










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.14 n.1 Pretoria Apr. 2020
http://dx.doi.org/10.7196.SAJCH.2020.v14.i1.1591
RESEARCH
Factors associated with preterm very low birthweight infant mortality at a tertiary hospital in Limpopo Province, South Africa
T S NtuliI, II; M P A MashegoIII; N ShipalanaIV; C SuttonV; M H K HameseVI
IPhD; Department of Public Health, University of Limpopo, Sovenga, South Africa
IIPhD; Department of Statistics and Operations Research, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IIIMB ChB, FCPaed (SA), MMed (Paed); Department of Paediatrics, University of Limpopo, Sovenga, South Africa
IVMB ChB, FCPaed (SA); Department of Paediatrics, University of Limpopo, Sovenga, South Africa
VMB ChB, FCPaed (SA); Department of Paediatrics, University of Limpopo, Sovenga, South Africa
VIMB ChB, FCPaed (SA);Department of Paediatrics, University of Limpopo, Sovenga, South Africa
ABSTRACT
BACKGROUND. Preterm very low birthweight (VLBW) infants remain a challenge worldwide. Local information on factors associated with mortality of VLBW infant is lacking.
OBJECTIVE. To identify the factors associated with the mortality of preterm VLBW infants at a tertiary hospital in Limpopo Province, South Africa.
METHODS. A retrospective study was undertaken between January and July 2015 at the neonatal intensive care unit (NICU). The medical records of mothers and their babies were retrieved and reviewed. Maternal data used were age, parity, use of antenatal corticosteroids, HIV status, mode of delivery and maternal morbidity. Neonatal data included gender, birthweight, gestational age, Apgar score, resuscitation in delivery, length of stay in NICU, morbidity and treatment. Data obtained were analysed using STATA version 10.0.
RESULTS. A total of 252 preterm VLBW infant-and-mother pairs were included in the study. The VLBW infant survival rate was 77.4%. Use of antenatal corticosteroids, spontaneous preterm labour, birthweight and gestational age, Apgar score <6 at 1 minute, resuscitation in delivery room, length of stay in the NICU, prematurity-related problems, sepsis, pulmonary haemorrhage, hypothermia, jaundice, and nasal continuous positive airway pressure (NCPAP) with surfactant and mechanical ventilation with or without surfactant were significantly associated with infants' outcomes.
CONCLUSION. The survival rate of preterm VLBW infants in this rural tertiary hospital was relatively high but could be further increased by prompt administration of surfactant and mechanical ventilation with or without surfactant.
Neonatal mortality remains a public health challenge worldwide, particularly in sub-Saharan Africa.[1-3] Preterm birth (<37 weeks' gestational age) is the main cause of neonatal mortality.[4] Infants born prematurely with very low birthweight (VLBW) (<1 500 g) usually require some form of respiratory support and long periods of hospitalisation.[5] The use of nasal continuous positive airway pressure (NCPAP) with or without surfactant has been shown to improve infant survival,[6-8] while the use of surfactant,[9] and ventilation with or without surfactant, increased infant mortality, possibly indicating more severe respiratory illness.[10,11] However, prompt administration of surfactant, and mechanical ventilation with or without surfactant, reduces infant morbidity and mortality.'121 Moreover, numerous studies have shown that the use of antenatal corticosteroids has significant benefits,[8,13-15] although some authors found that giving steroids to the mother did not have any influence on neonatal survival.[16]
Risk factors associated with VLBW infants have been widely researched, and research results have provided good preventative strategies which have improved infant survival rates.[8,9,14,17-21] The survival of VLBW infants was reported to be over 70% in a quaternary hospital in Johannesburg, South Africa (SA),[8] but ranged between 40% and 60% in Nigeria[22] and Malawi,'[23] while survival rates of more than 80% in developed countries have been encountered.[24,25] Although the risk factors associated with VLBW infant survival and morbidity have been extensively documented, including in SA, no data exist for this under-resourced subject in SA. Consequently, the present study aimed to determine factors relevant to our population which could be used to direct resources, intervention programnes and further research.
Method
This was a retrospective descriptive study based on a review of the medical records of VLBW premature infants admitted to the Neonatal Intensive Care Unit (NCU) of Mankweng Hospital, the only tertiary referral hospital in the Limpopo Province of SA. The data for this study were collected over a period of 7 months from January to July 2015. Ethics approval to conduct the study was obtained from the University of Limpopo Ethics Committee (ref. no. TREC/84/2016:PG), and anonymity and confidentiality of personal patient information was protected by using their identity numbers. The NICU is a 60-bed unit with 9 beds each for intensive care and high care, a nursery with 30 beds, and 12 kangaroo mother care beds. The unit has a total admission of 2 000 patients per annum.
Neonates were managed according to standard unit protocols by a neonatologist, general paediatrician, medical officer and paediatric registrars. All VLBW infants weighing <1 000 g with respiratory distress are not put on mechanical ventilation but on supplemental oxygen via a low-flow nasal cannula (NPO2) using either SiPAP or NCPAP. As a rescue treatment, surfactant therapy is given to all VLBW infants weighing >800 g or >26 weeks' gestational age (GA). Otherwise, all infants irrespective of birthweight receive resuscitation, warmth, intravenous antibiotics, supplemental oxygen and phototherapy. Cranial ultrasound is performed per availability of a sonographer and if intraventricular haemorrhage is clinically suspected. Screening for retinopathy of prematurity (ROP) is performed within 4 - 6 weeks' chronological age or <32 weeks' gestational age.
A minimum sample size of 246 was calculated based on a 95% confidence level, 5% sampling error and assuming a survival rate >80% (we excluded deaths in the delivery room) of VLBW infants admitted to the NCU.'81 A consecutive sample of VLBW infant pairs with their mothers was selected for the study. Data were collected using a data collection form designed for the study. The NICU register was used as the starting point to collate a list of infants admitted during the study period, after which the relevant medical records were retrieved. Using the register and patient files, the following maternal data were collected: age, parity, use of antenatal corticosteroids, HIV status, mode of delivery and maternal morbidity, while infant data included gender, birthweight (BW), GA, Apgar score, resuscitation at delivery, length of stay in the NICU, morbidity and invasive ventilation with or without surfactant, and NCPAP with or without surfactant.
Statistical analyses were performed using the statistical programme STATA version 10.0 (StataCorp., USA). Comparisons between survivors and non-survivors were performed using the Student i-test and χ2tests for continuous and categorical data, respectively. A p-value <0.05 was considered statistically significant.
Results
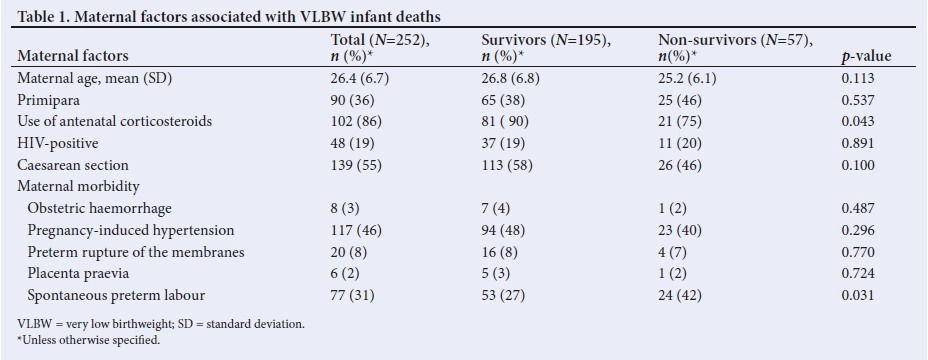
A total of 1 273 babies were admitted to the NCU during the period of the study. Of these, 19.8% (n=252) were VLBW infants, of whom 77.4% (n=195/252) survived. The maternal factors associated with neonatal mortality are shown in Table 1. The mean (standard deviation) age of mothers in the survivor group was similar to that of mothers in the non-survivor group (26.8 (6.8) years v. 25.2 (6.1) years, p>0.05). Mothers of the survivor group tended to be delivered by caesarean section more frequently than those in the non-survivor group; however, the finding was not statistically significant (58% v. 46%, p>0.05). A total of 118 mothers had information on administration of antenatal steroids, of whom 86% (n=102) received steroids. Of these, a significantly greater proportion of mothers in the survivor group received antenatal steroids than those in the non-survivor group (90% v. 75%, p<0.05). Mothers of non-survivor VLBW infants (42%) were more likely to have experienced spontaneous preterm labour than mothers of the survivor group (27%) (p<0.05). Only one mother was diagnosed with chorioamnionitis; her baby died. Other factors examined for an association with VLBW infant mortality included parity, HIV status, obstetric haemorrhage, pregnancy-induced hypertension (PIH), preterm rupture of the membranes, and placenta praevia; however, the results were not significant.
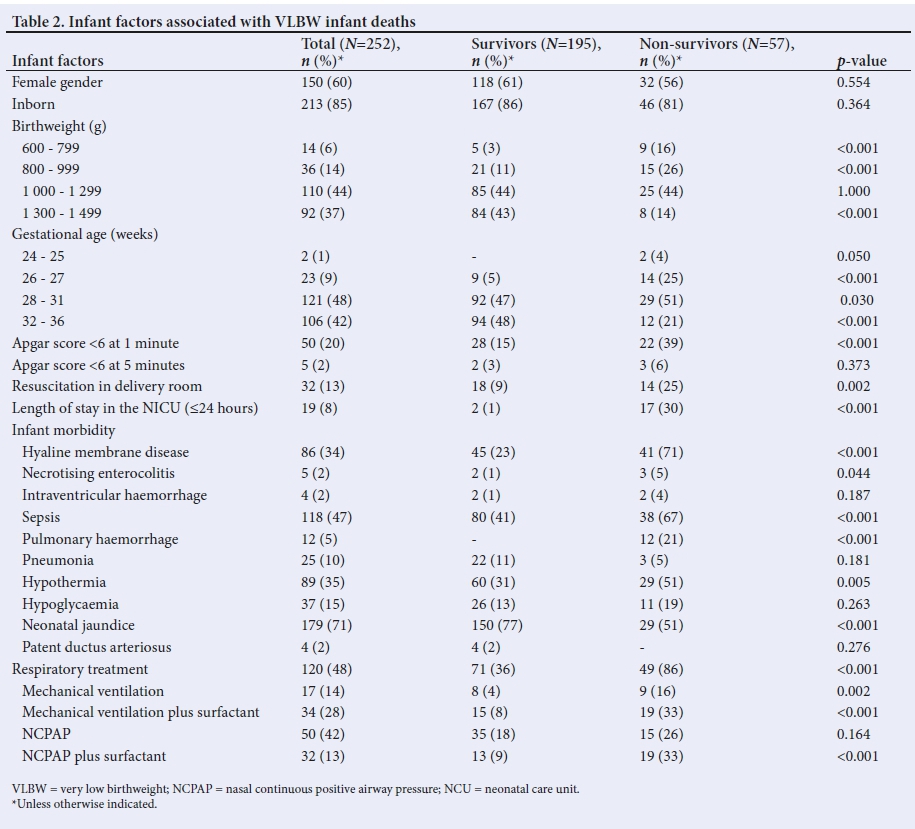
The characteristics of the VLBW infant-survivor and non-survivor groups are compared in Table 2. VLBW infants in the non-survivor group were significantly more likely to have a GA <31 weeks, birthweight <1 000 g and an Apgar score <6 at 1 minute (p<0.05). Efforts to resuscitate neonates in the delivery room were more common among the non-survivors than the survivors (25% v. 9%, p<0.05). VLBW infants in the non-survivor group were significantly more likely to have sepsis, hyaline membrane disease, pulmonary haemorrhage, hypothermia and necrotising enterocolitis than those in the survivor group (p<0.05). However, neonatal jaundice was significantly lower in the non-survivor group than in the survivor groups (51% v. 77%, p<0.05). Regarding clinical intervention, a significantly higher proportion of non-survivors were on mechanical ventilation without surfactant (16% v. 4%, p<0.05), and mechanical ventilation with surfactant (33% v. 8%, p<0.05), than were survivors. NCPAP was more likely to be given to non-survivors than survivors, which was statistically significant among those with surfactant.
Discussion
Our study found a VLBW infant survival rate of 77%, which is comparable to a survival rate of 75% reported in an urban academic hospital in SA,[8] as well as being higher than the survival rates, ranging between 40% and 60%, found in teaching hospitals in Nigeria[22] and Malawi.[23] Our survival rate is lower than the 80% reported for VLBW infants admitted to NICUs in developed countries.[24,25] Some of the differences in infant survival rates may be related to quality of care, availability of workforce and equipment; however, in our study, the high survival rate could be due to exclusion of deaths in the delivery room.[8] The use of antenatal corticosteroids has been shown to improve infant survival,[8,13-15] although this has not been shown in all studies.[16]
In this study, it was difficult to make meaningful comparisons on the use of antenatal steroids owing to incomplete data for the mother.
However, among mothers for whom information on administration of antenatal steroids was recorded (n=118), most (86%, n=102) received steroids and this practice was found to be significantly higher among mothers of infants in survivor groups than in non-survivor groups. The findings of our study illustrate that maternal age has no significant relationship with VLBW infant mortality, which is consistent with some previous studies.[17,21] However, this finding is in contrast to other studies which found a high risk of VLBW infant mortality among young mothers.[9,26] The use of caesarean section as a delivery mode was found to be associated with lower rates of infant morbidity and mortality.[21,26] However, similarly to other studies,[16,18 our findings show no statistically significant relationship between caesarean delivery and the outcomes of VLBW infants. The reason for this is unclear and needs further investigation.
PIH is one of the leading causes of maternal[27] and neonatal[19] mortality and morbidity. Early detection and correct management of hypertension remains a challenge in most healthcare facilities in developing countries. A meta-analysis of 55 studies from 25 countries confirmed that PIH is related to adverse pregnancy outcomes.[20] In contrast, in our study, PIH did not have any
significant influence on VLBW infant deaths; the reasons are not documented in our study, however. Although we did not assess whether babies were growth-restricted or not, women with PIH are more likely to deliver growth-restricted babies whose lungs are more mature.[28] In 2010, Blencowe et al.l29]found that spontaneous preterm birth is an issue in sub-Saharan Africa. In this study, spontaneous preterm labour was significantly higher in the mothers of non-survivors than in the mothers of survivors. The possible causes of spontaneous preterm labour were not documented in our study, but maternal infection,[30,31] mother's psychological stress[32-34] and social well-being,[35] and lack of antenatal care[36] are linked to preterm labour.
With regard to neonate risk factors, few (n=32) VLBW infants in our study were resuscitated in the delivery room. Those who were resuscitated during delivery had a higher mortality, which might reflect the severity of infant illness and/or lack of skills of attending healthcare workers. In line with other studies,[17,18] our findings show that 1-minute Apgar scores <6 were significantly associated with greater risk of VLBW infant mortality. In contrast, other studies have found that a low 5-minute Apgar score significantly influences VLBW infant mortality.[16] GA and birthweight have been found to be inversely associated with VLBW infant mortality,[17,21,26] but the methods used to define GA compromise its general use.[4] In our study, GA and birthweight were significantly lower in non-survivors than in survivors, which is consistent with previous studies.[8,14]
Most NICUs have different intervention criteria for their levels of care, owing to limited resources such as surfactant replacement therapy, NCPAP and mechanical ventilation, which have helped to improve the survival of immature babies.[6-12] In our study, more than half of the VLBW infants received NCPAP with or without surfactant, and mortality was higher in those receiving surfactant; however, mechanical ventilation with or without surfactant increased mortality, which is in line with other studies;'10,111 this could be because most infants required prolonged resuscitation in the delivery room, suggesting severe birth asphyxia and, in some cases, surfactant administration may have been delayed, and/or ventilation may have been delayed or prolonged.[37] In our study, 30% of the non-survivor infants died within 24 hours of NICU admission, which is higher than the rate of 9.4% in Brazil.[9] The earlier infant deaths in our study could relate to a number of factors, such as delay in seeking medical attention during labour, infrequent visits to antenatal clinics, no accessible intensive care unit bed with ventilator, and inadequate resuscitation equipment.[38]
Neonatal jaundice remains a concern worldwide. It is not surprising, then, in accordance with studies in low- and middle-income countries,[39,40] that jaundice was the main cause of neonatal morbidity and was significantly higher in the survivor group than in the non-survivor group. This tendency is because more survivors lived long enough to exhibit jaundice, which is common among premature babies owing to their physiological immaturity.[39] Interestingly, similarly to other studies,[9,41,42] hypothermia was found to be a common predictor of neonatal fatality, and has been shown to increase the risk of neonatal morbidity and mortality worldwide. A large proportion (38%) of the hypothermia cases in our study occurred in winter, which indicates a lack of thermal protection.[22,43]
Limitations
The above findings must be considered in the context of the following limitations. The study was limited to a 7-month period; a longer study period might have resulted in either a higher or lower survival rate than was established. As with retrospective studies, any missing data from patient files affect the reliability of the data. There was some incompleteness of notes regarding the mothers' pregnancy and data on the infants: maternal antenatal care visits, duration of resuscitation post delivery, postnatal age and duration of mechanical ventilation. Furthermore, it was difficult to determine whether maternal morbidities in our study contributed to spontaneous preterm labour. Another limitation is that the study was based on results from one referral centre which are therefore not generalisable.
Conclusion
The survival rate of VLBW infants in Mankweng Hospital, a rural tertiary hospital in Limpopo Province, SA, was relatively high but could be further increased by prompt administration of surfactant and mechanical ventilation with or without surfactant.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgments. We thank the records clerks and information officers of Mankweng Hospital for their assistance during the fieldwork.
Author contributions. TS analysed and interpreted data and prepared the manuscript. MPA, NC and MHK prepared the data collection instrument, collected data, interpreted data and reviewed the manuscript. All authors read and approved the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Oza S, Cousens SN, Lawn JE. Estimation of daily risk of neonatal death, including the day of birth, in 186 countries in 2013: A vital-registration and modelling-based study. Lancet Glob Health 2014;2(11):e635-644. https://doi.org/10.1016/S2214-109X(14)70309-2 [ Links ]
2. Wang H, Naghavi M, Allen C, Barber RM. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1459-1544. https://doi.org/10.1016/S0140-6736(16)31012-1 [ Links ]
3. Lehtonen L, Gimeno A, Parra-Llorca A, Vento M. Early neonatal death: A challenge worldwide. Semin Fetal Neonatal Med 2017;22(3):153-160. https://doi.org/10.1016/j.siny.2017.02.006 [ Links ]
4. Velaphi SC, Rhoda N. Reducing neonatal deaths in South Africa - are we there yet and what can be done? S Afr J Child Health 2012;6(3):67-71. [ Links ]
5. Dunn MS, Kaempf J, de Klerk A, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011;128:e1069-e1076. https://doi.org/10.1542/peds.2010-3848 [ Links ]
6. Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev 2012,11:CD001456. [ Links ]
7. Bopape-Chinyanga T, Thomas R, Velaphi S. Outcome of very low birth weight babies managed with nasal continuous positive airway pressure, with or without surfactant, in a high care nursery. S Afr J Child Health 2016;10(4):199. https://doi.org/10.7196%2FSAJCH.2016.v10i4.1096 [ Links ]
8. Ballot DE, Chirwa T, Ramdin T, et al. Comparison of morbidity and mortality of very low birthweight infants in a central hospital in Johannesburg between 2006/2007 and 2013. BMC Pediatr 2015;15:20. https://doi.org/10.1186/s12887-015-0337-4 [ Links ]
9. Castro EC, Leite AJ, Almeida MF, Guinsburg R. Perinatal factors associated with early neonatal deaths in very low birth weight preterm infants in Northeast Brazil. BMC Pediatrics 2014;14:312. https://doi.org/10.1186/s12887-014-0312-5 [ Links ]
10. Afjeh SA, Sabzehei MK, Fallahi M, Esmaili F. Outcome of very low birthweight infants over 3 years Report from an Iranian center. Iran J Pediatr 2013;23(5):579-587. [ Links ]
11. Iqbal Q, Younus MM, Ahmed A, et al. Neonatal mechanical ventilation: Indications and outcome. Ind J Crit Care Med 2015;19(9):523-527. https://doi.org/10.4103%2F0972-5229.164800 [ Links ]
12. Sweet DG, Carnielli V, Greisen G, et al. European consensus guidelines on the management of neonatal respiratory distress syndrome in preterm infants -2010 update. Neonatology 2010;97(4):402-417. [ Links ]
13. Chi CC, Wang SH, Wojnarowska F, Kirtschig G, Davies E, Bennett C. Safety of topical corticosteroids in pregnancy. Cochrane Database Syst Rev 2015;26(10):CD007346. https://doi.org/10.1002/14651858.CD007346.pub3 [ Links ]
14. Lim JW, Chung SH, Kang DR, Kim CR. Risk factors for cause-specific mortality of very-low-birth-weight infants in the Korean Neonatal Network. J Korean Med Sci 2015;30 Suppl 1:S35-S44. https://doi.org/10.3346/jkms.2015.30.S1.S35 [ Links ]
15. Simhan HN. Practice Bulletin No. 171: Management of preterm labor. Obstet Gynecol 2016;128(4):e155-e164. https://doi.org/10.1097/AOG.0000000000001711 [ Links ]
16. Ghorbani F, Heidarzadeh M, Dastgiri S, Ghazi M, Rahkar Farshi M. Survival of premature and low birth weight infants: A multicenter, prospective, cohort study in Iran. Iranian J Neonatol 2017:8(1). https://doi.org/10.22038/ijn.2017.17586.1203 [ Links ]
17. Carneiro JA, Vieira MM, Reis TC, Caldeira AP. Risk factors for mortality of very low birth weight newborns at a neonatal intensive care unit. Rev Paul Pediatr 2012;30(3):369-376. [ Links ]
18. Nayeri F, Dalili H, Nili F, et al. Risk factors for neonatal mortality among very low birth weight neonates. Acta Medica Iranica 2013;51:5. [ Links ]
19. Ghojazadeh M, Velayati A, Mallah F, et al. Contributing death factors in very low-birth-weight infants by path method analysis. Niger Med J 2014;55(5):389-393. https://doi.org/10.4103/0300-1652.140378 [ Links ]
20. Bramham K, Parnell B, Nelson-Piercy C, Seed PT, Poston L, Chappell LC. Chronic hypertension and pregnancy outcomes: Systematic review and meta-analysis. BMJ 2014;348:g2301. https://doi.org/10.1136/bmj.g2301 [ Links ]
21. Zile I, Ebela I, Rozenfelde IR. Risk factors associated with neonatal deaths among very low birth weight infants in Latvia. Curr Pediatr Res 2017;21(1):64-68. [ Links ]
22. Onalo R, Olateju EK. A four-year retrospective review of very low birth weight babies seen at the University of Abuja Teaching Hospital, Abuja, Nigeria. Niger Postgrad Med J 2015;22(2):93-99. [ Links ]
23. Rylance S, Ward J. Early mortality of very low-birthweight infants at Queen Elizabeth Central Hospital, Malawi. Paediatr Int Child Health 2013;33(2):91-96. https://doi.org/10.1179/2046905513Y.0000000053 [ Links ]
24. Horbar JD, Carpenter JH, Badger GJ, et al. Mortality and neonatal morbidity among infants 501 to 1500 grams from 2000 to 2009. Pediatrics 2012;129(6):1019-1026. https://doi.org/10.1542/peds.2011-3028 [ Links ]
25. Shim JW, Jin HS, Bae CW. Changes in survival rate for very-low-birth-weight infants in Korea: Comparison with other countries. J Korean Med Sci 2015;30 Suppl 1:S25-S34. https://doi.org/10.3346/jkms.2015.30.S1.S25 [ Links ]
26. Fernandez R, DApremont I, Domínguez A, Tapia JL, Red Neonatal Neocosur. Survival and morbidity of very low birth weight infant in a South American neonatal network. Arch Argent Pediatr 2014;112(5):405-412. https://doi.org/10.1590/S0325-00752014000500004 [ Links ]
27. Lo JO, Mission JF, Caughey AB. Hypertensive disease of pregnancy and maternal mortality. Curr Opin Obstet Gynecol 2013;25(2):124-132. https://doi.org/10.1097/GCO.0b013e32835e0ef5 [ Links ]
28. Shah DM, Shenai JP, Vaughn WK. Neonatal outcome of premature infants of mothers with preeclampsia. J Perinatol 1995;15(4):264-267. [ Links ]
29. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012;9;379(9832):2162-2172. https://doi.org/10.1016/S0140-6736(12)60820-4 [ Links ]
30. Galinsky R, Polglase GR, Hooper SB, Black MJ, Moss TJ. The consequences of chorioamnionitis: Preterm birth and effects on development. J Pregnancy 2013;2013:412831. https://doi.org/10.1155/2013/412831 [ Links ]
31. Xiao PL, Zhou YB, Chen Y, et al. Association between maternal HIV infection and low birth weight and prematurity: A meta-analysis of cohort studies. BMC Pregnancy Childbirth 2015;8;15:246. https://doi.org/10.1186/s12884-015-0684-z [ Links ]
32. Quispel C, Bangma M, Kazemier BM, et al. The role of depressive symptoms in the pathway of demographic and psychosocial risks to preterm birth and small for gestational age. Midwifery 2014;30(8):919-925. https://doi.org/10.1016/j.midw.2014.03.008 [ Links ]
33. Lilliecreutz C, Larén J, Sydsjö G, Josefsson A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth 2016;16:5. https://doi.org/10.1186/s12884-015-0775-x [ Links ]
34. Shapiro GD, Fraser WD, Frasch MG, Séguin JR. Psychosocial stress in pregnancy and preterm birth: Associations and mechanisms. J Perinat Med 2013;41(6):631-645. https://doi.org/10.1515/jpm-2012-0295 [ Links ]
35. Oftedal AM, Busterud K, Irgens LM, Haug K, Rasmussen S. Socio-economic risk factors for preterm birth in Norway 1999-2009. Scand J Public Health 2016;44(6):587-592. https://doi.org/10.1177/1403494816653288 [ Links ]
36. Shah R, Mullany LC, Darmstadt GL, et al. Incidence and risk factors of preterm birth in a rural Bangladeshi cohort. BMC Pediatr 2014;24;14:112. https://doi.org/10.1186/1471-2431-14-112 [ Links ]
37. Choi YB, Lee J, Park J, Jun YH. Impact of prolonged mechanical ventilation in very low birth weight infants: Results From a national cohort study. J Pediatr 2018;194:34-39.e3. https://doi.org/10.1016/j.jpeds.2017.10.042 [ Links ]
38. Lloyd LG, de Witt TW. Neonatal mortality in South Africa: How are we doing and can we do better? S Afr Med J 2013;2;103(8):518-519. https://doi.org/10.7196/samj.7200 [ Links ]
39. Bhutani VK, Wong RJ. Bilirubin neurotoxicity in preterm infants: Risk and prevention. J Clin Neonatol 2013;2(2):61-69. https://doi.org/10.4103/2249-4847.116402 [ Links ]
40. Greco C, Arnolda G, Boo NY, et al. Neonatal jaundice in low- and middle-income countries: Lessons and future directions from the 2015 Don Ostrow Trieste Yellow Retreat. Neonatology 2016;110(3):172-180. https://doi.org/10.1159/000445708 [ Links ]
41. Boo NY, Guat-Sim, Cheah I. Malaysian National Neonatal Registry. Admission hypothermia among VLBW infants in Malaysian NICUs. J Trop Pediatr 2013;59(6):447-452. https://doi.org/10.1093/tropej/fmt051 [ Links ]
42. De Almeida MF, Guinsburg R, Sancho GA, et al. Hypothermia and early neonatal mortality in preterm infants. J Pediatr 2014;164(2):271-275.e1. https://doi.org/10.1016/j.jpeds.2013.09.049 [ Links ]
43. Lunze K, Bloom DE, Jamison DT, Hamer DH. The global burden of neonatal hypothermia: Systematic review of a major challenge for newborn survival. BMC Med 2013; 31;11:24. https://doi.org/10.1186/1741-7015-11-24 [ Links ]
 Correspondence:
Correspondence:
T S Ntuli
tsntuli@hotmail.co
Accepted 4 April 2019


{kind=link}
{kind=link}