










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.13 n.2 Pretoria Jun. 2019
http://dx.doi.org/10.7196/sajch.2019.v13i2.1582
RESEARCH
Mortality and morbidity of very low-birthweight and extremely low-birthweight infants in a tertiary hospital in Tshwane
R M TshehlaI; M CoetzeeII; P J BeckerIII
IMB ChB, DCH (SA); Department of Paediatrics and Child Health, Steve Biko Academic Hospital, and the Faculty of Health Sciences, University of Pretoria, South Africa
IIMB ChB, DCH (SA), FCPaed, MMed (Paed), Cert Neonatol (SA), MPhil; Division of Neonatology, Department of Paediatrics and Child Health, Steve Biko Academic Hospital, and the Faculty of Health Sciences, University of Pretoria, South Africa
IIIMSc, PhD; Research Office, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND. Since 2000, South Africa (SA) has had a relatively static neonatal mortality rate, estimated to be 12/1 000 live births, with complications of prematurity being the leading cause of neonatal mortality. Survival to hospital discharge of small infants has improved over the last few decades; however, this is more marked in developed countries where neonatal intensive care, nasal continuous positive airway pressure, mechanical ventilation and surfactant are available to the majority of infants.
OBJECTIVES. The primary objective was to determine overall mortality of very low-birthweight and extremely low birthweight (ELBW) infants in the neonatal unit at Steve Biko Academic Hospital (SBAH). Secondary objectives were to determine the frequency of major morbidities, identify factors associated with morbidity and mortality, determine survival without major morbidity, and whether birthweight can accurately predict outcome.
METHODS. This was a retrospective cross-sectional study of infants with a birthweight of 500 - 1 499 g who had been admitted to the neonatal unit of SBAH between June 2016 and May 2017.
RESULTS. Overall survival to hospital discharge was 75.7%, with only 17.7% of infants weighing <750 g surviving. Survival without major morbidity was 35.1%. Small-for-gestational age, invasive ventilation, and culture-positive early-onset sepsis were associated with an increased risk of mortality, whereas higher birthweight and the use of nCPAP decreased mortality in multivariable analysis.
CONCLUSION. Although the overall survival of infants weighing <1 500 g is comparable to other large SA public hospitals, survival of ELBW infants is poor, while these are the infants that require the most interventions, placing a heavy burden on limited resources. However, it remains difficult to recommend a cut-off weight for potentially life-saving interventions.
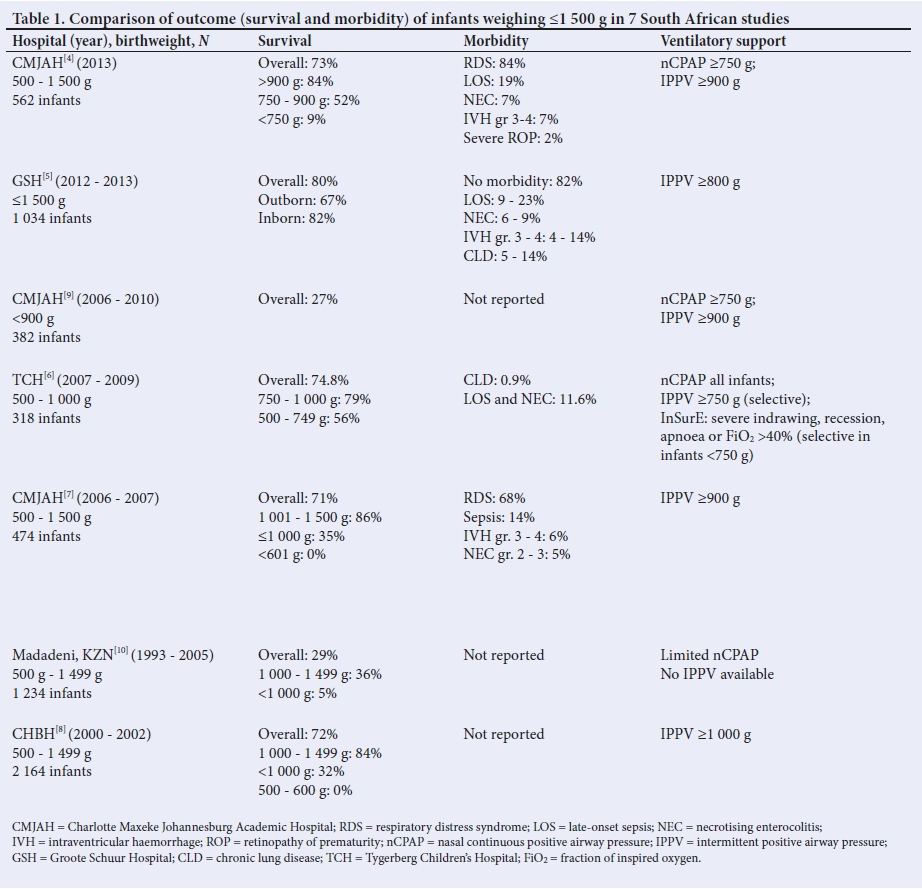
Since 2000, South Africa (SA) has had a relatively static neonatal mortality rate,[1] estimated to be 12/1 000 live births in 2016,[2] with complications of prematurity being the leading cause of neonatal mortality.[1] Very low-birthweight (VLBW) and extremely low-birthweight (ELBW) infants have the highest risk for mortality and morbidity. While survival to hospital discharge has improved over the last few decades, this is more marked in developed countries where neonatal intensive care (NICU), nasal continuous positive airway pressure (nCPAP), mechanical ventilation and exogenous surfactant are available to the majority of infants. VLBW and ELBW infant survival to hospital discharge was reported to be 85% and 72%, respectively, in the USA.[3] While the mortality in this group of infants has decreased in developing countries, it remains higher than in developed countries. Limited resources of life-saving interventions such as respiratory support and exogenous surfactant are contributory to the higher mortality. Studies performed at public hospitals in SA between 2000 and 2013 report rates of survival to hospital discharge of 71 - 80% in infants <1 500 g (Table 1).[4-8] In SA, survival of infants weighing 1 000 - 1 500 g is as high as 84 -86% in some facilities.[7,8] Notably, survival of ELBW infants in these two facilities were only 32 - 35%.[7,8] This contrasts with a study performed at Tygerberg Children's Hospital (TCH) in Cape Town, which reported 75% survival in infants 500 - 1 000 g who received nCPAP as standard care with administration of surfactant when indicated.[6] Hence, the degree of intervention provided to ELBW infants seems to be a predictor of outcome.
Birth weight and gestational age (GA) are reported as independent predictors of mortality.[7] Emergency caesarean section (CS) delivery, being outborn, resuscitation at delivery, small-for-gestational age (SGA), and hypothermia on admission are also associated with increased mortality.[5,7] Factors associated with improved survival include maternal attendance of antenatal care (ANC), delivery in a tertiary centre, and female gender.[5,7] Maternal risk factors for preterm birth include previous CS, previous miscarriage, previous preterm delivery, anaemia, bacterial vaginosis, and hypertension.[11,12]
Improved survival of VLBW and ELBW infants has resulted in increased morbidity, including necrotising enterocolitis (NEC), intraventricular haemorrhage (IVH), periventricular leucomalacia (PVL), patent ductus arteriosus (PDA), retinopathy of prematurity (ROP) and sepsis. In SA, the reported incidence of ROP, IVH and PVL is probably an underestimation as a large number of infants are still not screened for these conditions due to lack of resources. Maternal ANC and antenatal corticosteroids (ACS) improve the chance of survival without major morbidity.[5]
This study aims to evaluate the morbidity and mortality of VLBW and ELBW infants in the neonatal unit at Steve Biko Academic Hospital (SBAH). The findings in this study may be of value in establishing policies on the rationing of limited resources.
Methods
Study design and setting
A retrospective, cross-sectional study was performed in the neonatal unit of SBAH, between 1 June 2016 and 31 May 2017. SBAH is a tertiary care public hospital in Tshwane with a 39-bed neonatal unit, consisting of 10 neonatal ICU beds (reserved mainly for invasive and non-invasive ventilation) and 29 high-care and low-risk beds. This unit provides care for high-risk inborns, as well as infants referred from other hospitals within the Tshwane Metropolitan Municipality, and occasionally from other provinces (Mpumalanga and Limpopo), who require specialised care. Infants with both medical and surgical conditions are managed in this unit.
During the period of this audit, SBAH neonatal unit had no official policy regarding allocation of the limited resources, such as NICU admission and ventilation (invasive and non-invasive). The first-line management of infants with respiratory distress syndrome (RDS) weighing >750 g was nCPAP, followed by rescue surfactant therapy when indicated, with the provision of invasive ventilation being determined on an individual basis in infants of 750 - 999 g. Infants weighing >1 000 g were offered invasive ventilation when necessary (apnoea, worsening respiratory distress or respiratory failure). Although decisions regarding the level of care offered to infants weighing <750 g was determined individually, considering the available resources and clinical condition, all infants were offered standard neonatal care - including supplemental low-flow oxygen, intravenous fluids and thermoregulation - irrespective of birth weight. Indications for rescue surfactant therapy included ongoing or worsening respiratory distress (recession, grunting or tachypnoea) or a fraction of inspired oxygen (FiCy >30 - 40% (dependent on clinical picture and GA), despite the provision of nCPAP. Methods of administering surfactant included LISA (less invasive surfactant administration) and InSurE (intubate, surfactant, extubate). High-flow oxygen therapy was not available in the unit.
Study population and definitions
Infants weighing 500 - 1 499 g who were admitted to the neonatal unit at SBAH, including infants who died in theatre or the labour ward, those born before arrival to hospital (BBA), and infants born at another facility and transferred into the unit, irrespective of postnatal age at the time of transfer, were included in the study. Stillborn infants and those with congenital abnormalities with an expected poor prognosis, chromosomal abnormalities, and those previously discharged home were excluded from the study. GA was determined from the best estimate available in the clinical record, including last normal menstrual period, early ultrasound (<24 weeks gestation) and Ballard score.'131 Birth weight was plotted against GA on Fenton growth charts'141 to determine growth parameters. Infants were considered SGA if the weight plotted below the 10th percentile.'151 Resuscitation at birth included any positive-pressure ventilation, cardiac compression or the administration of adrenaline. All infants weighing <1 500 g were eligible for cranial ultrasound and RCP screening according to the unit policy. All cranial ultrasounds were performed by a trained sonographer. RCP was diagnosed by an opthalmologist. First screening was performed at 31 to 33 weeks GA or 4 to 6 weeks chronological age, if the gestation was uncertain.[16] Grading of severity (stage 1 - 5) was done according to the international classification of RCP.[16]For the purpose of this study, only sonographically confirmed IVH (graded according to Papile)[17] and radiographically confirmed NEC (Bell's stage 2 and 3)[18] were included. These diagnoses were confirmed by the primary author (RMT) by reviewing cranial ultrasound reports and abdominal radiographs, respectively. BPD diagnosis (supplemental oxygen for >28 days) and the severity grading[19] was confirmed by the primary author (RMT) using the information available in the patient records. The diagnosis of culture-positive or suspected sepsis was made by the attending doctor, and confirmed by the first author (RMT) by reviewing the results of blood investigations. Early-onset sepsis (ECS) was defined as sepsis occuring before 72 hours, and late-onset sepsis (LCS) after 72 hours of life.
Study procedure
Patients were identified using admission statistics. Records were retrieved and appropriate data collected. Laboratory results were accessed from the National Health Laboratory Service (NHLS) database. Cranial ultrasound reports and abdominal radiographs were viewed on the computerised record system (Xeroviewer).
Data analysis
An estimated sample of 250 infants was required. Maternal and infant data regarding demographics, outcome and morbidity were collected and analysed using Stata version 14.2 (StatCorp., USA). Maternal data were captured per infant, and wre therefore duplicated for women with a multiple pregnancy. Data were summarised using descriptive statistics such as means, standard deviations, medians, ranges, percentages and 95% confidence intervals. Percentages were calculted using the number of valid cases per variable as the denominator, i.e. cases for whom information about the variable was available.
Where data were skewed, median values were reported rather than mean. Crude odds ratios (CRs) for mortality and morbidity were assessed using logistic regression. For association in the case of continuous variables, the Student i-test or Wilcoxon rank-sum test was employed. Testing was done at a significance level of 0.05. A multivariable analysis with variables associated with mortality at the 0.15 level of significance was done using multivariable logistic regression. The latter was repeated using multivariable Cox regression, i.e. taking time to event into consideration. A prediction model for mortality using birth weight was attempted.
Ethics
Ethical approval was obtained from the Research Ethics Committee at the Faculty of Health Sciences of the University of Pretoria (ref. no. 210/2017).
Results
Study cohort
A total of 240 live-born infants weighing 500 - 1 499 g were admitted to the SBAH neonatal unit during the 1-year study period. Six infants were excluded from the study as per protocol, as they had congenital abnormalities (2 infants had duodenal atresia, 1 infant jejunal atresia, 1 infant imperforate anus, 1 infant trisomy 18, and 1 infant tracheoesophageal fistula and transposition of the great arteries). A further 3 infants were excluded as their records could not be traced. A total of 231 infants were eligible for inclusion.
Maternal characteristics
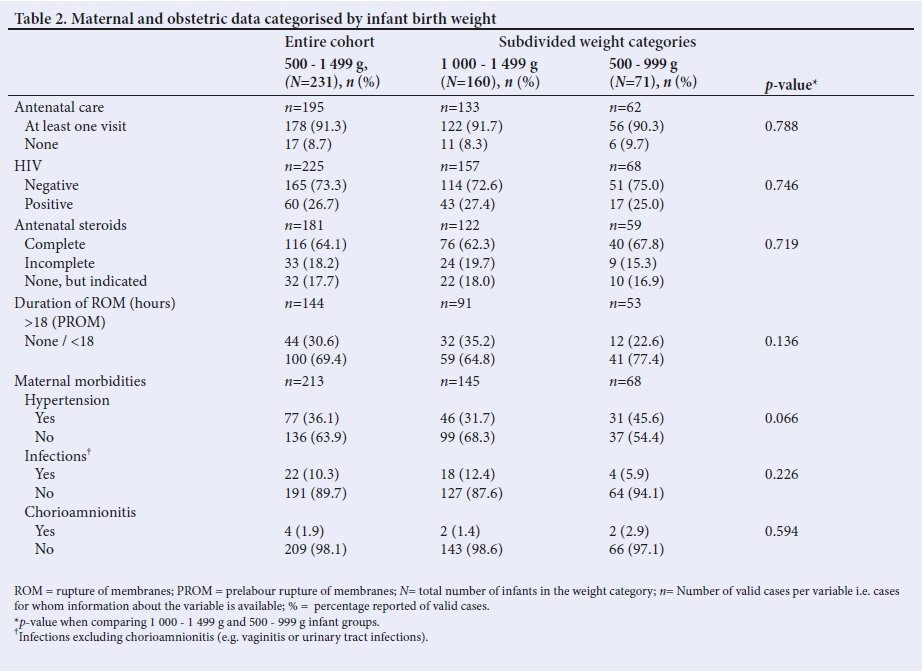
The mean (standard deviation (SD)) maternal age was 29 (6) years. Overall, 91.3% (n=178/195) of women attended ANC. Approximately one-quarter (26.7%; n=60/225) of women were HIV-positive, with 89.7% (n=52/58) of these women receiving lifelong combined antiretroviral therapy (cART) during pregnancy. Of the women receiving cART, 76.5% (n=39/51) received cART >4 weeks prior to delivery and 85% (n=34/40) had a HIV viral load <1 000 copies/mL. Approximately 80% (n=149/181) of women received ACS; however, only 64.1% of women completed the course, and 17.7% of women did not receive any ACS despite preterm labour before 34 weeks. Prolonged rupture of membranes (PROM) greater than 18 hours was present in 30.6% (n=44/144) of pregnancies. Co-morbidities included hypertension in 36.1% (n=77/213), infection (vaginitis or urinary tract infection) in 10.3% (n=22/213), and chorioamnionitis in 1.9% (n=4/213). Additionally, 6 women were diagnosed with tuberculosis (TB) during pregnancy. Significantly more women delivering ELBW infants had a previous miscarriage (35.8%; n=24/67) compared with women delivering infants weighing 1 000 - 1 499 g (p=0.046). Maternal age, ANC, HIV status, cART use and duration, ACS, hypertension, PROM, TB, infections and chorioamnionitis were similar between infants weighing 500 - 999 g and 1 000 - 1 499 g (Table 2).
Infant characteristics
The overall mean (SD) birth weight for the 231 infants was 1 117 (240) g, of whom 160 infants (69.3%; n=160/231) weighed 1 000 -1 499 g (mean (SD) 1 247 (151) g) and 71 infants (30.7%; n=71/231) weighed 500 - 999 g (mean (SD) 823 (106) g). Of the ELBW infants, 54 (23.4%) weighed 750 - 999 g and 17 (7.3%) weighed <750 g. The overall mean (SD) GA was 29.6 (2.6) weeks. Half of the infants (49.6%; n=111/224) were SGA, with significantly more SGA infants (p<0.001) weighing 500 - 999 g (75.0%; n=51/68) compared with 1 000 -1 499 g (38.5%; n=60/156).
Infant characteristics and comparison between weight groups are shown in Table 3. The majority of infants were inborn (82.6%; n=190/230), with significantly fewer outborn infants weighing <1 000 g (p=0.007). CS was the predominant mode of delivery (52.3%; n=113/216) and 84.1% (n=190/226) of infants were singletons. Resuscitation was required in 39.5% (n=88/223) of deliveries, with significantly more ELBW infants requiring resuscitation compared with infants weighing 1 000 - 1 499 g (50% v. 34.6%, respectively; p=0.038). Overall, three-quarters of the infants (76.4%; n=162/212) were hypothermic on admission (temperature <36.5°C): 93.8% of infants weighing <750 g, 84.6% of infants weighing <1 000 g and 72.8% of infants weighing 1 000 - 1 499 g. These differences were not significant. The majority of infants (90.9%; n=180/198) received only breastmilk during admission. Sixty infants were HIV-exposed with all early HIV-PCR tests negative. The overall median length of hospital stays (until death or discharge) was 19 days (range 0 - 114 days) compared with 25 days (range 4 - 114 days) for survivors. Surviving infants weighing <750 g had the longest hospital stays (65.5 days, range 15 - 114 days) compared with those weighing 750 - 999 g (60.5 days; range 15 - 114 days) and 1 000 -1 499 g (21 days, range 4 - 112 days). Infants who survived spent a median of 6 days (range 1 - 85 days) in NICU, and those weighing <750 g had the longest NICU stay (13 days, range 9 - 17 days).
The majority of infants received rescue surfactant (59%; n=128/217), with 35% (n=76), 20.7% (n=45), and 3.2% (n=7) of infants receiving 1, 2 and 3 doses, respectively. Significantly more ELBW infants received surfactant compared with those weighing 1 000 - 1 499 g (75.8% v. 51.7%; p=0.001). Additionally, a second or third dose was required more often in ELBW infants compared with infants weighing 1 000 - 1 499 g (39.4% v. 17.2%, respectively). nCPAP, conventional ventilation (CV) and high-frequency oscillation ventilation (HFOV) were offered to 81.3% (n=178/219), 30.6% (n=67/219) and 2.3% (n=5/219) of the infants, respectively. The median duration of nCPAP support for all infants (until death or discharge) was 3 days (range 1 - 45 days), and for surviving infants weighing 1 000 - 1 499 g, 750 - 999 g, and <750 g it was 2 days (range 1 - 30 days), 6 days (range 1 - 45 days), and 9.5 days (range 7 - 12 days), respectively. The median duration of CV was 3 days (range 1 - 33 days), with more infants weighing 750 - 999 g receiving CV (36%; n=18/50) compared with infants weighing 1 000 - 1 499 g (29.4%; n=45/153) and <750 g (25%; n=4/16); however, this difference was not significant (p=0.647). All infants who received HFOV died (n=5/219). The overall median duration of supplemental oxygen administration was 5 days (range 1 - 111 days), with surviving infants <1 000 g receiving oxygen for 17.5 days (range 1 - 111 days), and infants <750 g for 39.5 days (range 34 - 45 days) (Table 3).
Infant morbidity
Table 4 summarises the major causes of infant morbidity. One-quarter of infants (24.6%; n=45/183) developed IVH, with 14.8% (n=27), 1.6% (n=3), 3.3% (n=6) and 4.9% (n=9) having grade 1 to 4, respectively. There was a trend towards more infants weighing <750 g developing severe IVH (grade 3 and grade 4); however, this was not significant (p=0.650). There was no significant association between IVH and the method of delivery (p=0.380), ACS (p=0.750), resuscitation at birth (p=0.157), or hypothermia on admission (p=0.642).
Six infants were diagnosed with NEC during admission, of whom 3 had grade 2 and 3 had grade 3 NEC. There was no difference in the occurance of NEC in infants weighing 1 000 -1 499 g and 500 -999 g (p=0.501). Exclusive formula feeding was the only significant risk factor for developing NEC (p=0.030).
BPD was diagnosed in 11.8% (n=26/220) of infants, with 5.5% (n=12) having mild, 3.2% (n=7) moderate and 3.2% (n=7) severe BPD. The odds of developing BPD were 2.5-times higher in infants weighing 750 - 999 g (p=0.038; 95% CI 1.02 - 6.12), compared to those 1 000 - 1 499 g. The only significant risk for BPD in this study was the need for surfactant, which increased the odds 9-times (p<0.001; 95% CI 2.0 - 41.3). Maternal ACS and the use of nCPAP did not protect against BPD, nor did invasive ventilation increase the odds of developing BPD.
Only 54.1% (n=125/231) of infants were screened for ROP, of whom 5.6% (n=7) had ROP. Three infants had grade 1, 1 infant had grade 2, and 3 infants had grade 3 ROP. The distribution of ROP between infants weighing 1 000 - 1 499 g and 500 - 999 g was similar (p=0.395). Infants with ROP received oxygen for 16.9 days longer than those without ROP; however, this was not significant (p=0.075).
EOS and LOS were documented in 21.3% (n=49/230) and 28.3% (n=65/230) of infants, of which 20.4% (n=10) and 47.7% (n=31) were culture-positive, respectively. Significantly more ELBW infants had culture-positive EOS compared with infants weighing 1 000 -1 499 g (p=0.033); however, there was no difference regarding LOS (p=0.423). Chorioamnionitis increased the odds of developing EOS 11.5-imes (p=0.009; 95% CI 1.1 - 118.5) and prolonged rupture of membranes increased the odds 2.7-imes (p=0.013; 95% CI 1.2 - 6.0). HIV exposure did not increase the odds of developing EOS or LOS. Infants with LOS spent 22 days longer in the neonatal unit (p<0.001; 95% CI 14.2 - 29.9), and 6.8 days longer in NICU (p<0.001; 95% CI 3.5 - 10.0). Feeding choice and hypothermia did not increase the odds of developing LOS (Table 4).
Infant mortality
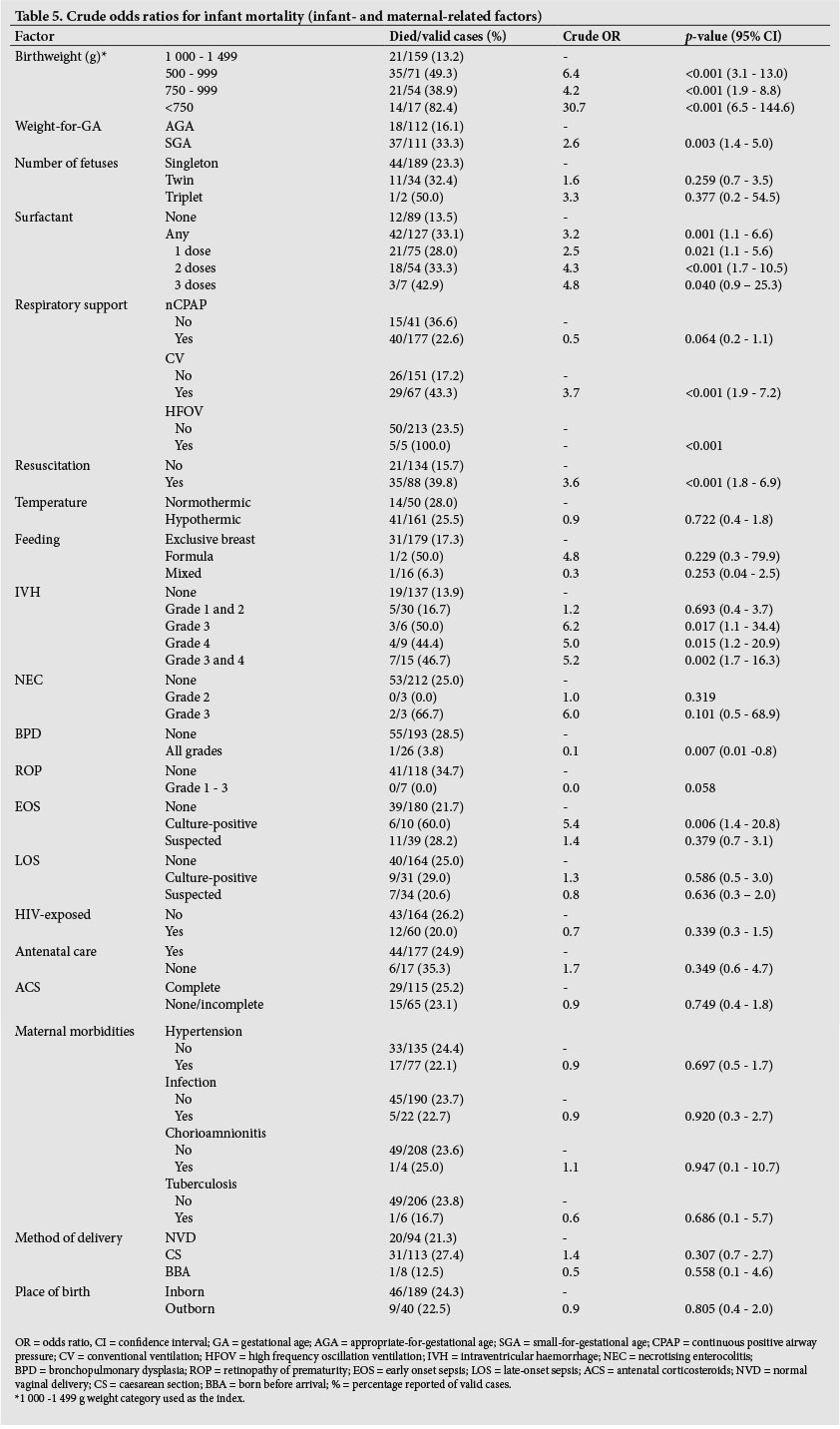
The overall survival for infants weighing 500 - 1 499 g was 75.7% (n=174/230). Table 5 summarises data and risks related to infant mortality. Eighty-seven percent (n=138/159) of infants weighing 1 000 - 1 499 g survived, compared with 50.7% (n=36/71) of infants <1 000 g (p<0.001). Significantly more infants weighing 750 - 999 g survived compared with those weighing <750 g (61.1% v. 17.6%, respectively; p<0.001). The mean (SD) birth weight of surviving infants was 1 178 (208) g and that of infants who died was 925 (234) g. The odds of death were increased 6.4 times in infants <1 000 g (p<0.001; 95% CI 3.1 - 13.0) and 30.7 times increased in infants <750 g (p<0.001; 95% CI 6.5 - 144.6) when compared with infants weighing 1 000 - 1 499 g. Therefore, birth weight was modelled as a predictor for mortality and, although survival clearly improved with increasing birth weight, no weight cut-off was a good predictor of outcome statistically. SGA infants had 2.6 times increased odds of death (p=0.003; 95% CI 1.4 - 5.0). Requiring resuscitation at delivery increased the odds of death 3.6 times (p<0.001; 95% CI 1.8 - 6.9). Infants who received exogenous surfactant had 3.2times increased odds of death (p=0.001; 95% CI 1.5 - 6.6), with the odds increasing for each additional dose of surfactant (p<0.001). CV had 3.7 times increased odds of death (p<0.001; 95% CI 1.9 - 7.2) and the use of HFOV predicted death in this study (p<0.001). The use of nCPAP improved outcome (OR 0.5), although this was not significant (p=0.064). Culture-positive EOS and severe IVH increased the odds of death 5.4 times (p=0.006; 95% CI 1.4 - 20.8) and 5.2times (p=0.002; 95% CI 1.7 - 16.3), respectively; while BPD was associated with decreased odds of death (OR 0.10; p=0.007; 95% CI 0.01 - 0.8).
Maternal ANC, ACS, infections (including chorioamnionitis and TB), PROM, place of birth, mode of delivery, multiple pregnancy, hypothermia on admission, feeding choice, NEC, ROP, HIV exposure, and LOS had no significant association with infant mortality. Infants of mothers with hypertension seemed to have a better outcome with an odds ratio of 0.9, although this was not significant (p=0.697) (Table 5).
Multivariable analysis
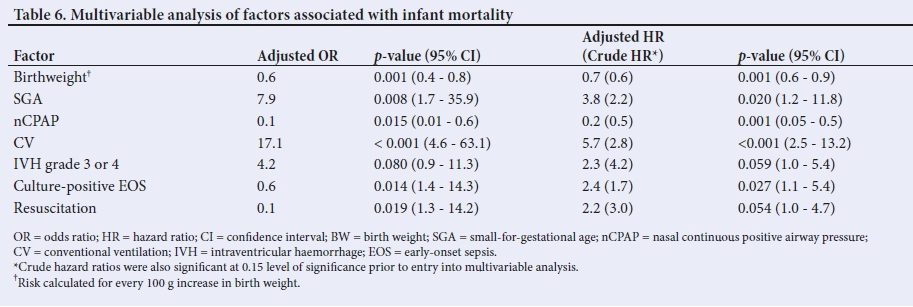
Multivariable logistic regression and Cox regression analysis of factors shown to affect survival at a significance level of 0.15 was done (Table 6). Birthweight was found to significantly improve survival for every 100 g increase in birth weight (OR 0.6; p=0.001; 95% CI 0.4 - 0.8 and HR 0.7; p=0.001; 95% CI 0.6 - 0.9). SGA was associated with mortality (OR 7.9; p=0.008; 95% CI 1.7 - 35.9 and HR 3.8; p=0.020; 95% CI 1.2 - 11.8), as was culture-positive EOS and CV (OR 4.4; p=0.014; 95% CI 1.4 - 14.3 and HR 2.4; p=0.027; 95% CI 1.1 - 5.4; and OR 17.1; p<0.001; 95% CI 4.6 - 63.1 and HR 5.7; p<0.001; 95% CI 2.5 - 13.2; respectively). The need for resuscitation at delivery increased mortality on logistic regression; however, this was marginally insignificant on Cox regression (OR 4.2; p=0.019; 95% CI 1.3 - 14.2 and HR 2.2; p=0.054; 95% CI 1.0 - 4.7). The use of nCPAP was protective (OR 0.1; p=0.015; 95% CI 0.01 - 0.6 and HR 0.2; p=0.001; 95% CI 0.05 - 0.5). Severe IVH was no longer associated with mortality using logistic regression; however, was only marginally insignificant on multivariable Cox regression (Table 6).
Survival without major morbidity
Of the 231 infants, 94 had complete data for all major morbidities (IVH, NEC, BPD, ROP or sepsis), and the 137 with missing data were excluded from this analysis. Survival without major morbidity was 35% (n=33) overall. Survival without major morbidity in infants weighing 1 000 - 1 499 g and infants weighing <1 000 g was 39% (n=26/67) and 26% (n=7/27), respectively. No infant (n=0/2) weighing <750 g survived without major morbidity.
Discussion
Three-quarters of VLBW infants admitted to SBAH neonatal unit survived to hospital discharge. Multivariable analysis showed that a higher birth weight was associated with improved survival, with 86.6%, 50.7% and 17.6% of infants weighing 1 000 - 1 499 g, <1 000 g and <750 g surviving to discharge, respectively. The mean birth weight of surviving infants was ~250 g greater than those who died; however, no cut-off weight demonstrated good sensitivity and specificity for predicting mortality in this or other studies.
Availability of resources, such as exogenous surfactant and ventilation (invasive and non-invasive), are additional factors that affect outcome. In this study, 75% (n=12/16) of infants <750 g and 85% (n=55/65) of infants <1 000 g received nCPAP, while a third (n=22/66) of infants <1 000 g received invasive ventilation. Multivariable analysis showed that invasive ventilation was associated with increased mortality, compared with nCPAP use, which was associated with decreased mortality. This effect may be explained by the fact that infants requiring invasive ventilation probably had more severe disease compared with those requiring only nCPAP support. Although rescue surfactant administration has been shown to improve survival, this association was not replicated in this study.
Only one-third of infants in this study survived to discharge without major morbidity. The most common major morbidity was LOS (28.3%), followed by IVH (24.6%), EOS (21.3%), BPD (11.8%), ROP (5.6%), and NEC (2.7%). LOS is an increasing healthcare challenge with a negative impact on survival, although there was no significant association between LOS (culture-positive or suspected) and mortality in this study. However, infants with LOS remained in hospital and NICU longer than those without sepsis in this study. For these reasons, measures to prevent LOS including hand-washing, prevention of overcrowding, and exclusive breastfeeding should still be reinforced in the neonatal unit. Conversely, culture-positive EOS was associated with increased mortality in this study; however, this may be confounded by the fact that culture-positive EOS occurred more frequently in infants weighing <1 000 g, compared with 1 000 - 1 499 g (10% v. 2%). Chorioamnionitis and PROM significantly increased the odds of developing EOS.
Severe IVH (grade 3 and 4) was associated with increased mortality in the univariable analysis in this study; however, no risk factors for the development of IVH were identified. The odds of developing BPD were the highest in infants weighing 750 - 999 g compared with other weight groups, which may reflect improved lung maturity of bigger infants (1 000 - 1 499 g) and increased mortality before 28 days of life in smaller infants (<750 g). Contrary to other studies, invasive ventilation did not increase the risk, and nCPAP and maternal ACS did not decrease the risk of developing BPD in this study. Surprisingly, infants who received surfactant had increased odds of developing BPD in this study; however, surfactant administration was likely a marker of less mature lungs and not directly related to the development of BPD.
Although NEC was not associated with an increased risk for mortality in this study, it must be highlighted that other studies report an increased risk of death, and therefore simple measures such as exclusive breastfeeding should be emphasised to prevent NEC. Similarly, contrary to other studies, no risk factors for ROP could be identified in this study (including prolonged supplemental oxygen administration).
Maternal ACS have been shown to improve outcomes in preterm infants. However, they did not decrease the length of supplemental oxygen administration or ventilatory support, nor did it decrease major morbidities such as severe IVH, NEC or BPD in this study. Similary, maternal ANC and hypertension did not influence infant outcome in this study.
Study limitations
By virtue of the retrospective design, this study has various limitations. The study population of 231 infants was near the required sample of 250 infants and, although few infants were excluded (n=9/240), incomplete data recorded in clinical records and poor adherence to screening protocols resulted in large gaps in the data set, particulary for the evaluation of survival without morbidity. Consequently, IVH and ROP were probably under-reported in this study. Similarly, NEC may have been under reported as only infants with radiographic evidence of NEC were included, excluding all infants with grade 1 NEC and those who may have died before an abdominal radiograph was taken.
Additionally, diagnoses were provided by different levels of healthcare professionals; although the first author (RMT) attempted to verify the accuracy of all collected data.
Conclusion
The overall survival for VLBW infants in this study is comparable to similar studies done in SA;[4,5,7,8] however, it is still lower than the survival reported in the USA.[3] The survival of ELBW infants in this study is higher than some other SA studies;[7,8,10] however, it is lower than that achieved by TCH in Cape Town[6] (50.7% v. 75%), with the most striking difference in survival noted in infants <750 g (17.6% v. 56%). Although the availability of resources affects survival, the practice of early nCPAP and rescue surfactant administration, as opposed to routine intubation and ventilation, is recommended practice for preterm infants with RDS, and the limited availability of invasive ventilation in this neonatal unit is minimally restrictive in this sense. Despite the burden that ELBW infants place on limited resources while having a poorer outcome, it remains difficult to recommend a cut-off weight for potentially life-saving interventions such as nCPAP and surfactant. However, the current practice of allocating resources based on availability to infants with an expected favourable outcome is supported by the results in this study. While the solutions to resource limitations are complex, inexpensive measures, including improved neonatal resuscitation skills, prevention of hypothermia, infection prevention and control measures, exclusive breastfeeding, and kangaroo mother care, can be encouraged to improve the outcome of these infants.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgements. None.
Author contributions. RMT and MC conceptualised the research project. PJB did the statistical planning and performed the data analysis. RMT collected and managed all data. RMT, MC and PJB interpreted the data after analysis. RMT and MC drafted the article. PJB revised the article for scientific content and statistical accuracy. All authors approved the final version for publication.
Funding. None.
Conflicts of interest. None.
References
1. Rhoda NR, Velaphi S, Gebhardt GS, Kauchali S, Barron P. Reducing neonatal deaths in South Africa: Progress and challenges. S Afr Med J 2018;3(Suppl 1):S9-S16. https://doi.org/10.7196/SAMJ.2018.v108i3.12804 [ Links ]
2. Dorrington RE, Bradshaw D, Laubscher R, Nannan N. Rapid mortality surveillance report 2016. Cape Town: South African Medical Research Council, 2016. http://www.mrc.ac.za/sites/default/files/files/2018-02-22/RapidMortalitySurveillanceReport2016.pdf (accessed 2 July 2018). [ Links ]
3. Eichenwald EC, Stark AR. Management and outcomes of very low birth weight. N Engl J Med 2008;358(16):1700-1711. https://doi.org/10.1056/NEJMra0707601 [ Links ]
4. Ballot DE, Chirwa T, Ramdin T, et al. Comparison of morbidity and mortality of very low birth weight infants in a central hospital in Johannesburg between 2006/2007 and 2013. BMC Pediatr 2015;15:20. https://doi.org/10.1186/s12887-015-0337-4 [ Links ]
5. Gibbs L, Tooke L, Harrison M. Short-term outcomes of inborn v. outborn very-low-birth-weight neonates (<1 500 g) in the neonatal nursery at Groote Schuur Hospital, Cape Town, South Africa. S Afr Med J 2017;107(10):900-903. https://doi.org/10.7196/SAMJ.2017.v107i10.12463 [ Links ]
6. Kirsten GF, Kirsten CL, Henning PA, et al. The outcome of ELBW infants treated with NCPAP and InSurE in a resource-limited institution. Pediatrics 2012;129(4):e952-959. https://doi.org/10.1542/peds.2011-1365 [ Links ]
7. Ballot DE, Chirwa TF, Cooper PA. Determinants of survival in very low birth weight neonates in a public sector hospital in Johannesburg. BMC Pediatr 2010;10:30. https://doi.org/10.1186/1471-2431-10-30 [ Links ]
8. Velaphi SC, Mokhachane M, Mphahlele RM, Beckh-Arnold E, Kuwanda ML, Cooper PA. Survival of very-low-birth-weight infants according to birth weight and gestational age in a public hospital. S Afr Med J 2005;95(7):504-509. [ Links ]
9. Kalimba EM, Ballot DE. Survival of extremely low-birth-weight infants. S Afr J Child Health 2013;7(1):13-16. https://doi.org/10.7196/SAJCH.488 [ Links ]
10. Bondi FS, Adhikari M. Improved survival of non-ventilated very-low-birth-weight infants at Madadeni Hospital, KwaZulu-Natal. S Afr J Child Health 2007;1(1):10-13. [ Links ]
11. Roy KK, Baruah J, Kumar S, Malhotra N, Deorari AK, Sharma JB. Maternal antenatal profile and immediate neonatal outcome in VLBW and ELBW babies. Indian J Pediatr 2006;73(8):669-673. [ Links ]
12. DiRenzo GC, Giardina I, Rosati A, et al. Maternal risk factors for preterm birth: A country-based population analysis. Eur J Obstet Gynecol Reprod Biol 2011;159(2):342-346. https://doi.org/10.1016/j.ejogrb.2011.09.024 [ Links ]
13. Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard Score, expanded to include extremely premature infants. J Pediatr 1991;119(3):417-423. https://doi.org/10.1016/S0022-3476(05)82056-6 [ Links ]
14. Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr 2013;13:59. http://doi.org/10.1186/1471-2431-13-59 [ Links ]
15. Battaglia FC, Lubchenco LO. A practical classification of newborn infants by weight and gestational age. J Pediatr 1967;71(2):159-163. https://doi.org/10.1016/S0022-3476(67)80066-0 [ Links ]
16. Visser L, Singh R, Young M, Lewis H, McKerrow N. Guideline for the prevention, screening and treatment of retinopathy of prematurity (ROP). S Afr Med J 2013;103(2):116-25. https://doi.org/10.7196/SAMJ.6305 [ Links ]
17. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1,500 gm. J Pediatr 1978, 92(4):529-534. https://doi.org/10.1016/S0022-3476(78)80282-0 [ Links ]
18. Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg 1978;187(1):1-7. [ Links ]
19. Jobe AH, Bancalari E. NICHD/NHLB/ORD Workshop Summary: Bronchopulmonary dysplasia. Am J Respir Criti Care Med 2001;163(7):1723-1729. https://doi.org/10.1164/ajrccm.163.7.2011060 [ Links ]
 Correspondence:
Correspondence:
M Coetzee
mel.coetzee@up.ac.za
Accepted 1 October 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}