights of Children. www.unicef.org (accessed 15 June 2015). [ Links ]
5. Swartling U, Helgesson G, Hansen G, Ludvigsson J. Split views among parents regarding children's right to decide about participation in research: A questionnaire survey. J Med Ethics 2009;35(7):450-455. https://doi.org/10.1136/jme.2008.027383 [ Links ]
6. Unguru Y, Sill A, Kamani N. The experiences of children enrolled in pediatric oncology research: Implications for assent. Pediatrics 2010;125(4):876-883. https://doi.org/10.1542/peds.2008-3429 [ Links ]
7. Shafir E, Simonson I, Tversky A. Reason-based choice. Cognition 1993;49(1-2):11-36. [ Links ]
8. Mann L, Harmoni R, Power C. Adolescent decision-making: The development of competence. J Adolescence 1989;12(3):265-278. [ Links ]
9. Hein IM, Troost PW, Lindboom R, de Vries MC, Zwaan CM, Lindauer RJL. Assessing children's competence to consent in research by a standardized tool: A validity study. BMC Pediatrics 2012;12:156. https://doi.org/10.1186/1471-2431-12-156 [ Links ]
10. Jeremic V, Sénécal K, Borry P, Chokoshvili D, Vears D. Participation of children in medical decision-making: Challenges and potential solutions. J Bioeth Inq 2016;13(4),525-534. https://doi.org/10.1007/s11673-016-9747-8 [ Links ]
11. Ambuel B, Rappaport J. Developmental trends in adolescents' psychological and legal competence to consent to abortion. Law Hum Behaviour 1992;16(2):129-154. https://doi.org/10.1007/bf01044794 [ Links ]
12. Mazanec P, Tyler M. Cultural Considerations in end-of-life care: How ethnicity, age, and spirituality affect decisions when death is imminent. Am J Nursing 2003;103(3):50-58. https://doi.org/10.1097/00000446-200303000-00019 [ Links ]
13. Lindegger G, Richter L. HIV vaccine trials: Critical issues in informed consent. S Afr J Sci 2000;96(6):313-318. [ Links ]
14. Pierscionek B. Children, Gillick competency and consent for involvement in research. J Med Ethics 2007;33(11):659-665. [ Links ]
15. Battles H. Disclosure of an HIV diagnosis to children: History, current research, and future directions. J Dev Behav Pediatr 2007;28(2):155-166. https://doi.org/10.1097%2F01.DBP.0000267570.87564.cd [ Links ]
16. Power F, Higgins A, Kohlberg L. Lawrence Kohlberg's Approach to Moral Education. New York: Columbia University Press, 1989. [ Links ]
17. Hein IM, Troost PW, Broersma A, de Vries MC, Daams JG, Lindauer RJL. Why is it hard to make progress in assessing children's decision-making competence? BMC Med Ethics 2015;16:1. https://doi.org/10.1186/1472-6939-16-1 [ Links ]
18. Manning S. Finding a direction for pediatric assent. J Pediatrics 2007;150(4):38. https://doi.org/10.1016/j.jpeds.2006.12.035 [ Links ]
19. Kodish E. Informed consent for pediatric research: Is it really possible? J Pediatr 2003;142(2):89-90. https://doi.org/10.1067/mpd.2003.64 [ Links ]
20. Paasche-Orlow M, Taylor H, Brancati F. Readability standards for informed-consent forms as compared with actual readability. N Engl J Med 2003;348(8):721-726. https://doi.org/10.1056/NEJMsa021212 [ Links ]
21. South African Children's Bill of Rights 2008. www.justice.gov.za. (accessed 15 June 2015). [ Links ]
22. Choice on Termination of Pregnancy Act 92 of 1996. www.gov.za. (accessed 15 June 2015). [ Links ]
23. McQuoid-Mason D. The effect of the new Children's Act on consent to HIV testing and access to contraceptives by children. S Afr Med J 2007;97(12):1252-1253. [ Links ]
24. Mann L, Radford M, Kanagawa C. Cross-cultural differences in children's use of decision rules: A comparison between Japan and Australia. J Pers Soc Psychol 1985;49(6):1557-1564. [ Links ]
25. Flavell J. An analysis of cognitive-developmental sequences. Genet Psychol Monogr 1972; 86(2): 279-287. [ Links ]
26. Grisso T, Vierling L. Minors' consent to treatment: A developmental perspective. Prof Psychol 1978;9(3):412-427. [ Links ]
27. Marks I, Connolly J, Muijen M, Audini B, McNamee G, Lawrence G. Home-based versus hospital-based care for people with serious mental illness. Br J Psychiat 1994;165(2):179-194. [ Links ]
28. Hoagwood K, Burns B, Kiser L, Ringeisen H, Schoenwald S. Evidence-based practice in child and adolescent mental health services. Psychiatr Serv 2001;52(9):1179-1189. https://doi.org/10.1176/appi.ps.52.9.1179 [ Links ]
29. Clar C, Waugh N, Thomas S. Routine hospital admission versus out-patient or home care in children at diagnosis of type 1 diabetes mellitus. Cochrane Database Syst Rev 2007;2:CD004099. http://doi.org/10.1002/14651858.CD004099.pub2 [ Links ]
30. Lerner RM, Stuart A. Karabenick physical attractiveness, body attitudes, and self-concept in late adolescents. J Youth Adolesc 1974;3(4):307-316. [ Links ]
31. Lerner RM. Adolescent maturational changes and psychosocial development: A dynamic interactional perspective. J Youth Adolesc 1985;14(4):355-372. [ Links ]
 Correspondence:
Correspondence:
M Kruger
marianakruger@sun.ac.za
Accepted 3 October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}