










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.14 no.1 Pretoria Abr. 2020
http://dx.doi.org/10.7196/SAJCH.2020.v14i1.1755
EDITORIAL
South African undergraduate paediatric clinical training: A call to action
In a recent letter to the editor of the South African Medical Journal (in press), we lamented the problems in undergraduate bedside paediatric clinical teaching. We attributed these problems to the lack of collaboration between clinicians, educators, medical schools, the National Department of Health (NDoH) and the National Department of Higher Education towards training fit-for-purpose junior doctors who can competently and effectively care for children. As two of the authors of this editorial are paediatric educators who have trained scores of interns over the last two decades, we would like to voice our concerns about the level of clinical and reasoning skills of interns, irrespective of the medical school at which they were trained.
This editorial serves as a national call to action to improve the quality of paediatric undergraduate clinical training. Drawing on the successful example of the development of the Standard Treatment Guidelines and Essential Medicines List for South Africa,[1] we advocate that the NDoH co-ordinate the appointment of a task team to support paediatric undergraduate teaching. The task team will consist of clinicians and educational experts from the nine South African medical schools and will develop a national undergraduate paediatric training curriculum, propose the best methods for teaching particular topics, and suggest an assessment strategy.
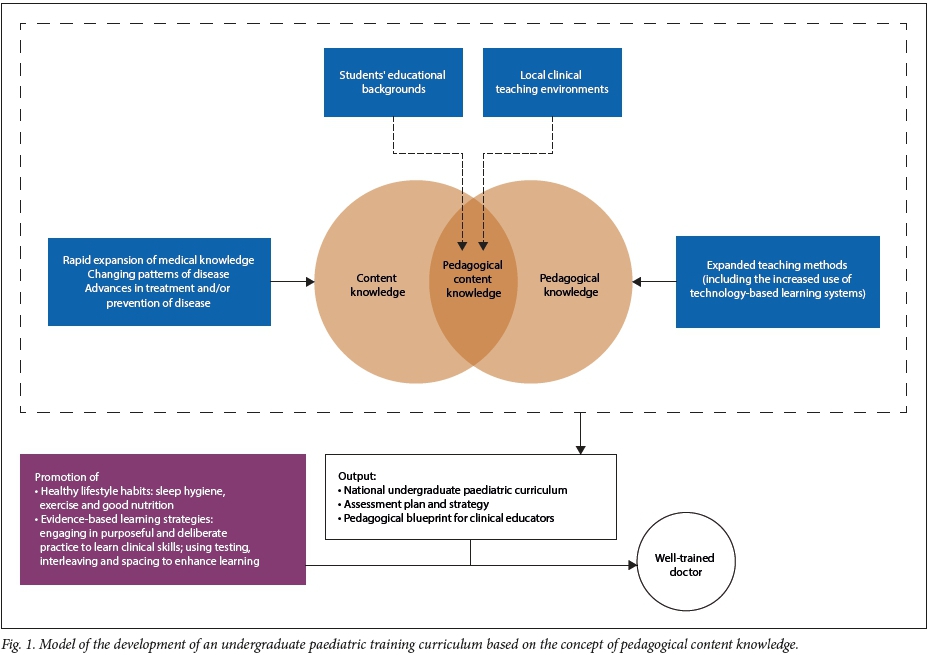
The model shown in Fig. 1 represents the process we envisage the task team undertaking. Central to the model is the concept of pedagogical content knowledge (PCK). PCK recognises knowledge as the basis for good teaching but posits that teachers' knowledge of their subject matter (content knowledge) and their knowledge of pedagogical strategies (pedagogical knowledge) should not be regarded as two separate domains.[2] Instead, teachers' content knowledge and their pedagogical knowledge should integrate to form the PCK required to teach a particular topic.[2] We recommend that the concept of PCK, which has been applied across many diverse fields including mathematics and the natural sciences,[3] forms the basis of developing an undergraduate paediatric curriculum that integrates the content to be taught with appropriate teaching methods.
While clinician educators can be expected to have knowledge of their discipline (content knowledge), they may not be aware of the different pedagogical methods they could use to teach particular topics (pedagogical knowledge), notwithstanding the unique nature of clinical teaching.[4] Many clinician educators teach based on their personal experience of teaching,!51 without a sound knowledge of medical education.[6] There is thus a need for clinician educators to be made aware of different teaching methods to enhance their development of PCK and promote learning, as shown in the model.
A recent meta-analysis of 132 papers compared the magnitude of learning effects associated with different clinical teaching methods.[7] The authors advocated for the inclusion of teaching methods identified as effective, including mastery learning (a combination of activities including repetitive practice and regular feedback[8]), small group learning and goal setting (teacher-designated goals based on student levels and expected outcomes[8]), worked examples, play programmes, questioning, concept mapping, metacognitive strategies and visual perception programmes.[7]
While clinicians have the content knowledge, the task team will need to consider content-related factors like the rapid expansion of medical knowledge, as shown in the model. The estimated doubling time of medical knowledge in 1950 was 50 years; this year (2020), it is projected to be just 73 days.[9] This 'expansion of knowledge will force medical schools to define those concepts that form the essential core of what students must learn.'[9] The core curriculum will need ongoing review to ensure that the content taught is focused, relevant and manageable.
The task team would need to consider the local clinical teaching environments across the country, as well as our students' diverse educational backgrounds, to suggest suitable pedagogical methods that will ensure effective teaching of the national curriculum. The curriculum would also contain a list of essential practical clinical skills that need to be mastered to produce competent graduates.
The outputs from the task team, a core undergraduate paediatric curriculum, an assessment strategy, and a pedagogic blueprint for suggesting teaching methods for different topics, would standardise the teaching across medical schools by providing a benchmark that could address curricular gaps across universities and provide additional guidance for less well-resourced universities. The collaborative development of a national paediatric training curriculum could potentially provide a framework for other clinical disciplines, as well as new medical schools in the country.
In parallel with the implementation of the new curriculum, the critical importance of healthy lifestyle habits and evidence-based learning strategies to promote effective learning[10] must be taught to undergraduate students, especially those from disadvantaged educational backgrounds. The principles of purposeful and deliberate practice[1] will teach students how to build strong foundations for the content knowledge and clinical skills that they need to learn and master.
The implementation of a national curriculum brings with it responsibilities for clinicians that include a paradigm shift in our approach and execution of teaching. Although mistakes will be made and lessons learnt during the development of the national curriculum, clinician educators must be willing to undertake training based on the recommendations of the task team to gain insight into evidence-based teaching methods. Clinical educators need to be aware that content knowledge is not sufficient to ensure the best learning outcomes and that they need to develop the 'content-specific pedagogical knowledge'[12] to promote meaningful engagement and deep learning.

Ann George
BSc (cum laude), BSc Hons, PhD Centre for Health Science Education, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa ann.george@wits.ac.za
Ziyaad Dangor
MB BCh, FCPaed (SA), MMed, PhD (Wits) Paediatric Education and Research Ladder, Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa ziyaad.dangor@wits.ac.za
Sanjay G Lala
MB BCh, FCPaed (SA), MMed, PhD (London) Paediatric Education and Research Ladder, Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, and Perinatal HIV Research Unit, Chrs Hani Baragwanath Hospital, Johannesburg, South Africa sanjay.lala@wits.ac.za
References
1. South African National Department of Health (NDoH). Standard Treatment Guidelines and Essential Medicines List for South Africa Hospital Level 2017 Edition. Pretoria: NDoH, 2017. [ Links ]
2. Shulman LS. Those who understand: Knowledge growth in teaching. Educ Res 1986;15(2):4-14. [ Links ]
3. Evens M, Elen J, Depaepe F. Developing pedagogical content knowledge: Lessons learned from intervention studies. Educ Res Int 2015(1):1-23. https://doi.org/10.1155/2015/790417 [ Links ]
4. Spencer J. ABC of learning and teaching in medicine: Learning and teaching in the clinical environment. BMJ 2003;326(7389):591-594. https://.doi.org/10.1136%2Fbmj.326.7389.591 [ Links ]
5. Irby D. Educating physicians for the future: Carnegie's calls for reform. Med Teach 2011;33(7):547-550. https://doi.org/10.3109/0142159X.2011.578173 [ Links ]
6. Misch D. Androgogy and medical education: Are medical students motivated to learn? Adv Heal Sci Educ 2002;7:153-160. https://doi.org/10.1023/a:1015790318032 [ Links ]
7. Huang PH, Haywood M, O'Sullivan A, Shulruf B. A meta-analysis for comparing effective teaching in clinical education. Med Teach 2019;41 (10): 1129-1142. https://doi.org/10.1080/0142159X.2019.1623386 [ Links ]
8. Missouri's Educator Evaluation System. Research and Proven Practices of Dr. John Hattie. Jefferson City (MO): Missouri Department of Elementary and Secondary Education, 2017. [ Links ]
9. Densen P. Challenges and opportunities facing medical education. Trans Am Clin Climatol Assoc 2011;122:48-56. [ Links ]
10. Brown P, Roediger H, McDaniel M. Make It Stick. The Science of Successful Learning. Cambridge: Harvard University Press, 2014. [ Links ]
11. Ericsson A, Pool RP. Peak: Secrets from the New Science of Expertise. Boston: Houghton Mifflin Harcourt, 2016. [ Links ]
12. McLeod P, Steinert Y, Chalk C, et al. Which pedagogical principles should clinical teachers know? Teachers and education experts disagree. Disagreement on important pedagogical principles. Med Teach 2009;31(4):e116-124. [ Links ]


{kind=link}