










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.14 no.1 Pretoria Abr. 2020
http://dx.doi.org/SAJCH.2020.v14.i1.1516
RESEARCH
A descriptive study of children with cerebral palsy at Chris Hani Baragwanath Academic Hospital
N MahlabaI; F L NakwaII; J R RoddaIII
IMB ChB, MMed (Paeds), FCPaed; Department of Paediatrics, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, FCPaed, MMEd (Paeds), Cert Neonatol (SA), Cert Paed Neurol (SA); Department of Paediatrics, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB BCh, FCPaed, Dipl Theol Department of Paediatrics, Chris Hani Baragwanath Academic Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Cerebral palsy (CP) is a motor disability owing to a non-progressive insult to the developing motor brain. To contribute to the paucity of CP data in South Africa, we undertook a retrospective study to describe new cases of CP presenting at the CP clinic at Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg.
OBJECTIVE. To determine the age at presentation, the common types of CP that are seen at the clinic, and imaging abnormalities detected; and to assess the level of functional capabilities of patients using the Gross Motor Function Classification Scale (GMFCS). We assessed the association between the GMFCS level of patients with the type of imaging abnormalities, type of CP, gestational age, and comorbidities.
METHODS. All CP patients who presented for the first time to the CP clinic in 2012 were screened for enrolment. A total of 145 patients from the 201 new cases of CP presenting to the CP clinic during the study period were included in the study. Demographic data, radiology reports of imaging abnormalities (if imaging had been performed), GMFCS scores and perinatal history were extracted from the clinical files.
RESULTS. The mean (standard deviation) age at presentation of the patients was 34.7 (35) months. Two-thirds of the patients were male. Forty-eight percent of CP patients were diagnosed with neonatal encephalopathy. Mixed CP (39%) was the predominant type of CP. Cranial ultrasound, computed tomography (CT) scanning and magnetic resonance imaging (MRI) of the brain were performed in 60% of the patients. These scanned patients (54%) had periventricular white matter lesions (PWML). More than a third of cases had a level III GMFCS score. Intellectual impairment was the most frequent comorbidity.
CONCLUSION. In our cohort of patients, PWML were frequently reported on imaging results, DGML (deep grey matter lesions) were infrequently described, and some patients had normal imaging reports. Most of our patients functioned at GMFCS level III with a higher GMFCS level correlating with the type of CP, intellectual impairment and orthopaedic complications. Most CP patients had been diagnosed with neonatal encephalopathy. This information will aid in the management of patients with CP at CHBAH.
Cerebral palsy (CP) is predominantly a motor disability that is caused by a non-progressive insult to the developing motor brain. CP describes a group of permanent disorders of the development of movement and posture, causing activity limitations that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of CP are often accompanied by disturbances of sensation, perception, cognition, communication, and behaviour; by epilepsy; and secondary musculoskeletal problems.[1]
CP is the most common motor disability during childhood. The prevalence estimates of CP have been reported to range from 1.5 to more than 4 per 1 000 live births, in both developing and developed countries.[2] The Surveillance of Cerebral Palsy in Europe (SCPE) network reported a prevalence rate across 12 centres in Europe of 1.5 - 3 per 1 000 live births.[31 Currently, there is no established national registry of children living with CP in South Africa (SA). Two SA studies have indicated that the prevalence rates may be as high as 1.0 - 8.0 percent.[5]
Van Toorn et al.[6]reviewed 240 records of children with CP at Tygerberg Children's Hospital in Cape Town, SA, investigating the aetiology of CP in these patients. They found that the origin of insults occurred predominantly in the perinatal or neonatal period in 38% of cases. Cerebral malformations (15.7%) and stroke (5.7%) were the most frequent antenatal causes, while birth asphyxia (17.3%), encephalopathy of prematurity (17.7%) and kernicterus (2%) were the most frequent perinatal causes.
In order to contribute to the paucity of CP data in SA, we undertook a retrospective study between 1 January 2012 and 31 December 2012 to describe new cases of CP presenting at the CP clinic at Chris Hani Baragwanath Academic Hospital (CHBAH) in Soweto, Johannesburg. The aim of our study was to determine the demographics of patients referred to the CP clinic inclusive of imaging results, comorbidities, risk factors, and Gross Motor Functional Classification Scale (GMFCS) level.
Methods
Study centre
The CP clinic at CHBAH is held every week on a Tuesday. Children with CP from Soweto (population of ~1.3 million, 2011 census[7]) and surrounding areas are seen at this clinic. It is run by 2 specialist neurologists, 2 paediatric registrars (rotating through neurology every 2 months), nurses, physiotherapists, and speech and occupational therapists. Patients are referred to the CP clinic from the neonatal follow-up clinic at CHBAH and from clinics in Soweto and surrounding hospitals. Approximately 4 - 5 new patients and 20 follow-up patients are booked and seen per week at the CP clinic; the services provided are consultancy, referral for physiotherapy, occupational therapy (OT), speech therapy, orthopaedics and dietetics. Selected patients are treated with botulinum toxin (Botox).
Data
All CP patients who presented for the first time to the CP clinic in 2012 were screened for enrolment. Demographic data, radiology reports, GMFCS scores and perinatal history were extracted from the patient files. Patients excluded were those with syndromes and chromosomal abnormalities, and patients presenting with loss of previously attained milestones, suggesting a progressive disorder. A total of 145 patients from the 201 new cases of CP presenting to the CP clinic during the study period were included in the study.
Definition of terms
Preterm delivery was defined as born alive before 37 completed weeks of gestation while term delivery was defined as born between 37 and 41 weeks' gestation. Post-term delivery was defined as born at 42 weeks' gestation and beyond. Gestational age was determined by first day of last normal menstrual period (LNMP) and/or early sonar (done before 20 weeks' gestation) estimating the gestational age. Birthweight was defined according to the following categories: (i) extreme low birthweight (ELBW): <1 000 g; (ii) very low birthweight (VLBW): 1 000 - 1 499 g; (iii) low birthweight (LBW): 1 500 - 2 499 g; (iv) normal birthweight (NBW): 2 500 - 4 200 g; and (v) large for gestational age (LGA): >4 200 g.
There are 5 types of CP, defined as follows: (1) spastic CP is a stretch-dependent hypertonus which can be abolished by posterior root section and may be of 2 types: (i) phasic spasticity that is velocity dependent and (ii) tonic spasticity. Spastic CP is further divided into 4 subtypes: hemiplegia, diplegia, quadriplegia and double hemiplegia, according to which parts of the body are affected. Hemiplegia refers to documentation of unilateral involvement, diplegia refers to disproportionate lower extremity involvement, and quadriplegia refers to whole body involvement. Double hemiplegia refers to quadriplegia where the arms are significantly more affected than the legs; (2) dyskinetic CP is due to lesions in the basal ganglia and their pathways. It is characterised by involuntary movements (chorea or athetosis) and abnormal muscle tone which consists of rigidity. These patients usually present with an extensor dystonic posturing; (3) hypotonic CP is due to injury to the cerebellum and its pathways, and the tone is usually decreased in the trunk; (4) ataxic CP presents with a loss of orderly muscular co-ordination and movements that are performed with abnormal force, rhythm and accuracy. It occurs as a result of lesions in the cerebellum; and (5) mixed CP may involve a combination of the groups described above.[3,8]
We applied the current version of the GMFCS and the Gross Motor Function Classification System-Expanded and Revised (GMFCS-ER) to each case of CP in our study. The GMFCS-ER is a system that rates the patient's locomotive function, taking into consideration the use of mobility aids and the execution of sitting, standing and walking activities. As motor functions of children differ according to age, functions have been defined for the following age categories: <2 years, 2 - 4, 4 - 6, 6 - 12 and >12 years. The definitions of GMFCS-ER were taken from the Can Child Centre for Childhood Disability Research.[9]
Some of the patients referred to the clinic had cranial sonars, computed tomography (CT) brain or magnetic resonance imaging (MRI) brain scans done. However, because of the large demand for CT and MRI imaging at CHBAH, not all CP patients were able to have brain imaging performed. The neuro-imaging results were based on radiology reports extracted from the patient's clinical records. Neuro-imaging was performed at presentation and cranial sonars were repeated 3 - 6 months later. CT and MRI scans were not repeated. Neuro-imaging results were reported as suggested by Krägeloh-Mann and Horber, as follows: normal, miscellaneous, deep grey matter lesions (DGML), periventricular white matter lesions (PWML), and brain maldevelopments.[10]
Statistical analysis
Categorical data are presented as frequencies and proportions and further reproduced using histograms and tables. Continuous data are presented as means and standard deviations (SDs). The test was used to compare 2 categorical variables. All data were analysed using STATA version 12 (StataCorp., USA).
Ethics
Ethics approval was obtained from the ethics committee of the University of the Witwatersrand (ref. no. M130377). Data were collected from clinic files and entered onto a data collection sheet, and thereafter managed using Research Electronic Data Capture (REDCap).[11] REDCap uses a MySQL database via a secure web interface; with data checks used during data entry to ensure data quality.
Results
Demographics of CP patients
A total of 201 patient records were retrieved and reviewed. The age range of the patients was 3 months to 18 years, with a mean (SD) age at presentation of 34.7 (35) months. The age when patients first presented to the CP clinic was stated for 144 of the 145 patients seen (these patients were included in the study as the date of first presentation corresponded with the stipulated study timeline). Nearly two-thirds of the patients were male (Table 1). The majority of patients (75%) were born at term and 36 (25%) patients were preterm. The preterm cohort had a median gestational age of 30 (interquartile range (IQR) 27 - 34) weeks and a median birthweight of 1 620 g (IQR 760 g - 2 000 g), while the babies who were born at term had a median gestational age of 37 (IQR 37 - 38) weeks with a median birthweight of 3 118 g (IQR 2 797 - 3 373). Forty percent (n=15) of the babies who were born preterm were LBW. Forty-seven percent of preterm babies were born by emergency caesarean section v. 21% of term babies; there was no statistically significant difference (p=0.137). Table 1 shows the demographics of CP patients at CHBAH.
Risk factors
Table 2 shows the antenatal, perinatal and neonatal risk factors for CP in the patients who were reviewed. The majority of CP patients had been diagnosed with neonatal encephalopathy (n=70, 48%). More than two-thirds (n=50/70, 71%) of these patients were born at term. The largest contributing neonatal risk factor was infections (13%).
CP type
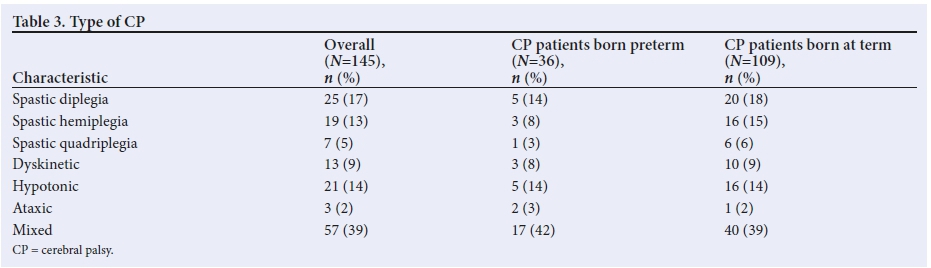
Mixed CP (39%) was the predominant type of CP seen in our patients, and spastic-dyskinetic CP was the most common subtype diagnosed (28% of patients). In 70% (n=29) of the patients in this subcategory, the predominant motor deficit was dyskinetic (inclusive of dystonia and choreoathetosis). There was no association between gestational age (whether term or preterm) and type of CP (p=0.960) (Table 3).
Imaging results
Imaging in the form of cranial ultrasound (35.2%, n=31), CT scan (57.9%, n=51), and MRI of the brain (6.7%, n=6) was performed on 88 (60%) of the patients reviewed. Imaging results were reported as suggested by Krägeloh-Mann and Horber.[10] There were 6 patients (6.8%) with brain maldevelopments of whom 2 patients had lissencephaly, 3 had schizencephaly, and 1 had polymicrogyria. PWML included lesions such as periventricular leukomalacia (PVL), lesions from intraventricular haemorrhage (IVH), and lesions from periventricular or haemorrhagic infarcts. The majority of patients had PWML (54%, n=48). PVL occurred in 12.5% of patients, and IVH was reported in 4.5% ofpatients. Cortical/DGML included basal ganglia lesions, parasagittal injury, multicystic encephalomalacia, thalamic lesions and middle cerebral artery infarcts. Miscellaneous findings were hydrocephalus, slit-like ventricles, ventriculomegaly, cerebral oedema and cerebral atrophy. Eleven patients had normal neuroimaging results.
Comorbidities
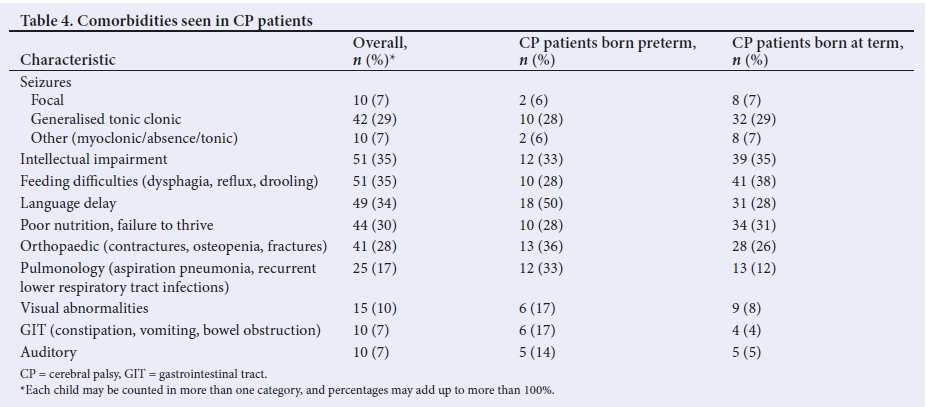
Intellectual impairment was the most frequent comorbidity, and was reported in 35% of patients. Orthopaedic complications were seen in 28% of our patients. Patients with mixed CP (spastic-dyskinetic group) had the most orthopaedic complications (34%, n=14) which included contractures, hip dislocations, subluxations, osteopenia and osteoporosis. Hip dislocations were a significant problem in patients with spastic quadriplegia, occurring in more than half of them (57%, n=4). Generalised tonic-clonic epilepsy was seen in a majority of patients (28%, n=42). Most patients (42.5%) had seizures at the beginning of their course and stabilised with treatment. The dyskinetic CP type comprised the majority of patients with severe intellectual impairment (100%, n=13). Visual and hearing impairment were the least occurring complications (10% and 7% of patients, respectively) (Table 4).
GMFCS level
More than a third (36.50%) of the patients were found to be functioning at GMFCS level III. Patients with level IV (26.8%) and level V (13.7%) GMFCS were the most severely affected, as they were wheelchair bound (Table 5). The type of CP (p=0.008), intellectual impairment (p=0.027) and orthopaedic complication (p=0.003) correlated with a higher GMCSF level.
Discussion
Cerebral palsy is the most common cause of childhood disability worldwide and especially in SA with an estimated incidence of 3 per 1 000 live births.[2] In our cohort of patients, the mean age at first visit was found to be 34.1 months (2.8 years). Patients who were referred from institutions outside CHBAH had a mean age at first presentation of 45.6 months (3.8 years). The transition of care of CP patients from neonatal follow-up clinic occurs at 1 year for term infants and 18 months corrected age for preterm infants. These infants would have been followed up because they had had a complicated neonatal period (complicated by neonatal encephalopathy, sepsis, prematurity and other risk factors for CP).
The incidence of CP in boys was 30% higher than that in girls (63.4% v. 36.6%; p=0.01) in our study. Research into some of the causes of CP has revealed that gender differences in the immature brain are strongly influenced by intrinsic differences between male and female cells; this is due to their distinct chromosomal complements. Evidence suggests that cellular pathways involved in neuronal death after infant brain injury differ between male and female. Sex chromosomes rather than sex hormones have been implicated in the gender difference. Male newborns have a higher incidence of brain-based developmental disabilities as they are more prone to extreme prematurity and its complications.[12]
The contribution of prematurity and ELBW in the increasing prevalence of CP is due to improved obstetric and neonatal care. Premature birth before 28 weeks' gestation and post-term deliveries (>42 weeks' gestation) are associated with an increased risk for CP.[13] McIntyre et al. [14] performed a systematic review of risk factors for CP in children born at term in developed countries. The conclusion of their study was that placental abnormalities, major and minor birth defects, LBW, meconium aspiration, instrumental or emergency caesarean delivery, birth asphyxia, neonatal seizures, respiratory distress syndrome, hypoglycaemia and neonatal infections were all statistically significant contributing risk factors for CP. The leading risk factor for the development of CP in our cohort of patients was neonatal encephalopathy. The incidence of perinatal asphyxia in our population is high and was reported to range from 8.7 to 15.2 per 1 000 live births as opposed to the lower rate of 1 to 6 per 1 000 live births in the developed world.[15] Risk factors for the development of neonatal encephalopathy may be due to antenatal, intrapartum and postnatal factors, which in turn may be due to placental, fetal or maternal factors as well. It is important to recognise these factors and manage them appropriately to diminish the risk factor for the development of CP.
Mixed CP (spastic-dyskinetic subtype) was the most common type of CP seen in our cohort of patients. Spastic CP is the most common type of CP, occurring in 70 - 75% of all cases, and dyskinetic CP is the second most common type and accounts for 10 - 15% of cases. Ataxic CP accounts for less than 5% of cases.[16]The high number of patients in our study population diagnosed with mixed predominantly spastic diplegic CP could be due to improved prenatal, natal and neonatal intensive care of premature infants. Dyskinetic CP was associated with neonatal hyperbilirubinaemia and hypoxic ischaemic encephalopathy. There was a strong association between the type of CP and the GMFCS (p=0.009).
The GMFCS has been used as a measure of severity. Level I denotes the least impairment in physical capabilities and level V denotes the worst impairment. The importance of early physical treatment is emphasised, as individuals with a poor GMFCS score (grade III and IV) may regain some functionality with intense treatment.[17] Howard et al.[18] studied the distribution of motor impairment in a large population cohort of patients with CP from the Victorian Cerebral Palsy Register (VCPR) for the birth years 1990 - 1992 in Australia. They found that GMFCS classification level I was the most common (35%) level and the remaining cases were distributed fairly equally from levels II to V (14 - 18% per level). In our study, most patients were found to be functioning at level III (36.50%), 27% were at level IV, and 12.5% level V. These patients had no means of independent movement and were diagnosed with quadriplegic (8.9%) or dyskinetic (3.4%) types of CP. A small proportion (16%) of patients were functioning at GMFCS level II and only 6% at level I GMFCS. The dissimilarity is that level I, which is the mildest form, is the most common in higher-income countries. This finding echoes improved neonatal care, early diagnosis of CP, the different aetiologies and their timely detection, the quality of rehabilitation, and adherence to therapy in higher-income countries which is probably lacking in lower-middle-income countries.
The present study is one of the few in SA, after Molteno and Arens,[19] and van Toorn et al,[6]to describe neuroimaging and GMFCS in patients with CP. The major neuroimaging findings in our cohort of patients were PWML, occurring in 54% of patients; this is in contrast to the study by Kakooza-Mwesige et al.,[20] who found that the most common imaging abnormality in their Ugandan cohort of patients was primary grey matter lesions (found in 44% of patients). PVL was seen in 12.5% of patients (both term and preterm infants) in our study. Children who are born at term with PVL are more likely to have diffuse brain injury than those born preterm, indicating differential timing of the brain injury. PVL affects the motor, cognitive and social adaptive patterns of children born preterm.[21,22] IVH, reported in 4.5% of our study population, is a complication of prematurity, especially of VLBW infants. Patients with IVH have a 50% risk of developing CP.'231 Basal ganglia lesions (DGML) were the least-seen imaging abnormalities, and they were seen in patients with asphyxia. These lesions are associated with congenital hyperbilirubinaemia and kernicterus, and patients present with dyskinetic and ataxic types of CP. There was no association between neuroimaging and GMFCS (p=0.44).
The comorbid conditions associated with CP are those that adversely affect the child's quality of life rather than the CP itself. In our study, intellectual impairment (35%), seizures (42.5%), and orthopaedic (28%) and gastrointestinal problems (41%) were frequent among patients, similar to a study in South India by Amoghimath et al.[24] and a study in South Egypt by Abas et al.[25]
These studies as well as ours show that CP in developing countries has a different clinical profile regarding severity and associated disabilities when compared with developed countries where there is adherence to good-quality rehabilitation therapy. There was an association between orthopaedic complications and GMFCS levels (p=0.003).
Study limitations
The study was a retrospective study from a single centre, over a period of one year. As it was a consecutive convenient sampling of all CP patients who presented for the first time to the CHBAH CP clinic, it therefore introduced sample bias. As the study was a review of clinical records, some data were missing from the clinical records. The neuroimaging results were not retrieved and reviewed by a blinded radiologist; they were based on radiology reports in patient records. The gender ratio in the general neurology and paediatric clinics was unknown, and we were therefore unsure whether we saw more males at the clinics than females. It was not known whether female infants (term and preterm) with neonatal encephalopathy die in the perinatal period, as this would have skewed the ratio towards males being more frequently diagnosed with CP than females. The clinical records had insufficient information about antenatal and intrapartum risk factors for CP.
Conclusion
In our cohort of patients, PWML was frequently reported on imaging results, and DGML was infrequently described, in contrast with other developing countries; some patients had normal imaging reports. Most of our patients functioned at GMFCS level III, with a higher GMFCS level correlating with the type of CP, intellectual impairment and orthopaedic complications. The majority of CP patients had been diagnosed with neonatal encephalopathy. We believe this research has important clinical and research implications, especially in the era of medicolegal litigation concerning CP. We have shown that there are a variety of risk factors for CP and that imaging may be normal in patients diagnosed with CP. The prevention and management of hypoxic ischaemic brain injury is fundamental in decreasing the incidence and complications of CP, especially in our country where the incidence is high. Treatment modalities such as induced hypothermia have been shown to improve outcome of patients with hypoxic and traumatic brain injury.[26] In our neonatal department, induced hypothermia is offered to patients who meet the criteria for neonatal encephalopathy. Future research is needed to assess the link between risk factors, timing of the occurrence of risk factors, and neuroimaging in the prevention of CP.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgements. NM: I would like to thank my supervisors Dr F Nakwa and Prof. J Rodda, and Alane Izua for her support in the statistical analysis.
Author contributions. NM: guarantor of the manuscript and responsible for the integrity of the data and the accuracy of data analysis, data collection, statistical analysis and interpretation of data; drafting, writing, reviewing and incorporating co-authors' feedback, revision and approval of the submission. FN: contributed to the study concept; interpretation of the data; review, revision and approval of the manuscript. JR: interpretation of the data; review, revision and approval of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Rosenbaum P, Paneth N, Leviton A, et al. A report: The definition and classification of cerebral palsy. International Executive Committee for definition and classification of CP workshop. Dev Med Child Neurol 2007;109:8-14. [ Links ]
2. Centers for Disease Control and Prevention. Data and statistics for cerebral palsy. Atlanta: Elsevier Publishing, 2012. [ Links ]
3. Cans C. Surveillance of cerebral palsy in Europe: A collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol 2000;42(12):816-824. [ Links ]
4. Couper J. Prevalence of childhood disability in rural KwaZulu-Natal. S Afr Med J 2002;92(7):549-552. [ Links ]
5. Christianson AL, Zwane ME, Manga P, et al. Children with intellectual disability in rural South Africa: Prevalence and associated disability. J Intellect Disabil Res 2002;46:176-186. [ Links ]
6. Van Toorn R, Laughton B, van Zyl N, et al. Aetiology of cerebral palsy in children presenting at Tygerberg Hospital. S Afr J Child Health 2007;1(2):74-77. [ Links ]
7. Statistics South Africa. Statistical release (revised). Consensus 2011. Updated 30 October 2012. www.statssa.gov.za/census 2011 (accessed 9 August 2017). [ Links ]
8. Wittenberg DF. Coovadia's Paediatrics and Child Health: A Manual for Health Professionals in Developing Countries. 6th ed. Cape Town: Oxford University Press, 2009:580-584. [ Links ]
9. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39:214-223. https://doi.org/10.1111/j.1469-8749.1997.tb07414.x [ Links ]
10. Krägeloh-Mann I, Horber V. The role of magnetic resonance imaging in elucidating the pathogenesis of cerebral palsy: A systematic review. Dev Med Child Neurol 2007;49:144-151. https://doi.org/10.1111/j.1469-8749.2007.00144.x [ Links ]
11. Harris AP, Robert T, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
12. Johnston MV, Hagberg H. Sex and the pathogenesis of cerebral palsy. Dev Med Child Neurol 2007;49:74-78. [ Links ]
13. Stavsky M, Mor O, Mastrolia SA, et al. Cerebral palsy - trends in epidemiology and recent development in prenatal mechanisms of disease, treatment, and prevention. Front Pediatr 2017;5:21. https://doi.org/10.3389/fped.2017.00021 [ Links ]
14. McIntyre S, Taitz D, Keogh J, Goldsmith S, Badawi N, Blair E. A systematic review of risk factors for CP in children born at term in developed countries. Dev Med Child Neurol 2013;55:499-508. https://doi.org/10.1111/dmcn.12017 [ Links ]
15. Bruckmann EK, Velaphi S. Intrapartum asphyxia and hypoxic ischaemic encephalopathy in a public hospital: Incidence and predictors of poor outcome. S Afr Med J 2015;105(4):298-303. https://doi.org/10.7196%2FSAMJ.9140 [ Links ]
16. Dias E, Dias A. Cerebral palsy: A brief review. Acad J Ped Neonatol 2017;4:1. https://doi.org/10.19080/AJPN.2017.03.555687 [ Links ]
17. Wood E, Rosenbaum P. The gross motor function classification system for cerebral palsy: A study of reliability and stability over time. Dev Med Child Neorol 2000;42(5):292-296. [ Links ]
18. Howard J, Soo B, Graham HK, et al. Cerebral palsy in Victoria: Motor types, topography and gross motor function. J Paediatr Child Health 2005;41:479-483. [ Links ]
19. Arens LJ, Molteno CD. A comparative study of postnatally-acquired cerebral palsy in Cape Town. Dev Med Child Neurol 1989;31:246-254. [ Links ]
20. Kakooza-Mwesige A, Byanyima RK, Tumwine JK, et al. Grey matter brain injuries are common in Ugandan children with cerebral palsy suggesting a perinatal aetiology in full-term infants. Acta Paediatrica 2016;105:655-664. https://doi.org/10.1111/apa.13352 [ Links ]
21. Lasry O, Shevell MI, Dagenais L. Cross-sectional comparison of periventricular leukomalacia in preterm and term children. Neurology 2010;74:1386-1391. https://doi.org/10.1212/WNL.0b013e3181dad62d [ Links ]
22. Choi JY, Rha D, Park ES. The effects of the severity of periventricular leukomalacia on the neuropsychology outcomes of preterm children. J Child Neurol 2016;31(5):603-612. https://doi.org/10.1177/0883073815604229 [ Links ]
23. Wei JC, Catalano R, Profit J, et al. Impact of antenatal steroids on intraventricular hemorrhage in very low birth weight infants. J Perinatol 2016;36(5):352-356. https://doi.org/10.1038%2Fjp.2016.38 [ Links ]
24. Amoghimath R, Gowda VK, Benakappa A. Comorbidities and their relationship to subtype of cerebral palsy in a tertiary care hospital in South India. Indian J Cereb Palsy 2016;2:90-93. https://doi.org/10.4103/2395-4264.204408 [ Links ]
25. Abas O, Abdelaziem F, Kilany A. Clinical spectrum of cerebral palsy and associated disability in South Egypt: A local survey study. Open Access Maced J Med Sci 2017;15:5(1):37-41. https://doi.org/10.3889/oamjms.2017.020 [ Links ]
26. Davidson JO, Wassink G, van den Heuij LG, et al. Therapeutic hypothermia for neonatal hypoxic ischemic encephalopathy - where to from here? Front Neurol 2015;6:198. https://doi.org/10.3389/fneur.2015.00198 [ Links ]
 Correspondence:
Correspondence:
N Mahlaba
ntombizodwa.mahlaba2@wits.ac.za
Accepted 20 May 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}