










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.13 n.2 Pretoria Jun. 2019
http://dx.doi.org/10.7196/sajch.2019.v13i2.1572
RESEARCH
Non-invasive continuous positive airway pressure ventilation and high-flow nasal cannula oxygen therapy use in children without primary lung pathology: A prospective observational study
K BrowdeI; B M MorrowII
IMB BCh, FCPaed, MMed; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIPhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Non-invasive nasal continuous positive airway pressure (nCPAP) and high-flow nasal cannula oxygen therapy (HFNC) are non-invasive ventilation (NIV) modalities appropriate for children in developing countries. There is minimal literature describing nCPAP and HFNC use in children with respiratory compromise secondary to non-pulmonary disease.
OBJECTIVES. Th present study aimed to describe the characteristics and outcomes of children without primary lung pathology, who received nCPAP and HFNC during their admission to Red Cross War Memorial Children's Hospital, Cape Town, South Africa.
METHODS. This was a prospective observational study of routinely collected data, between August 2015 and January 2016. Primary and secondary outcome measures were NIV failure (progression to intubation and invasive ventilation) and paediatric intensive care unit (PICU) admission, respectively. Comparative statistics were conducted using Mann-Whitney U or t-tests. Data significantly associated with the primary and secondary outcomes on univariate analysis were entered into backward stepwise logistic regression models to determine independent predictive factors.
RESULTS. There were 31 cases of nCPAP and 1 case of HFNC use in 31 patients (median age 3.5 (interquartile range (IQR) 1.8 - 7.6) months). The majority (n=23; 71.9%) presented with primary diarrhoeal disease. There were 2 deaths (6.5%), 17 (53.1%) PICU admissions, and 5 (15.6%) cases received invasive ventilation (NIV failure). The median duration of hospital stay was 11.5 (IQR 6.0 - 17.5) days. Patients who failed NIV had lower admission SaO2 levels than those without treatment failure (95% (IQR 95 - 99) v. 100% (IQR 100 - 100); p=0.03). On multiple logistic regression, lower temperature (adjusted OR (aOR) 0.19; 95% confidence interval (CI) 0.05 - 0.78; p=0.02) and receiving inotropes in the emergency setting (aOR 23.05; 95% CI 1.64 - 325.06; p=0.02) were independently associated with PICU admission.
CONCLUSION. nCPAP was used clinically for the management of children with respiratory compromise secondary to non-pulmonary illnesses, particularly diarrhoeal disease. Larger controlled clinical studies are needed to determine the effectiveness and utility of nCPAP in this population. HFNC was not commonly used, and this modality requires further investigation in this population.
Non-invasive ventilation (NIV) refers to respiratory support provided by an external interface rather than an invasive airway such as an endotracheal tube or tracheostomy.[1] This form of ventilation is gaining popularity in adult and paediatric practice, as it might prevent the need for endotracheal intubation[2] and, in so doing, prevent complications associated with invasive mechanical ventilation.[3]
NIV has been well described in the adult population,[2,4] and is used in the management of adult respiratory failure, across all diagnostic categories.[5] Compared iht other forms of NIV in adults, high-flow nasal cannula oxygen therapy (HFNC) is associated with the lowest intubation rates and the best 90-day survival rate in those with respiratory failure.[6] NIV is also well established for use in the neonatal setting, in the management of all-cause respiratory distress and for the early stabilisation of premature and low-birthweight newborns[7] Despite fewer formal data supporting its use in infants and older children[1] NIV is becoming more popular in this setting, commonly used in the management of acute and chronic respiratory failure; status asthmaticus; hypoventilation syndromes; neuromuscular disorders and chronic upper airway obstruction; as well as the prevention of extubation failure[8-10]
In low- and middle-income countries, where mechanical ventilatory support cannot be provided to the majority of children owing to resource limitations, simple yet effective non-invasive methods of providing respiratory support should be considered to optimise clinical paediatric outcomes.[11] In this context, both nasal continuous positive airways pressure (nCPAP) and HFNC can be provided by stand-alone machines, and have been adapted for use in low-resource settings.[11]
nCPAP has been shown to be effective in the management of older children with bronchiolitis and other respiratory illnesses, and bubble CPAP specifically reduces mortality and treatment failure compared to low-flow oxygen[12-17] and has become a mainstay of treatment for many of these conditions. HFNC is also being used more frequently in older children[3] where it has been shown to be as effective as nCPAP for some conditions.[18]
nCPAP and HFNC are also recommended in the initial resuscitation of children with respiratory compromise or hypoxaemia associated with sepsis or septic shock[19] Despite these recommendations, data supporting the use of nCPAP or HFNC for patients in whom the primary pathology is non-pulmonary are scarce.
We found only one article which specifically investigated the use of nCPAP in the management of respiratory compromise caused by non-pulmonary disease, this in the setting of Dengue shock syndrome[20] Other studies have included heterogeneous populations, with sample sizes too small to allow meaningful subgroup analyses[21-28] To the best of our knowledge no other studies have systematically evaluated the use of nCPAP or HFNC therapy specifically in children with non-pulmonary causes of respiratory compromise.
Objectives
In light of the above, this study aimed to describe the use of HFNC and nCPAP in the management of children admitted to Red Cross War Memorial Children's Hospital (RCWMCH), Cape Town, South Africa (SA), with primary pathologies other than respiratory illness.
Methods
Setting
RCWMCH is a public tertiary and secondary level hospital in Cape Town, SA. It is the only stand-alone, specialist children's hospital dedicated entirely to paediatric care in sub-Saharan Africa. RCWMCH has a total of 275 beds (medical and surgical), of which 15 are high-care medical beds and 22 are in the paediatric intensive care unit (PICU). Currently, children on nCPAP and HFNC are managed both in high-care ward units and in the PICU.
Approximately 40 000 children per year are managed at RCWMCH. It is estimated that 360 children are admitted to the PICU and 1 200 to high-care units via the medical emergency unit (MEU) (MEU records) annually. Because of the highly specialised care available at RCWMCH, patients present with a wide variety of illnesses, but the majority of patients are admitted with acute infections, most commonly respiratory or gastrointestinal, depending on the season.
At RCWMCH, institutional guidelines recommend the use of nCPAP or HFNC, using a stand-alone Bubble-nCPAP device (Fisher & Paykel Healthcare, New Zealand) as the standard of care in children presenting in severe respiratory distress where intubation and mechanical ventilation is not urgently required. Patients are carefully monitored considering the potential effects of PEEP on venous return. The interface standardly used for nCPAP is the F&P FlexiTrunk (Fisher & Paykel Healthcare, New Zealand) midline interface and nasal prongs, while appropriately sized paediatric oxygen therapy nasal cannulae are used for HFNC (Fisher & Paykel Healthcare, New Zealand). Although pulmonary disease remains the primary indication for nCPAP or HFNC, these modalities are also used in the management of children with respiratory compromise related to multiple non-pulmonary aetiologies.
In our context, in the summer months, a large proportion of patients present to the emergency department with gastroenteritis and dehydration as their primary illness, with respiratory compromise occurring as a consequence of shock, hypokalaemia or severe metabolic acidosis. Respiratory compromise is also common in the face of septic shock or overwhelming sepsis. It is currently standard practice to consider using nCPAP/HFNC for respiratory support in such cases, despite the scarcity of supporting evidence.
Study design and period
This was a prospective, single-centre, observational study of routinely collected data between August 2015 and January 2016.
Participants
All children between 0 and 12 years who received nCPAP or HFNC as part of standard respiratory care, and in whom respiratory compromise was not caused by primary lung pathology, were included in the study.
Neonates requiring respiratory support for hyaline membrane disease (HMD) or other diseases of the newborn period, children receiving chronic/home-based nCPAP/HFNC, and children with cardiogenic pulmonary oedema were excluded from the study.
Ethics approval
Permission to conduct the study was obtained from the University of Cape Town's Faculty of Health Sciences Human Research Ethics Committee (ref. no. 141/2015) and written informed consent was obtained from parents/legal guardians. The study adhered to the provisions of the Declaration of Helsinki (2013).
Procedure
MEU admissions were reviewed daily by the researcher to identify eligible patients. Patients receiving nCPAP/HFNC therapy in the medical wards were screened for eligibility daily by the same researcher. Parents/caregivers were approached for consent after admission of their child but prior to the collection of data from the files. All parents approached gave consent.
Routinely collected admission data ere prospectively collected from clinical folders on all eligible patients, using a standardised data collection form. Outcome data were collected at discharge or after death from digital or paper-based hospital records.
Statistical analysis
Data were entered into an Excel spreadsheet and appropriate parametric or non-parametric descriptive analyses were conducted using Statistica version 12 (StaSoft Inc., USA), after testing for normality (Shapiro-Wilk W-test). Comparative statistics were conducted using Mann-Whitney U-tests for non-parametric data and t-tests for independent variables for normally distributed data, using failure of nCPAP/HFNC (progression to intubation and invasive ventilation) and PICU admission as categorical primary and secondary outcome measures. Mortality was a further planned secondary outcome measure, but was not further analysed owing to small numbers (n=2). Data found to be associated with the primary and secondary outcomes on univariate analysis (p<0.05) were entered into backward stepwise logistic regression models to determine independent predictive factors. A significance level of p<0.05 was used for this study.
Results
There were 31 cases of nCPAP and 1 case of HFNC use in 31 patients with an age range of 0.4 to 56.5 months (median age 3.5 (interquartile range (IQR) 1.8 - 7.6) months; 50% male). Twenty-three of the 32 cases (71.9%) presented with respiratory distress secondary to diarrhoeal disease or complications thereof. Of these, 18 (78.3%) presented with hypovolaemic shock and 12 (52.2%) required inotropic support. One patient was admitted twice, on both occasions with hypovolaemic shock and respiratory compromise associated with diarrhoeal disease. Seven of the 32 cases (21.9%) were admitted with septicaemia. Four of these 7 were shocked and only 1 required inotropes. One child was admitted with acute liver failure and metabolic acidosis with respiratory compensation and increased work of breathing and 1 with meningitis who was lethargic and required respiratory support. Both were in septic shock and initiated on nCPAP therapy. A total of 24 (75%) cases were shocked on admission. Thirteen of the 31 patients (41.9%) were HIV-exposed but uninfected, and 3 (9.7%) were HIV-infected.
The only patient who was treated with HFNC had diarrhoeal disease and Salmonella sepsis (without shock). HFNC was initiated on the basis of the patient clinically tiring.
One (3.2%) complication of NIV - nasal skin trauma related to pressure caused by the nCPAP interface - was documented.
Primary outcome
Five (15.6%) patients failed NIV and were intubated and mechanically ventilated. These included the patient with acute liver failure, two cases with diarrhoeal disease and 2 cases with septicaemia.
Secondary outcomes
Seventeen (53.1%) cases required ICU admission, with diarrhoeal disease (n=13); septicaemia (n=3); and acute liver failure (n=1). Two (6.5%) patients died. Both deaths occurred in children who presented with diarrhoeal disease and comorbid chronic illness. One patient had neuroblastoma and previous ventriculo-peritoneal shunt. He demised in the MEU before admission to high care or PICU but was given fluid boluses and started on nCPAP and inotropes as part of his emergency management. The second patient had congenital haemolytic uraemic syndrome (HUS) with chronic kidney disease and demised after a protracted hospital stay.
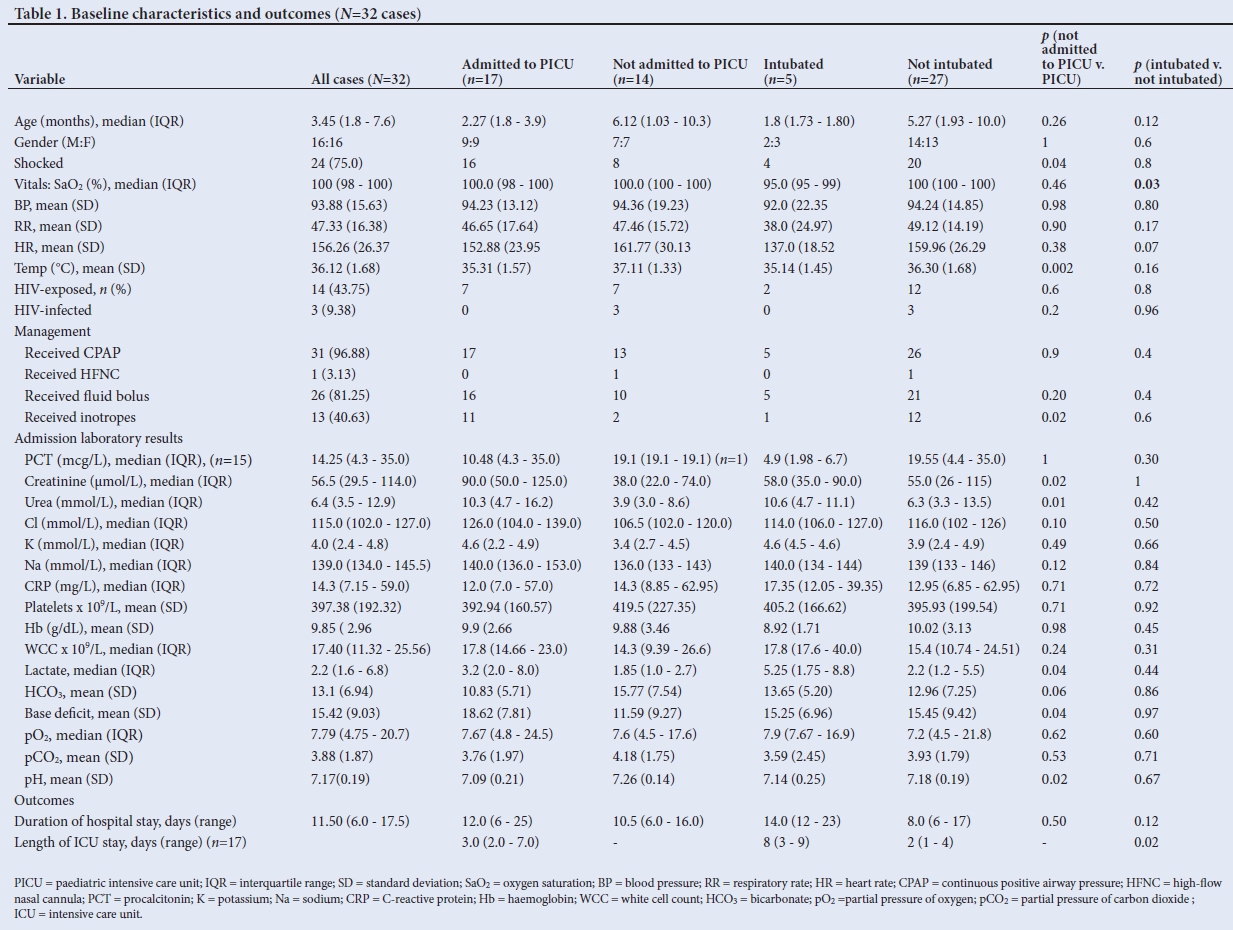
Table 1 presents univariate analyses of baseline characteristics and outcomes between primary and secondary outcome measures. Patients who failed NIV had lower presentation SaCh on univariate analysis. However, owing to insufficient patient numbers (only 5 failed NIV), we were unable to test this association on multiple logistic regression. Lower admission temperature (adjusted OR 0.19; 95% CI 0.05 - 0.78; p=0.02) and receipt of inotropes in the emergency setting (aOR 23.05; 95% CI 1.64 - 325.06; p=0.02) were independently associated with PICU admission.
Positive blood cultures within the first 3 days were obtained in 3 (9.3%) cases: 1 case each of Pseudomonas aeruginosa and coagulase-negative Staphylococcus aureus in patients who presented with diarrhoeal disease and 1 case of Streptococcus pneumoniae in a patient with septicaemia. The coagulase negative S. aureus was considered likely to have been a contaminant.
Two of the children with septicaemia had nasopharyngeal aspirate (NPA) specimens sent for respiratory viral panel analysis. These were both positive for respiratory syncytial virus (RSV) A and adenovirus, respectively. Four of the children with diarrhoeal disease had NPAs sent, of which 2 were positive for both adenovirus and rhinovirus, and 2 were negative. The patient with acute liver failure had a negative NPA.
Discussion
We report the results of an exploratory, observational study conducted in a single setting, in which nCPAP was used clinically in cases with respiratory compromise of non-pulmonary aetiology. HFNC was used in only 1 case in our cohort, for reasons that are unclear. To the best of our knowledge, there are no published data systematically describing the clinical use of nCPAP and HFNC in children admitted to hospital with respiratory compromise associated with primarily non-respiratory disease.
The vast majority (71.9%) of children receiving nCPAP/HFNC in this study presented with diarrhoeal disease (many with associated shock) requiring respiratory support. Globally, diarrhoeal disease is one of the leading causes of death in children under 5 years of age, responsible for more child deaths than AIDS, malaria and measles combined.[29] There is a particularly high burden of diarrhoeal disease in SA,[30] where an estimated 10 109 000 (54%) children live below the poverty line of ZAR671 (~$48) per month. In the Western Cape province, in 2013, ~486 000 (26%) children were living in income-poor households.[31] Diarrhoeal disease is responsible for 20% of child deaths under 5 years of age in SA.[32]
Considering the burden of disease, limited PICU resources, and poor access to paediatric healthcare centres in SA,[33] there is a need to identify safe, effective and affordable means of providing respiratory support to children with complications of diarrhoeal disease, sepsis, and other conditions outside the PICU setting. In this context, nCPAP and HFNC require further study, but are promising in terms of availability and affordability. A study from Malawi[34] showed that a stand-alone bubble nCPAP device could be developed for one-fifteenth of the price of the device recently approved by the Food and Drug Administration (FDA). In a recently published study conducted in Cape Town, SA, ventilatory management was identified as an important modifiable factor in the initial management of critically ill children presenting to city health clinics, which could impact on morbidity.[33] nCPAP and HFNC could feasibly be implemented at such centres. Although no definitive conclusions can be made on the basis of this study, and more research is needed, it is notable that 47% of children were spared PICU admission after nCPAP/HFNC therapy was provided in the ward high-care units. This finding may have important implications for low-resourced countries with little access to high-level PICU care.
The paediatric section of the 2012 Surviving Sepsis Campaign guidelines for treating sepsis and septic shock recommends the use of nCPAP or HFNC in the initial resuscitation of children with respiratory compromise or hypoxaemia associated with sepsis or septic shock.[19] Young children with severe sepsis or shock commonly require early respiratory support owing to low functional residual capacity. However, intubation and ventilation in these circumstances may cause harm by increasing intrathoracic pressure with resulting compromised venous return and worsening shock. HFNC and nCPAP could be effective in this setting, by increasing functional residual capacity and reducing work of breathing, thereby allowing for establishment of intravenous or intraosseous access for fluid resuscitation and peripheral inotrope delivery.[19] By reducing the need for intubation, the use of potentially harmful sedative drugs may also be avoided.
The 15.6% NIV failure rate is within the range (11.5% - 19%) described previously in children with sepsis.[22,25] In a prospective observational study investigating nCPAP use in 214 critically ill children in a resource-limited setting (India), Anitha et al.[22] found associated shock to be a risk factor for nCPAP failure, while Kelly et al.,[251in a retrospective review (n=498) found that those who failed NIV had presented with a higher venous pCO2, higher initial RR, and a lower venous pH than those in whom NIV was successful. Both these studies were limited by lack of control groups. On univariate analysis, Mayordomo-Colunga et al.,[35] in a prospective epidemiological study (N=116), found that smaller children were at higher risk of NIV failure. This did not remain a predictor on multivariate analysis. We were, however, unable to identify any predictive factors for NIV failure on the basis of such admission characteristics
The complication rate in this study was low, at 3%, but skin breakdown and pressure ulcers have been previously reported as complications of nCPAP.[1,35] Therefore care must be taken in applying the interface and frequently checking for pressure areas. Other complications of both nCPAP and HFNC which have been described include pneumothorax and other air-leak syndromes[28] abdominal distension, upper-airway bleeds[,35,36] and noise-induced hearing loss.[37]
In our setting PICU admission is largely dependent on resources and availability of PICU beds, therefore not being admitted to PICU does not necessarily always reflect lower acuity of illness. However, we found that lower admission body temperature and the receipt of inotropes were independent predictors of PICU admission, possibly reflecting higher severity of illness in these patients. Studies have shown that scoring systems such as the Pediatric Early Warning Systems (PEWS), which include assessment of temperature and blood pressure, may be able to predict the need for a higher level of care when they are used in the emergency department.[38] Research is warranted in our setting to determine the utility of such scoring systems to timeously recognise children who may require PICU admission and increased levels of support.
Study limitations
This was a single-centre study with a small sample size, and no control group. Therefore, the actual prevalence of HFNC/nCPAP in this population cannot be determined. However, the sample size is comparable with that of previous studies of NIV use in children.[2-23] Randomised controlled trials with larger, homogeneous study populations are needed to establish the safety and efficacy of nCPAP and HFNC in the management of children with diarrhoeal disease, and other non-pulmonary diseases.
Having had only one researcher to recruit patients throughout the study period, there is a possibility that eligible patients might have been missed. It is possible that children had co-existing, but undiagnosed, respiratory pathology, which might have confounded the results of this study and contributed to patients' respiratory distress. The positive viral screens in a number of respiratory specimens support this suggestion. However, it is not clear how many identified viruses represent colonisation or asymptomatic carriage. Routine chest radiography and respiratory secretion sampling are not standard practice in diarrhoeal disease and therefore we could not confirm the presence of respiratory disease in these patients.
Conclusion
nCPAP was found to be used clinically for the management of children with respiratory compromise potentially secondary to non-pulmonary illnesses, particularly diarrhoeal disease. In the majority of cases intubation and mechanical ventilation were not required. Larger controlled clinical studies are needed to determine the effectiveness and utility of nCPAP in this population. HFNC was not commonly used, and this modality requires further investigation in this setting.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgements. Thank you to Associate Professor Mignon McCulloch for overseeing this project.
Author contributions. KB: collected data and wrote the paper drafts. BM: principal investigator, analysed data and managed script writing.
Funding. None.
Conflicts of interest. None.
References
1. Argent AC, Bib an P. What's new on NIV in the PICU: Does everyone in respiratory failure require endotracheal intubation? Intensive Care Med 2014;40(6):880-884 https://doi.org/10.1007/s00134-014-3274-z [ Links ]
2. Keenan S, Sinuff T, Burns K, et al. Clinical practice guidelines for the use of noninvasive positive-pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ 2011;183(3):E195-E214 https://doi.org/10.1503/cmaj.100071 [ Links ]
3. Milesi C, Baleine J, Le Bouhellec J, Pons-Odena M, Cambonie G. High flow on the rise pediatric perspectives on the FLORALI trial. J Thorac Dis 2015;7(8):E230-E233. https://doi.org/10.3978/j.issn.2072-1439.2015.07.40 [ Links ]
4. Antonelli M, Conti G, Bello G. New niches for NIV: Ahead with caution! Intensive Care Med 2013;39(7):1325-1327. https://doi.org/10.1007/s00134-013-2943-7 [ Links ]
5. Walkey AJ, Wiener RS. Use of noninvasive ventilation in patients with acute respiratory failure, 2000-2009: A population-based study. Ann Am Thorac Soc 2013;10(1):10-17. https://doi.org/10.1513/AnnalsATS.201206-0340C [ Links ]
6. Frat J-P, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 2015;372(23):2185-2196. https://doi/org/10.1056/NEJMoa1503326 [ Links ]
7. Ramanathan R, Sardesai S. Lung protective ventilatory strategies in very low birth weight infants. J Perinatol 2008;28(Suppl 1):S41-S46. https://doi.org/10.1038/jp.2008.49 [ Links ]
8. Teague WG. Non-invasive positive pressure ventilation: Current status in paediatric patients. Paediatr Respir Rev 2005;6(1):52-60. https://doi.org/10.1016/j.prrv.2004.11.014 [ Links ]
9. Abadesso C, Nunes P, Silvestre C, Matias E, Loureiro H, Almeida H. Non-invasive ventilation in acute respiratory failure in children. Pediatr Rep 2012;4(2):57-63. https://doi.org/10.4081/pr.2012.e16 [ Links ]
10. Gupta P, Kuperstock JE, Hashmi S, et al. Efficacy and predictors of success of noninvasive ventilation for prevention of extubation failure in critically ill children with heart disease. Pediatr Cardiol 2013;34(4):964-977. https://doi.org/10.1007/s00246-012-0590-3 [ Links ]
11. Duke T. CPAP: A guide for clinicians in developing countries. Paediatr Int Child Health 2014;34(1):3-11. https://doi.org/10.1179/2046905513Y.0000000102 [ Links ]
12. Essouri S, Durand P, Chevret L, et al. Physiological effects of noninvasive positive ventilation during acute moderate hypercapnic respiratory insufficiency in children. Intensive Care Med 2008;34(12):2248-2255. https://doi.org/10.1007/s00134-008-1202-9 [ Links ]
13. De Freitas Dantas Gomes EL, Costa D, Germano SM, Borges PV, Sampaio LMM. Effects of CPAP on clinical variables and autonomic modulation in children during an asthma attack. Respir Physiol Neurobiol 2013;188(1):66-70. https://doi.org/10.1016/j.resp.2013.05.004 [ Links ]
14. Fleming PF, Richards S, Waterman K, et al. Use of continuous positive airway pressure during stabilisation and retrieval of infants with suspected bronchiolitis. J Paediatr Child Health 2012;48(12):1071-1075. https://doi.org/10.1111/j.1440-1754.2012.02468.x [ Links ]
15. Furness J, Singh A, Tinnion R. Question 2: Will continuous positive airway pressure reduce the need for ventilation in bronchiolitis? Arch Dis Child 2013;98(12):1020-1022. https://doi.org/10.1136/archdischild-2013-305375 [ Links ]
16. Yanez LJ, Yunge M, Emilfork M, et al. A prospective, randomized, controlled trial of noninvasive ventilation in pediatric acute respiratory failure. Pediatr Crit Care Med 2008;9(5):484-489. https://doi.org/10.1097/PCC.0b013e318184989f [ Links ]
17. Chisti MJ, Salam MA, Smith JH, et al. Bubble continuous positive airway pressure for children with severe pneumonia and hypoxaemia in Bangladesh: An open, randomised controlled trial. Lancet 2015;386(9998):1057-1065. https://doi.org/10.1016/S0140-6736(15)60249-5 [ Links ]
18. Metge P, Grimaldi C, Hassid S, et al. Comparison of a high-flow humidified nasal cannula to nasal continuous positive airway pressure in children with acute bronchiolitis: Experience in a pediatric intensive care unit. Eur J Pediatr 2014; 173(7):953-958. https://doi.org/10.1007/s00431-014-2275-9 [ Links ]
19. Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39(2):165-228. https://doi.org/10.1007/s00134-012-2769-8 [ Links ]
20. Cam BV, Tuan DT, Fonsmark L, et al. Randomized comparison of oxygen mask treatment vs. nasal continuous positive airway pressure in dengue shock syndrome with acute respiratory failure. J Trop Pediatr 2002;48(6):335-339. https://doi.org/10.1093/tropej/48.6.335 [ Links ]
21. Kinikar A, Kulkarni R, Valvi C, Gupte N. Use of indigenous bubble CPAP during swine flu pandemic in Pune, India. Indian J Pediatr 2011;78(10):1216-1220. https://doi.org/10.1007/s12098-011-0389-x [ Links ]
22. Anitha GFS, Velmurugan L, Sangareddi S, Nedunchelian K, Selvaraj V. Effectiveness of flow inflating device in providing continuous positive airway pressure for critically ill children in limited-resource settings: A prospective observational study. Indian J Crit Care Med 2016;20(8):441-447. https://doi.org/10.4103/0972-5229.188171 [ Links ]
23. Spentzas T, Minarik M, Patters AB, Vinson B, Stidham G. Children with respiratory distress treated with high-flow nasal cannula. J Intensive Care Med 2009;24(5):323-328. https://doi.org/10.1177/0885066609340622 [ Links ]
24. Wilson PT, Morris MC, Biagas K V, Otupiri E, Moresky RT. A randomized clinical trial evaluating nasal continuous positive airway pressure for acute respiratory distress in a developing country. J Pediatr 2013;162(5):988-992. https://doi.org/10.1016/j.jpeds.2012.10.022 [ Links ]
25. Kelly GS, Simon HK, Sturm JJ. High-flow nasal cannula use in children with respiratory distress in the emergency department: Predicting the need for subsequent intubation. Pediatr Emerg Care 2013;29(8):888-892. https://doi.org/10.1097/PEC.0b013e31829e7f2f [ Links ]
26. Ten Brink F, Duke T, Evans J. High-flow nasal prong oxygen therapy or nasopharyngeal continuous positive airway pressure for children with moderate-to-severe respiratory distress? Pediatr Crit Care Med 2013;14(7):e326-331. https://doi.org/10.1097/PCC.0b013e31828a894d [ Links ]
27. Schlapbach LJ, Schaefer J, Brady AM, Mayfield S, Schibler A. High-flow nasal cannula (HFNC) support in interhospital transport of critically ill children. Intensive Care Med 2014;40(4):592-599. https://doi.org/10.1007/s00134-014-3226-7 [ Links ]
28. Long E, Babl FE, Duke T. Is there a role for humidified heated high-flow nasal cannula therapy in paediatric emergency departments? Emerg Med J 2016;33(6):386-389. https://doi.org/10.1136/emermed-2015-204914 [ Links ]
29. Centers for Disease Control and Prevention. Diarrhea : Common Illness , Global Killer. 2012. https://www.cdc.gov/healthywater/global/diarrhea-burden.html (accessed 20 May 2019). [ Links ]
30. Stephen C, Bamford L, Patrick M, Wittenberg D. Saving children 2009: Five Years of Data. A Sixth Survey of Child Health Care in South Africa. Pretoria: Tshepesa Press, Medical Research Council of South Africa, Centers for Disease Control and Prevention, 2011. [ Links ]
31. De Lannoy A, Swartz S, Lake L, Smith C (eds). Broad overview of the South African Child Gauge 2015. Cape Town: University of Cape Town, 2015:107. [ Links ]
32. Statistics South Africa. Levels and trends of morbidity and mortality among children aged under-five years in South Africa, 2006-2010. Vol 10. Pretoria: StatsSA, 2010. [ Links ]
33. Hodkinson P, Argent A, Wallis L, et al. Pathways to care for critically Ill or injured children: A cohort study from first presentation to healthcare services through to admission to intensive care or death. PLoS One 2016;11(1):1-16. https://dx.doi.org/10.1371%2Fjournal.pone.0145473 [ Links ]
34. Brown J, Machen H, Kawaza K, et al. A high-value, low-cost bubble continuous positive airway pressure system for low-resource settings: Technical assessment and initial case reports. PLoS One 2013;8(1):e53622. https://doi.org/10.1371/journal.pone.0053622 [ Links ]
35. Mayordomo-Colunga J, Medina A, Rey C, et al. Predictive factors of non-invasive ventilation failure in critically ill children: A prospective epidemiological study. Intensive Care Med 2009;35(3):527-536. https://doi.org/10.1007/s00134-008-1346-7 [ Links ]
36. Wilson PT, Morris MC, Biagas KV, Otupiri E, Moresky RT. A randomized clinical trial evaluating nasal continuous positive airway pressure for acute respiratory distress in a developing country. J Pediatr 2013;162(5):988-992. https://doi.org/10.1016/j.jpeds.2012.10.022 [ Links ]
37. Surenthiran SS, Wilbraham K, May J, Chant T, Emmerson AJ, Newton VE. Noise levels within the ear and post-nasal space in neonates in intensive care. Arch Dis Child Fetal Neonatal Ed 2003;88(4):F315-F318. https://doi.org/10.1136/fn.88.4.f315 [ Links ]
38. Seiger AN, Maconochie I. Validity of different pediatric early warning scores in the emergency department. Pediatrics 2013;132(4):e841-e850. https://doi.org/10.1542/peds.2012-3594 [ Links ]
 Correspondence:
Correspondence:
K Browde
kbrowde@gmail.com
Accepted 17 September 2018.


{kind=link}