










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Child Health
versão On-line ISSN 1999-7671
versão impressa ISSN 1994-3032
S. Afr. j. child health vol.13 no.4 Pretoria Dez. 2019
http://dx.doi.org/10.7196/sajch.2019.v13i4.1619
RESEARCH
Demographic and socioeconomic factors associated with under-5 mortality in KwaZulu-Natal, South Africa
M HlongwaI; N de WetII
IMA; Demography and Population Studies, Schools of Public Health and Social Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; Demography and Population Studies, Schools of Public Health and Social Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. The KwaZulu-Natal (KZN) Province remains one of the provinces mostly affected by under-5 mortality in South Africa, despite the many programmes and policies implemented to prevent under-5 children from dying.
OBJECTIVE. To examine the association between socioeconomic and demographic factors and under-5 mortality in KZN.
METHODS. The study was cross-sectional and based on a secondary data set from the 2011 national census, conducted by Statistics South Africa. From the 10% sample, 1 474 under-5-year-olds had died in the province during the period of data collection. Statistical analysis was performed in Stata 12.0 and involved univariate, bivariate and multivariate analysis.
RESULTS. The results showed that maternal variables such as age, education level and race, as well as annual household income were predictors of under-5 mortality. Male children were also found to have a higher likelihood of dying before the age of 5 years than female children.
CONCLUSION. The study identified several socioeconomic and demographic factors as predictors of under-5 mortality in KZN. The findings suggest the importance of up-scaling and strengthening interventions aimed at reducing under-5 mortality in the province, with specific focus on addressing the needs of young black women, those with limited education and women from poor households.
The under-5 mortality rate (U5MR) is a reflection of a country's socioeconomic conditions, including the healthcare system and economic development.[1] Estimates indicate that in 2010 more than 7 million under-5-year-olds died worldwide, with almost three-quarters of these deaths among infants. Sub-Saharan African countries are the worst affected, and contribute 35% of all global deaths of children under the age of five years.[2] Diseases such as pneumonia (18%), diarrhoea (9%), malaria (7%), and meningitis and tetanus (6%) remain the leading causes of death among under-5s globally.[3] An increase of 17% in under-5 deaths (from 125 to 146 deaths per 1 000 live births) has been reported for the sub-Saharan African region between 1990 and 2006.[4] Although a decline in under-5 mortality has been noticed in recent years (72 deaths per 1 000 live births in 2015[5]), the rates remain high relative to the target of 25 per 1 000 live births by 2030 as set out in the Sustainable Development Goals.[6]
Children in South Africa (SA) and other developing countries are at high risk of dying before their fifth year of life.[7] Thousands of children under the age of five years die in SA each year,[7] with as many as 24 216 deaths recorded among infants in 2015.[8] In SA, HIV/AIDS, diarrhoeal diseases, lower respiratory tract infections and low birthweight remain the most common diseases associated with child death.[9]
To reduce the high U5MR in the country, the SA government has invested substantial financial and other resources aimed at improving child health. Before the implementation of the National Development Plan, SA worked towards achieving Millennium Development Goal 4, which aimed to reduce child mortality by two-thirds. Some initiatives introduced by the government were programmes such as the Negotiated Service Delivery Agreement 2010 - 2024, the Strategic Plan for Maternal, Newborn, Child and Women's Health, and the Campaign for Accelerated Reduction of Maternal and Child Mortality.[3] However, by 2013, little progress had been made, with mortality rates still as high as 47 deaths per 1 000 children under five.[2,3]
In SA, high levels of poverty, due to high unemployment rates and subsequently low income levels, contribute to children in such households being deprived of basic services required for survival and optimal health, including having nutritious food and access to basic healthcare services.[10] The KwaZulu-Natal (KZN) province is particularly affected. The province has high unemployment and illiteracy rates (33% and 22%, respectively), more than 30% of households are in rural areas, and has a higher U5MR than elsewhere in SA.[11] In 2011, 28% of the 55 476 under-5 deaths in SA were recorded in KZN, followed by Gauteng (17%), Eastern Cape (14%), Limpopo (10%), Mpumalanga (9%) and North West (9%). The Free State, Western Cape and Northern Cape provinces reported the lowest under-5 mortality figures (7%, 4% and 2%, respectively).[12]
Studies on the association between socioeconomic and demographic factors and under-5 mortality have reported some contradicting findings, both locally and internationally.[13-15] For example, some studies have shown child mortality to be significantly associated with living in rural areas, while others have established the reverse.[13,14] Likewise, some results have shown that children born to younger mothers (<20 years of age) had a high likelihood (52%) of dying before their fifth year of life,[15] whereas a study in Ghana found that children born to older mothers (>35 years) were at higher risk.[14]
The main objective of this study was to investigate the maternal demographic and socioeconomic factors associated with under-5 mortality in KZN. The outcomes of the study may contribute to Chapter 10 of SA's National Development Plan, which aims to significantly reduce the burden of mortality among under-5s by 2030.[16]
Methods
Data
The 10% sample of the 2011 national census was used for this study. During the census, a total of 14 450 161 households were successfully interviewed across the country, of which 2 539 429 were in KZN.[17] The census reported the SA population size as 51 770 560. Of the total of 604 545 deaths recorded, findings showed that 55 476 children under the age of 5 years had died in the 12 months prior to the census. In KZN, this number was 15 356 based on maternal reports. The information from KZN also showed that 777 288 under-5s were alive.[17] According to the sample, 65 349 women had had their last child during the 5 years preceding the census, regardless of whether the child was still alive.
The census questionnaires used to survey mothers between the ages of 12 and 50 years focused on fertility and mortality.[17] The questionnaires were checked for consistency, and edited where necessary, during the pilot stage of data collection. Recorded data were checked for quality and consistency, and verified in collaboration with a multidisciplinary team of experts including researchers and programmers.
The dependent variable 'under-5 mortality' was derived by recoding and merging the following two variables:
(i) 'When was (name's) last child born, even if the child died soon after birth?' This question aimed to establish the age of the last child born. If mothers could not remember the last child's day or month of birth, they were encouraged to give the year at least. In cases where the mother had multiple births, information was recorded only of the last child. Responses were given in the form of days (01 - 31), months (01 - 12) or years.
(ii) 'Is (name's) last child born still alive?' This question aimed to establish the last child's survival status at the time of the census. Respondents would indicate 'yes' if the child was still alive, 'no' if the child had died, or 'do not know' if the child's survival status was unknown.
Although different age groups were included in these responses, we recoded the dependent variable in our study to focus only on responses referring to children under 5 years. To this end, data were used only of children born between 2006 and 2011. Mortality data included both natural and unnatural deaths. As the dependent variable is dichotomous, 'alive' was coded as 0 and 'dead' as 1.
The independent variables were selected based on the hypothetical foundation established through a literature review to address this study's research question. Many studies have revealed contradictory findings regarding the relationship between under-5 mortality and some of these variables. Our study examined variables specifically at the individual level, which included the characteristics of the mother and child. The demographic variables were: sex of the child; maternal age at first birth; maternal race; and place of residence. The socioeconomic variables were: mother's level of education, mother's employment status, and annual household income.
Analysis
The individual personal and the household data sets were merged to generate a single data set. Stata 12.0 was used for the analysis. The analysis focused only on this study's target population, namely women in KZN who had their last child during the 5 years preceding the census.
The analysis was performed at three levels. The first level involved descriptive (univariate) analysis of variables related to under-5 mortality and demographic and socioeconomic factors. The background characteristics of respondents were described and summarised, and patterns between variables were discussed. Frequency distributions and cross-tabulations were subsequently generated for each independent variable. The following formulae-was used to estimate the U5MR in KZN:

The second step involved bivariate analysis, in which a binary logistic regression model was applied (model 1). This model was used to estimate the probability of the association between the dependent variable and the respective independent variables. Odds ratios (ORs) were used to interpret the results from this model. Pearson's chi-squared (χ2) test was used to verify the level of significance.
The final step involved multivariate analysis by applying a logistic regression model. This model (model 2) was used to analyse variables that proved to be significantly associated (p<0.05) with under-5 mortality during the bivariate stage of analysis. Before applying the logistic regression model, a pairwise correlation test was conducted to test for correlations between independent variables in the 2011 census data. A significance level of p<0.05 at a confidence interval (CI) of 95% was used in all the analyses. Both unadjusted ORs and adjusted ORs and their associated p-values were used to understand factors related to under-5 mortality in KZN.
Results
Background characteristics
Table 1 shows that the sample had a fairly equal distribution of male and female children. The majority of the respondents (76%) had completed at least secondary school, whereas only 7% of the respondents had completed tertiary education. The remaining respondents had either completed only primary education or had no schooling at all. Approximately a quarter of respondents (26%) were employed.
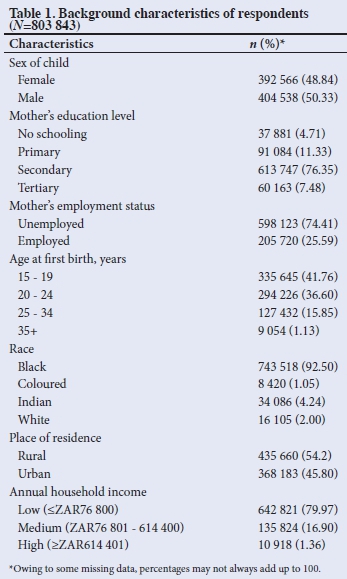
Almost all respondents (94%) were younger than 35 years at first birth, and close to 42% were between 15 and 19 years old. The majority (93%) of respondents were black; only 1% were coloured. Indian and white respondents accounted for 4% and 2% of the sample, respectively.
More respondents lived in rural areas (54%) than in urban areas (46%), and most (80%) lived in low-income households. This finding may be related to the high level of unemployment (74%) in the sample. Of the children who had died before the age of 5, 20% were infants. Based on the census data, the U5MR in KZN was calculated as 22.65 per 1 000 live births.
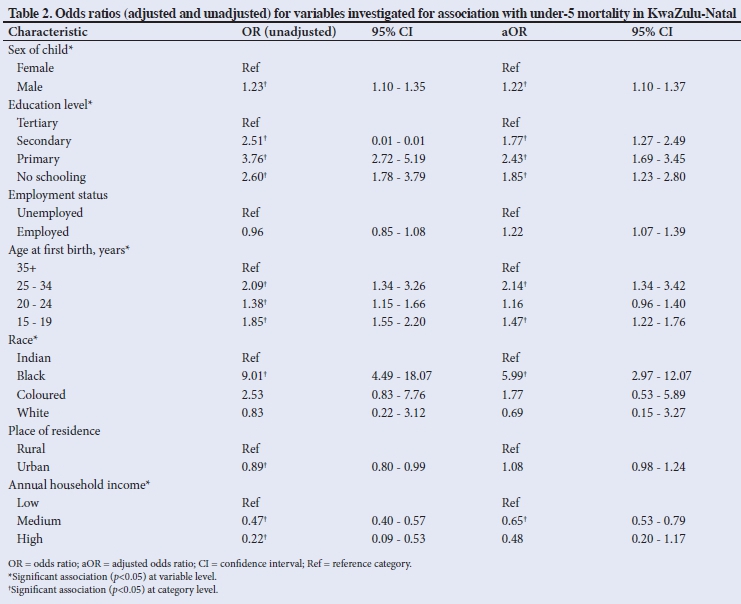
Table 2 shows both the aORs and the unadjusted ORs for each independent variable. Results show that male children were 1.22 times more likely to die before the age of 5 years than female children (95% CI 1.10 - 1.37). Relative to respondents with tertiary education, respondents without any schooling were 1.85 times more likely to experience under-5 mortality (95% CI 1.23 - 2.80). A similar observation held for respondents who had completed only primary education (aOR 2.43; 95% CI 1.69 - 3.45) or secondary education (aOR 1.77; 95% CI 1.27 - 2.49).
The likelihood of under-5 mortality was 1.47 times higher among respondents who were between 15 and 19 years old at the time of their first birth (95% CI 1.22 - 1.76), and 2.14 times higher among respondents between 25 and 34 years of age (95% CI 1.34 - 3.42), compared with those older than 34. No significant association was found between under-5 mortality and the mother's age being between 20 and 24 (p=0.132).
Compared with Indian respondents, under-5 mortality was 5.99 times more likely to be reported by black respondents (95% CI 2.97 - 12.07). However, no significant association was found for reports of under-5 mortality among coloured (p=0.354) or white respondents (p=0.641).
Under-5 mortality was 1.22 times more likely to be reported by respondents who were employed compared with those who were unemployed (95% CI 1.07 - 1.39). With regard to household income, respondents from medium-income households were 0.65 times less likely to report under-5 mortality then those from low-income households (95% CI 0.53 - 0.79). No association was found between high household income and under-5 mortality at the multivariate level (p=0.106).
The pairwise correlation test did not show any of the independent variables to be highly correlated (i.e. a correlation coefficient >0.5). Although statistically significant correlations were seen between a few variable pairs (employment status and annual household income; education level and annual household income; place of residence and annual household income), they were weak. The highest correlation was found between employment status and annual household income (p=0.299). As all the correlation coefficients were <0.5, there are no concerns of multicollinearity among independent variables.
Discussion
Our results show that the child's sex was a significant predictor of under-5 mortality in KZN. This is in line with findings from other studies that showed infants and boys under five more likely to die than girls in this age group.[19-21] The findings are consistent with the pattern of under-5 mortality by sex found in both KZN and nationally,[12] but contradict those from studies in other developing countries (e.g. India and some African countries) that showed healthcare services often being prioritised for male children, as they are perceived as the future leaders and heads of the households.[21-27] This observation could be an important consideration in social planning and for government interventions, because it raises issues regarding possible gender bias. Studies have also suggested that male children are biologically more likely to die before the age of five than female children.[25] Such sex differentials in under-5 mortality are a serious concern for many countries in their efforts to achieve gender equality.[28] Sex bias in general may further contribute to development failures in the province owing to unequal allocation of resources and limited opportunities provided to women to contribute to development goals.[28]
Level of maternal education was shown to be a significant predictor of under-5 mortality by both the adjusted and unadjusted models. This is in line with several studies that reported similar results[29-32] and may be interpreted as confirmation of Mosley and Chen's framework of child survival in developing countries.[33] These findings may be related to higher-educated mothers being better equipped for and more knowledgeable about antenatal care and feeding practices and more aware of measures to prevent serious childhood diseases.[34-37] Mothers without formal education may not be aware of the health benefits of vaccinations, for example.[37] In addition, a higher maternal education level could also lead to mothers accessing healthcare services more often than those with limited or no schooling.[37,38] The finding of a lower likelihood of under-5 mortality being reported by mothers who had no schooling (aOR 1.85) compared with those with primary education (aOR 2.43) was surprising. The reason for this is not clear, but it may be related to the wider family and not only the mother being involved in child care in rural areas, as is seen in large areas of KwaZulu-Natal.
Findings from studies such as this one point to the importance of empowering women by providing equal education opportunities, and can be useful to inform decisions by social planners and government structures for strategically aligning resources and improving interventions aimed at increasing women's access to education. The higher the educational status of the mother, the lower the risk that her child will die before the age of 5 years.[14,39] In light of the government's progress in providing access to education for women, the findings from our study further suggest that policies aimed at promoting education among women should be maintained and strengthened across all levels of education (primary, secondary and tertiary).
Significant associations were found between the mother's age at first birth and under-5 mortality in our study. However, results from studies in other countries have been contradictory: some studies reported a higher likelihood of under-5 mortality being reported by mothers between the ages of 15 and 19 years at first birth, whereas others reported a maternal age of 35 years and older to be strongly associated with under-5 mortality.[14,15] Our results showed that teenage mothers (i.e. those who were between 15 and 19 years old at first birth) and those between 25 and 34 years were most likely to report under-5 mortality.
Teenage pregnancy has been a serious social and public health issue in SA for many years, especially as this age group may not be well equipped for childcare and so could contribute to a high rate of under-5 mortality. Further research is recommended to investigate the underlying reasons for the association of under-5 mortality with a maternal age of 25 - 34 years at first birth, as this result is inconsistent with what has been reported in literature.
The findings regarding the association between under-5 mortality and annual household income are similar to those from previous reports.[29,40,41] We found that mothers living in middle-income households are less likely to report under-5 mortality than those from low-income households. No association was found for high-income households during multivariate analysis, although a significant association was seen in the bivariate analysis. Poor households are found mostly in crowded environments, with limited or no access to basic sanitation and services and limited access to health facilities.[29] Poor households have suboptimal access to healthcare services and often cannot afford nutritious foods, which increase the likelihood of malnourishment in children under five.[42] Children from such households may therefore be more vulnerable to infections that could lead to death.[41]
This finding points to the importance of improved healthcare systems to promote quality of health in poor households. Results from other studies show that low household income may have a negative effect on the health of under-5s, such as malnutrition, illness and limited access to quality healthcare.[13] Fast-tracking the National Health Insurance, a government initiative aimed at ensuring that all SA citizens have access to appropriate, efficient and quality health services, is key in addressing healthcare challenges. Improving the provision of social grants (Child Support Grant) and employment opportunities to women may be necessary to improve the income status among poor families. This, in turn, may help mothers to provide nutritious food for their children despite limited finances and unemployment.
Recommendations and policy implications
The findings from this study may be useful to provincial government structures, social planners, researchers and policy makers to improve child survival status. Given the strong association between maternal education and under-5 mortality seen in this study, programmes and policies should aim to improve women's access to education and maintained attendance across all levels of the education system.
Empowering women through education can have notable effects on income and employment status, and may further also influence the age at which women have their first child and their use of healthcare services.[40] As studies have shown higher education levels to be associated with better use of healthcare services,[37,38] it is important that empowerment initiatives be aligned with the education system.
Rural community development strategies and programmes should be strengthened and the progress monitored in KZN in an attempt to combat poverty. Government's collaboration with local businesses to improve employment and education opportunities for black women in rural areas should be evaluated often to inform interventions
and ensure successful implementation of programmes. This may also improve annual household income, which, in turn, may result in better nutrition and access to healthcare services, and so positively influence children's survival status.[41]
Healthcare services should be improved and brought closer to the rural communities. However, it is not only the physical infrastructure that is important, but also keeping facilities adequately staffed and well stocked with medication. Our findings also point to the importance of pre- and post-natal health education among mothers.
Study limitations
The study was not based on death records but on self-reported data. Incorrect recall of the date of the child's birth or death could therefore have compromised the quality of information, especially if no death certificate was referred to. Although some missing data points were noted, these were minimal (except for the variable 'maternal age at first birth' - 5%) and therefore unlikely to have had a substantial affect on the study outcome. In addition, while the data used in this study are still relevant, they are not recent, and it is possible that some demographic or socioeconomic parameters may have changed since the 2011 census. Owing to the cross-sectional nature of the study, cause-effect relationships could not be established.
Conclusion
This study showed that socioeconomic and demographic factors substantially influence under-5 mortality in KZN. Our findings suggest that black women may have a higher risk of experiencing under-5 mortality and similarly also women in rural areas, those who have limited education, have their first child at a young age or who come from poor households. These findings may be of interest to both provincial and national government structures dealing with issues of social development and health. Understanding the associations between demographic and socioeconomic variables and under-5 mortality as investigated in this study could contribute to addressing the challenges around child health and survival status at a provincial or national level.
Declaration. None.
Acknowledgements. The authors thank the Department of Humanities, Demography and Population Studies, University of the Witwatersrand for academic support.
Author contributions. MH conceptualised and designed the study and prepared the initial draft of the manuscript, reviewed by NdW. Both authors reviewed and approved the final version of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Rajaratnam J, Marcus J, Flaxman A, et al. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970-2010: A systematic analysis of progress towards Millennium Development Goal 4. Lancet 2010;375(9730):1988-2008. https://doi.org/10.1016/s0140-6736(10)60703-9 [ Links ]
2. Sanders D, Bradshaw D, Ngongo N. The status of child health in South Africa. In: Kibel M, Lake L, Pendlebury S, Smith C, eds. South African Child Gauge 2009/2010. Cape Town: Children's Institute, University of Cape Town, 2010:29-40. [ Links ]
3. Statistics South Africa. Millennium Development Goals: Country Report 2013. Pretoria: Stats SA, 2013. [ Links ]
4. United Nations Children's Emergency Fund. The State of Africa's Children. New York: UNICEF, 2008. [ Links ]
5. Golding N, Burstein R, Longbottom J, et al. Mapping under-5 and neonatal mortality in Africa, 2000-15: A baseline analysis for the Sustainable Development Goals. Lancet 2017;390:2171-2182. https://doi.org/10.1016/s0140-6736(17)31758-0 [ Links ]
6. United Nations. Progress towards the Sustainable Development Goals. 2017. [ Links ]
7. You D, Hug L, Chen Y, Wardlaw T, Newby H. Levels and trends in child mortality: Report 2014. New York: United Nations Children's Fund, 2014. https://www.who.int/maternal_child_adolescent/documents/levels_trends_child_mortality_2014/en/ (accessed 18 July 2018). [ Links ]
8. Statistics South Africa. Mortality and Causes of Death in South Africa, 2015: Findings from Death Notification. Pretoria: Stats South Africa, 2015. [ Links ]
9. Bradshaw D, Nannan N, Laubscher R, et al. South African National Burden of Disease Study 2000: Estimates of Provincial Mortality. Pretoria: South African Medical Research Council, 2000. [ Links ]
10. Ester PV, Torres A, Freire JM, Hernandez V, Gil A. Factors associated to infant mortality in Sub-Saharan Africa. J Public Health Africa 2011;2:e27. https://doi.org/10.4081/jphia.2011.e27 [ Links ]
11. Statistics South Africa. Mortality and Causes of death in South Africa, 2013: Findings from Death Notification. Pretoria: Stats SA, 2014. [ Links ]
12. Statistics South Africa. Census 2011. Pretoria: Stats SA, 2012. https://www.statssa.gov.za/publications/P03014/P030142011.pdf (accessed 17 July 2016). [ Links ]
13. Ettarh R, Kimani J. Determinants of under-five mortality in rural and urban Kenya. Rural Remote Health 2014;12:1812. [ Links ]
14. Kanmiki EW, Bawah A, Agorinya I, et al. Socio-economic and demographic determinants of under-five mortality in rural northern Ghana. BMC Int Health Hum Rights 2014;14:24. https://doi.org/10.1186/1472-698x-14-24 [ Links ]
15. Ayotunde T, Mary O, Melvin AO, Faniyi FF. Maternal age at birth and under-5 mortality in Nigeria. East Afr J Public Health 2009;6(1):11-14. https://doi.org/10.4314/eajph.v6i1.45735 [ Links ]
16. South Africa, National Planning Commission. Chapter 10: Promoting health. In: National Development Plan 2030: Our Future - Make it Work. Pretoria: NPD, 2013. https://www.gov.za/sites/default/files/gcis_document/201409/ndp-2030-our-future-make-it-workr.pdf (accessed 18 July 2016). [ Links ]
17. Statistics South Africa. Census 2011 Metadata. Pretoria: Stats SA, 2012. http://www.statssa.gov.za/census/census_2011/census_products/Census_2011_Metadata.pdf (accessed 24 July 2016). [ Links ]
18. Indrayan A, Satyanarayana L. Measures of mortality: Indicators of child mortality. http://www.medicalbiostatistics.com/childmortality.pdf (accessed 12 July 2018). [ Links ]
19. Singh R, Tripathi V. Maternal factors contributing to under-five mortality at birth order 1 to 5 in India: A comprehensive multivariate study. SpringerPlus 2013;2:284. https://doi.org/10.1186/2193-1801-2-284 [ Links ]
20. Nasejje JB, Mwambi HG, Achia TNO. Understanding the determinants of under-five child mortality in Uganda including the estimation of unobserved household and community effects using both frequentist and Bayesian survival analysis approaches. BMC Public Health 2015;15:1003. https://doi.org/10.1186/s12889-015-2332-y [ Links ]
21. Krishnaji N. Working mothers and child survival in rural India: Insights from spatial patterns. Econ Polit Wkly 1995;30(44):2803-2808. [ Links ]
22. Claeson M, Bos E, Mawji T, Pathmanathan I. Reducing child mortality in India in the new millennium. Bull World Health Organ 2000;78:1192-1199. [ Links ]
23. Chen LC, Huq E, D'Souza S. Sex bias in the family allocation of food and health care in rural Bangladesh. Popul Dev Rev 1981;7(1):55-70. https://doi.org/10.2307/1972764 [ Links ]
24. Arokiasamy P. Gender preference, contraceptive use and fertility in India: Regional and development influences. Int J Popul Geogr 2002;8(1):49-67. https://doi.org/10.1002/ijpg.236 [ Links ]
25. Ssewanyana S, Younger SD. Infant mortality in Uganda: Determinants, trends and Millennium Development Goals. J Afr Econ 2007;17(1):34-61. https://doi.org/10.1093/jae/ejm004 [ Links ]
26. Charmarbagwala R, Ranger M, Waddington H, White H. The Determinants of Child Health and Nutrition: A Meta-Analysis. Washington DC: World Bank, 2004. [ Links ]
27. Sartorius B, Sartorius K, Chirwa T, Fonn S. Infant mortality in South Africa - distribution, associations and policy implications, 2007: An ecological spatial analysis. Int J Health Geogr 2011;10:61. https://doi.org/10.1186/1476-072x-10-61 [ Links ]
28. Arokiasamy P. Regional patterns of sex bias and excess female child mortality in India. Population 2005;59(6):831. https://doi.org/10.3917/pope.406.0831 [ Links ]
29. Boadi KO, Kuitunen M. Childhood diarrheal morbidity in the Accra Metropolitan Area, Ghana: Socio-economic, environmental and behavioral risk determinants. J Health Popul Dev Ctries 2005;7:1-13. [ Links ]
30. Cleland J. Maternal education and child survival: Further evidence and explanations. In: Caldwell JC, Findley E, Caldwell P, et al., eds. What We Know about Health Transition: The Cultural, Social and Behavioural Determinants of Health. Canberra: Australian National University, 1990. [ Links ]
31. Hobcraft J. Women's education, child welfare and child survival: A review of evidence. Health Transit Rev 1993;3(2):159-175. [ Links ]
32. Hobcraft JN, McDonald JW, Rutstein SO. Socio-economic factors in infant and child mortality: A cross-national comparison. Popul Stud 1984;38(2):193-223. https://doi.org/10.1080/00324728.1984.10410286 [ Links ]
33. Mosley WH, Chen LC. An analytical framework for the study of child survival in developing countries. Popul Dev Rev 1984;10(Suppl):25-40. https://doi.org/10.2307/2807954 [ Links ]
34. Barrera A. The role of maternal schooling and its interaction with public health programs in child health production. J Dev Econ 1990;32:69-91. https://doi.org/10.1016/0304-3878(90)90052-d [ Links ]
35. Nattey C, Masanja H, Klipstein-Grobusch K. Relationship between household socio-economic status and under-five mortality in Rufiji DSS, Tanzania. Glob Health Action 2013;6:19278. https://doi.org/10.3402/gha.v6i0.19278 [ Links ]
36. El-Zanaty F, Way A. Egypt demographic and health survey 2000. Calverton, MD: Ministry of Health and Population (Egypt), National Population Council, ORC Macro, 2001. https://www.dhsprogram.com/pubs/pdf/FR117/FR117.pdf (accessed 18 May 2016). [ Links ]
37. Sartorius B, Kahn K, Vounatsou P, Collinson M, Tollman S. Young and vulnerable: Spatial-temporal trends and risk factors for infant mortality in rural South Africa (Agincourt), 1992-2007. BMC Public Health 2010;10:645. https://doi.org/10.1186/1471-2458-10-645 [ Links ]
38. Caldwell JC. Maternal education as a factor in child mortality. World Health Forum 1981;2:75-78. [ Links ]
39. Amouzou A, Hill K. Child mortality and socioeconomic status in sub-Saharan Africa. Etude Popul Afr 2004;19(1):1-12. [ Links ]
40. Ujunwa F, Ezeonu C. Risk factors for acute respiratory tract infections in under-five children in Enugu Southeast Nigeria. Ann Med Health Sci Res 2014;4(1):95-99. https://doi.org/10.4103/2141-9248.126610 [ Links ]
41. Birchenall JA. Economic development and the escape from high mortality. World Dev 2007;35:543-568. https://doi.org/10.1016/j.worlddev.2006.06.003 [ Links ]
42. Doctor HV. Does living in a female-headed household lower child mortality? The case of rural Nigeria. Rural Remote Health 2011;11(2):1635. [ Links ]
 Correspondence:
Correspondence:
M Hlongwa
hlongwa.mbu@gmail.com
Accepted 22 May 2019


{kind=link}