










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Child Health
On-line version ISSN 1999-7671
Print version ISSN 1994-3032
S. Afr. j. child health vol.13 n.2 Pretoria Jun. 2019
http://dx.doi.org/10.7196/sajch.2019.v13i2.1571
RESEARCH
Incidence of hypoglycaemia in late preterm and term infants born to women with diabetes mellitus
Y MagadlaI; S VelaphiII; F MoosaIII
IMB ChB, FCPaed, MMed (Paed); Department of Paediatrics, Faculty of Health Sciences, University of Witwatersrand, Johannersburgy, South Africa
IIMB ChB , FCPaed, MMed (Paed), Cert Neonatology; Department of Paediatrics, Faculty of Health Sciences, University of Witwatersrand, Johannersburgy, South Africa
IIIMB BCh, FCPaed, CEM, MMed (Paed); Department of Paediatrics, Faculty of Health Sciences, University of Witwatersrand, Johannersburgy, South Africa
ABSTRACT
BACKGROUND. Diabetes mellitus (DM) is a common metabolic disorder affecting pregnant women and is associated with adverse outcomes in their offspring, including hypoglycaemia. The incidence and factors associated with development of hypoglycaemia in infants of diabetic mothers (IDM) from developing countries such as South Africa are not well known. Objectives. To determine the incidence of hypoglycaemia and factors associated with its development in IDM.
Methods. Medical records of mothers diagnosed with DM, and their infants who were term and/or late preterm and admitted to the neonatal unit at Chris Hani Baragwanath Academic Hospital, were retrieved and reviewed. Maternal characteristics, type and management of diabetes, infant characteristics and glucose measurements were captured for analysis.
RESULTS. Over the 2-year period, 234 infants were born to diabetic mothers (median age 33 years) and 207 met the diagnostic criteria and were admitted for monitoring of blood glucose using the hemoglucotest. Among the mothers with DM, 56% had gestational diabetes; ~19% of IDM were large for gestational age (LGA) and 10% were macrosomic. Hypoglycaemia occurred in 39% of IDM, and 85% of the infants were diagnosed within the first 6 hours of life. There were no statistically significant differences in maternal characteristics, including type of maternal diabetes and its management between hypoglycaemic and normoglycaemic infants. Hypoglycaemic infants were more likely to be LGA (28.2% v. 12.8%; p=0.009).
CONCLUSION: Hypoglycaemia is a common finding in IDM. It presents early (within the first 6 hours of life) and rarely beyond 24 hours after birth. The only characteristic found to be associated with development of hypoglycaemia in IDM was a neonate being LGA.
Diabetes mellitus (DM) is a multisystem disease causing both biochemical and structural alterations in the afflicted person. The incidence of DM is increasing rapidly and is estimated to double by 2030.[1] It is the most common metabolic disease affecting pregnancy and may result in adverse fetal and neonatal outcomes[2] Over the past years the outcomes of diabetic pregnancies have improved to almost what is expected in non-diabetic pregnancies thanks to advanced management provided by obstetricians.® Improved outcomes apply in high-income countries due to better resources such as preconception clinics and continuous glucose monitoring[4] Diabetes complicates about 3 - 10% of pregnancies, with gestational DM (GDM) causing 80% of these diabetic pregnancies, as opposed to pre-gestational DM.[3] A United States study on the trend in the prevalence of gestational and pre-gestational diabetes from 1999 to 2005 showed that a prevalence of 10% was due to pre-gestational in 1999 and increasing to 21% in 2005, with the gestational DM accounting for the remaining women (90% in 1999 and 79% in 2005) with diabetes in pregnancy.[5]
The increase in DM incidence is attributed to lifestyle changes and urbanisation growing in parallel with overweight and obesity as well as older age in pregnant populations and late presentation[2] There is a clear need for further research into diabetes in pregnancy as there is inadequate information about the disease in Africa. [6,7]
After delivery, the infants of diabetic mothers (IDM) are at risk of having respiratory distress syndrome and multiple metabolic complications, including hypoglycaemia. Complications have been related to time of diagnosis of DM and the type and control of DM.[3,8-10] Therefore, knowledge of the type of maternal diabetes and diabetic management or control during pregnancy and their role in neonates developing hypoglycaemia, allows pediatricians to anticipate those infants who are likely to develop complications post delivery. Hypoglycaemia is reported to develop in 20 - 50% of IDM and 15 - 25% of hypoglycaemic IDM are born to mothers with gestational diabetes[11,12] Data on the incidence of hypoglycaemia are lacking in South Africa (SA) due to a lack of consensus on the definition of hypoglycaemia and different screening methods utilised by different institutions. Current literature recommends continuous glucose monitoring, which is only possible in high-income countries. Hypoglycaemia is typically noted in neonates who are large for gestational age (LGA) or small for gestational age (SGA) and those infants whose mothers had poor glycaemic control during pregnancy.[3] Hyperinsulinism is the cause of neonatal hypoglycaemia, which Pederson's hypothesis explains as being a consequence of maternal hyperglycaemia, leading to fetal hyperglycaemia that in turn stimulates the fetal pancreas, causing excessive insulin secretion and leading to hypoglycaemia in the newborn. This condition is exacerbated by the interruption of placental glucose transfer that occurs after delivery.[14]
The nadir in IDM blood glucose levels usually occurs between 1 - 3 hours of life, can persist up to 72 hours and may even last up to a week.[2] Hypoglycaemic IDM are commonly asymptomatic and if they become symptomatic, early features include tachypnoea, apnoea, tremors, sweating, irritability and seizures, thus emphasising the need for monitoring glucose levels post delivery[13,15] Late features include delayed developmental milestones, poor Bayley scores and poor school performance in lower grades and that correlates with duration, severity and number of hypoglycaemic episodes.[16] No single study is conclusive as to which infants should be routinely tested, and at what point in the postpartum period this should be done. One study recommended that infants must be screened at 4 - 6 hours of life, with an emphasis that no studies demonstrated harm from fewer hours of hypoglycaemia,[17] and another study demonstrated that IDM have asymptomatic hypoglycaemia in the first hour, thus supporting earlier screening in these infants and to stop after 12 hours, if glucose levels remain above 2.6 mmol/L.[18]
At Chris Hani Baragwanath Academic Hospital (CHBAH), which is a tertiary hospital admitting mostly patients from the urban township of Soweto, all IDM are admitted for monitoring of glucose for 12 to 24 hours. Knowing the characteristics of IDM at risk of developing hypoglycaemia, may assist in focusing glucose monitoring and appropriate management in this specific group of patients, allowing early discharge of others. Therefore, we sought to determine the incidence of hypogylcaemia and characteristics of term and late-term infants admitted for glucose monitoring born to diabetic pregnant mothers.
Methods
This was a retrospective study conducted at CHBAH. This hospital delivers two-thirds of annual births from the surrounding urban, low-to middle-income population of Soweto. About two-thirds of women delivering iat this hospital are referrals from local clinics and hospitals with obstetric risk factors including diagnosis of diabetes mellitus, and a third are self-referrals with normal pregnancies. The majority of Soweto births outside CHBAH occur in public clinics, and if any of these newborns require further medical management, they are referred to CHBAH. During the study period, CHBAH was the only public hospital admitting high-risk or sick neonates in Soweto.
Inclusion criteria
Term and late pre-term infants (defined as birth weight of at least 2 000 g or more and gestational age of 34 weeks or more),[19] who were born and admitted to the CHBAH neonatal unit from January 2012 to December 2013, with a main diagnosis of IDM.
Exclusion criteria
Infants weighing less than 2 000 g, gestational age less than 34 weeks, and admission from another hospital with no hospital records.
Procedures
Hospital medical records of infants with a diagnosis of IDM were reviewed and their mothers' records were retrieved. Data on infant and maternal demographics, type and management of maternal DM, infant anthropometry, glucose levels and diagnosis of hypoglycaemia were collected. Maternal diabetes was classified as 'pre-gestational' if the patient was a known diabetic at first antenatal visit and 'gestational' if diabetes was diagnosed at or after first antenatal visit, using the WHO criteria. During the study period, CHBAH was using the 100 g OGTT (oral glucose tolerance test) which they have since changed to 75 g OGTT.
Macrosomia was defined as newborns weighing above 4 000 g at birth. Large for gestational age was defined as weight above 90th centile for gestational age, SGA as weight below the 10th centile for gestational age and appropriate for gestational age (AGA) as weight between the 10th and 90th centiles for gestational age
Ethics
Permission to conduct this study was obtained from the CHBAH protocol committee and the Wits University Human Research Ethics Committee (ref. no. M131139).
Results
Over a period of 24 months, from January 2012 to December 2013, there was a total of 43 876 live births at CHBAH, of which 234 were from mothers with DM, giving a prevalence of diabetes during pregnancy of 5.3 per 1 000 live births. From this total of 234 IDM, only 207 met the inclusion criteria. Among the 207 neonates, 80 (39%) were born to mothers with pre-gestational diabetes (29 having type I DM, 43 having type II DM, 8 were of an unspecified pre-gestational type), 101 (49%) to mothers with gestational diabetes and in 26 (12%) cases, the type of DM was not stated. Overall, among the 181 records of known diabetes status, 56% had gestational DM.
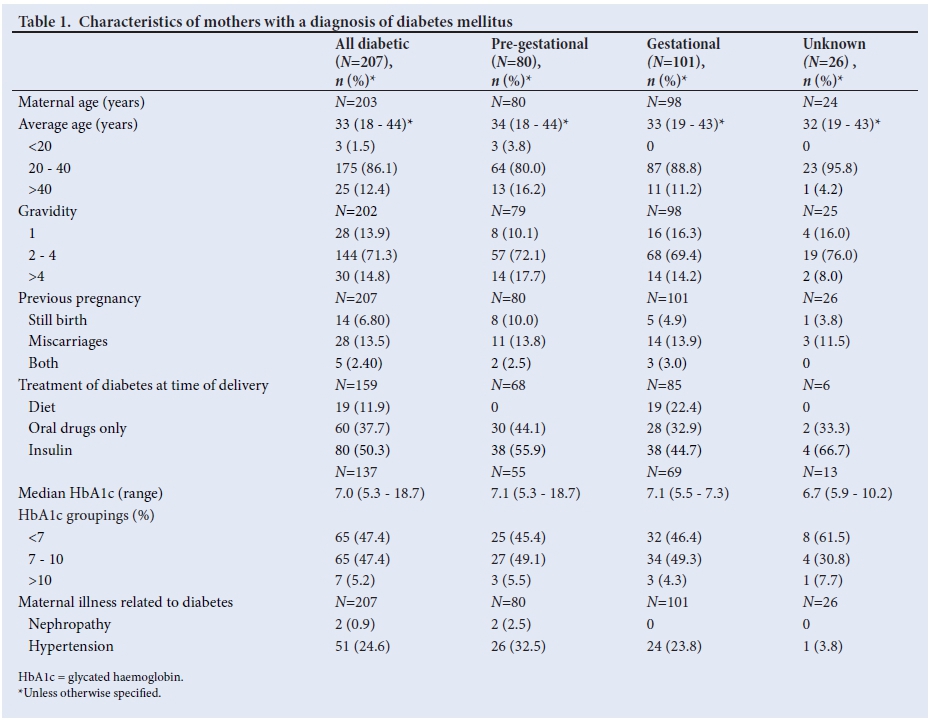
Characteristics of mothers diagnosed with diabetes mellitus
The majority of mothers (94.1%) were of African origin and fell within the age range of 20 - 40 years (86.1%) (Table 1). Only 3 mothers were younger than 20 years and all had pre-gestational diabetes. The median (range) maternal weight at initial antenatal care visit was 85 kg (range 48 - 149) and 20% weighed more than 100 kg. Height was not recorded. About 47 mothers had adverse outcomes in their previous pregnancy (14 stillbirths, 28 miscarriages and 5 had both stillbirths and miscarriages). There were no differences relating to these adverse outcomes, between those with gestational and pre-gestational diabetes (26.2% v. 21.8%; p=0.540).
Among the 159 patients whose management of diabetes during pregnancy was recorded at time of delivery, 12% were managed with diet only, 38% with oral medication and 50% with insulin. About 60% of pre-gestational mothers were treated with insulin compared with 45% of those with gestational diabetes (p=0.582). Among the mothers with known HbA1c levels, 53% had HbA1c >7.0%, with no differences in the level of HbA1c (median 7.1% v. 7.1%; p=0.920) or proportion of mothers with HbA1c >7% (54.6% v. 53.6%; p=0.959) between pre-gestational and gestational groups. The common associated maternal complication recorded was hypertension (24.6%).
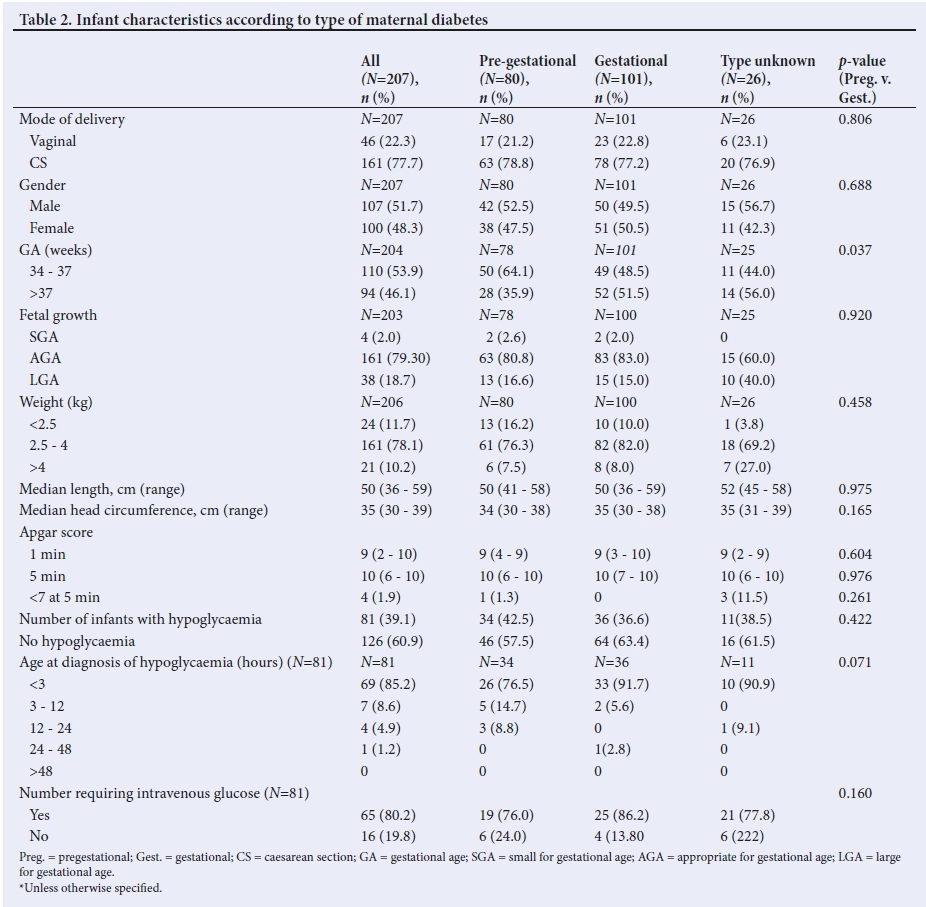
Infant characteristics
Demographics, anthropometry and Apgar scores of infants are reported in Table 2. Most (77.7%) of IDM were delivered by caesarean section. Just over 50% were born preterm (gestational age 34 - 36 weeks), and there were more babies born preterm in the pre-gestational group compared with those with gestational DM (p=0.037). About 18% of infants were large for gestational age (LGA), 10% were macrosomic and there were no differences between the types of maternal diabetes in prevalence of LGA and macrosomia. The length, head circumference measurements and Apgar scores were also not significantly different between the 2 groups.
Incidence of hypoglycaemia in infants of diabetic mothers
Among the 207 IDM, 81 (39%) had hypoglycaemia (defined as random blood glucose <2.6 mmol/L), with 42.5% occurring in the pre-gestational group, compared with 36.6% in those with gestational DM (p=0.422) (Table 2). In most (85%) of the infants, the hypoglycaemia occurred within the first 3 hours of life, with no difference as to the time of presentation of hypoglycaemia between pre-gestational and gestational DM groups. For the hypoglycemic group, the median was 2.7 (2.3 - 3.0). Only 1 baby had hypoglycaemia after 24 hours. A total of 65 (80%) hypoglycaemic infants («=81) required glucose supplementation using intravenous fluids that contained 10% glucose.
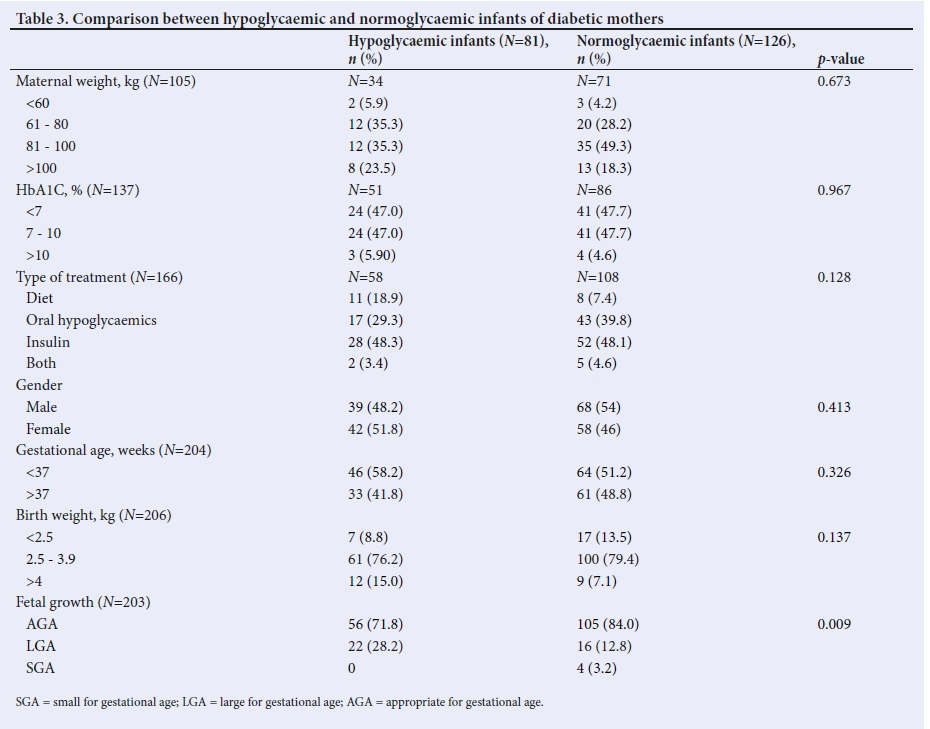
Comparison of hypogycaemic v. normoglycaemic infants
No statistically significant differences were found in maternal weight, HbA1c, diabetes type, type of pre-gestational DM, treatment modalities, sex of the infant, gestational age and birth weight when comparing hypoglycaemic and non-hypoglycaemic infants. However, the proportion of LGA infants was significantly higher in the hypoglycaemic than the normoglycaemic group (28.2% v. 12.8%; p=0.009)
Discussion
DM is the most common metabolic disease affecting pregnancy, with previous studies documenting a preponderance of gestational diabetes.[15,20,21] One of the common perinatal complications associated with DM during pregnancy is hypoglycaemia in infants. Hypoglycaemia can be associated with severe morbidity and mortality, nd therefore infants known to be at risk of developing hypoglycaemia need regular glucose monitoring. This often results in delays in discharging the IDM home and placing additional strain on limited resources, thus making it crucial to know the prevalence and characteristics of those infants who develop hypoglycaemia.
The first finding in the present study was a prevalence of IDM at 5.3% that is lower than a recent study by Macauley et al.[22] This could relate to different screening methods and variation in diagnostic criteria.[3] For our study, diagnostic criteria were not specified in the files but the clinical norm in 2012 was risk factor-based screening and a 100 g OGTT which has been changed to 75 g OGTT. Another finding was that more than half of mothers diagnosed with DM at the time of birth, had gestational DM. Though >50% of mothers were managed with insulin, a significant number (37%) were managed with oral hypoglycaemic agents during pregnancy. None of the women with pre-gestational diabetes was managed with diet only, whereas ~20% of women with gestational diabetes were managed in this way. Only about a fifth of the IDM were large for gestational age and a tenth were macrosomic. About 40% of IDM developed hypoglycaemia, with most of them developing hypoglycaemia within the first 6 hours of life.
A number of studies have reported similar findings that mothers with DM during pregnancy are more likely to have gestational DM than pre-gestational DM. The high proportion of women with gestational DM compared with pre-gestational DM could be because of a high proportion of undiagnosed, asymptomatic women with DM before pregnancy and presenting late during pregnancy therefore labelled as gestational DM, and that there is better screening for DM together with increased contact with healthcare during pregnancy. [8,12,23] Slightly more than 50% of all women in this report, and 56% of those with pre-gestational diabetes, were managed with insulin, which was more than the 47.2% of women in the same category reported elsewhere.[8]
Macrosomic and LGA babies are common among IDM compared with infants of mothers without diabetes.[23,24] The prevalence of macrosomia has been reported to be 15%,[8] while that of LGA babies as been reported to be 35%.[25] The prevalence of macrosomia (10%) and LGA (18%) in our study was much lower than previously reported rates, possibly due to incorrect gestational age assessment in our cohort. The higher prevalence of 15% in a previous study[8] was attributed to the definition of macrosomia used, i.e. weight greater than 90th centile for gestational age, while we used weight greater than 4 000 g. Nonetheless, a significant association was noted between LGA and hypoglycaemia.
The proportion of IDM who developed hypoglycaemia in the present study was 39% compared with 56%[23] reported in recent studies, while another reported (33.4%) [8] - thse figures may be related to differences and higher numbers of macrosomic patients (15%) in the same study that had hypoglycaemia (56%). Another cause could be different definitions of hypoglycaemia used. There are a number of factors that have been associated with hypoglycaemia in IDM. These include babies that are LGA, SGA, increased maternal HbAlc levels and poor maternal glucose control[8-10-16] LGA was the only infant characteristic identified to be significantly associated with hypoglycaemia in this study. The present study also found no correlation between the HbAlc levels and incidence of hypoglycaemia, similar to a previous report.[26] However, another study[11] reported a statistically significant association between hypoglycaemia and HbA1c.
The majority of patients who had hypoglycaemia developed it within the first 6 hours post- delivery. This drop in glucose post delivery is explained by the transition from the intrauterine, maternally supported life to extra uterine life. Infants of diabetic mothers are reported to be more at risk due to their hyperinsulinaemic state caused by high glucose levels from the mother in-utero, leading to pancreatic stimulation and insulin secretion. Therefore, removal of glucose supply from the mother during delivery in the presence of hyperinsulinism increases the risk of hypoglycaemia in the neonate after delivery. Nold et al.[6] reported similar findings that IDM develop hypoglycaemia within the first six hours of life.
Study limitations
The limitations of this study include the fact that it was of the retrospective nature, therefore leading to difficulties in finding complete data sets, namely maternal weight, type of maternal diabetes mothers which has led to inability to distinguish between T1DM and T2DM. Thus, incomplete data could have affected the findings of an association between maternal diabetes and the prevalence of hypoglycaemia in IDM. In most of the mothers, the gestational age of the baby was assessed on maternal dates and most of the babies did not have Ballard scoring done. This is likely to result in inaccurate assessment of gestational age as the use of last menstrual period is known to overestimate gestational age likely because of delayed ovulation, leading to a lower estimated occurrence of LGA.[27] Inaccurate assessment of gestational age could have led to under or overestimation of the effect of DM on fetal growth and in assessing the association of prevalence of hypoglycaemia and fetal growth. The lack of information to calculate BMI (basal metabolic index) led to an inability to correlate maternal BMI and neonatal hypoglycaemia.
Conclusion
A significant number of IDM developed hypoglycaemia soon after delivery with most patients developing hypoglycaemia within the first six hours of life, rarely beyond 24 hours. Large for gestational age was the only infant characteristic found to be significantly associated with hypoglycaemia. These findings are in agreement with a report by Blank et al[8] which suggested that 12 hours of glucose monitoring is adequate in IDM and late preterms, and recommendations by American Academy of Pediatrics [29] that screening time of 12 hours might be adequate for IDM and those more than 64 weeks. Currently management of IDM at CHBAH is that all IDM are admitted for 12 - 24 hours for glucose monitoring, and a diagnosis of hypoglycaemia is made if glucose levels on hemoglucotest are less than 2.8 mmol/L, this is based on Pediatric Endocrine Society consensus which recommends a target glucose of more than 2.8mmol/L for high risk neonates in the first 48 hours of life.[60-
Therefore, we recommend that well IDM at a gestation of 64 weeks or greater have glucose testing at the bedside using a point-of-care testing system (hemoglucotest) within an hour after delivery, then hourly for the first 6 - 4 hours of life (in a high-care or triage area), while continuing with breastfeeding. If the hemoglucotest levels are >2.8 mmol/L with all measurements, then the infant can be transferred to his/her mother where he/she can be monitored with 6-hourly hemoglucotest for another 12 - 24 hours, before discharge. This will reduce the number of IDM who get admitted to neonatal wards, and thus leaving more space to admit critically ill neonates. More studies are required to further elucidate if there are differences in incidence of hypoglycaemia and time of onset based on type of pregestational DM.
Declaration. This manuscript was submitted in partial fulfilment of the requirements for the degree of Master of Medicine.
Acknowledgements. I would like to express my gratitude to my family and to Prof. Velaphi and Dr Moosa, my research supervisors for their guidance.
Author contributions. YM: developed the theory, wrote the protocol for ethics approval, data collection and interpretation, wrote the manuscript with assistance from SV and FM. SV: provided the title and study design, guidance with data collection and interpretation, drafting of the manuscript and approved the final version of the manuscript. FM: guidance with data analysis, interpretation and approved the final version of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2 000 and projections for 2030. Diabetes Care 2004;27(5):1047-1053. https://doi.org/10.2337/diacare.27.5.1047 [ Links ]
2. International Diabetes Federation. IDF Diabetes Atlas, 6th ed. Brussels, Belgium: International Diabetes Federation; 2013. http://www.idf.org/diabetesatlas (accessed 16 September 2016). [ Links ]
3. Nold JL, Georgieff MK. Infants of diabetic mothers. Pediatr Clin North Am 2004;51(3):619-637. https://doi.org/10.1016/j.pcl.2004.01.003 [ Links ]
4. Murphy HR, Bell R, Cartwright C, Curnow C et al. Improved pregnancy outcomes in women with type 1 and type 2diabetes but substantial clinic to clinic variations: A prospective nationwide study. Diabetologica 2017;60:1668-1677. https://doi.org/10.1007/s00125-01704314-3. [ Links ]
5. Lawrence JM, Contreras R, Chen W, Sacks DA. Trends in the prevalence of preexisting diabetes and gestational diabetes mellitus among a racially/ ethnically diverse population of pregnant women, 1999 - 2005. Diabetes Care 2008;31:899-904. https://doi.org/10.2337/dc07-2345 [ Links ]
6. Macauley S, Dunger DB, Norris SA. Gestational diabetes mellitus in Africa: Asystematic review. PLoS ONE 2014;9(6):e97871. [ Links ]
7. https://doi.org/10.1371/journal.pone.0097871
8. Kanguru L, Bezawada N, Hussein J, Bell J. The burden of diabetes mellitus during pregnancy in low- and middle-income countries: A systematic review. Glob Health Action 2014. 1;7:23987. https://doi.org/10.3402/gha.v7.23987 [ Links ]
9. Van Haltren K, Malhotra A. Characteristics of infants admitted with hypoglycaemia to a neonatal unit. J Pediatr Endocrinol Metab 2013;26:525-529. https://doi.org/10.1515/jpem-2013-0009 [ Links ]
10. Hay WW, Jr. Care of the infant of the diabetic mother. Curr Diab Rep 2012;12:4- 15. https://doi.org/10.1007/s11892-011-0243-6 [ Links ]
11. Coetzee EJ, Levitt NS. Maternal diabetes and neonatal outcome. Semin Neonatol 2000;5(2):221-229. [ Links ]
12. Fanaroff AA, Stoll BJ, Wright LL, et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol 2007;196:147e1-8. [ Links ]
13. Stoll B. The endocrine system. In: Kliegman RM Behrman REJenson HB,Stanton FB.Nelson textbook of pediatrics 18th ed..Philadelphia: Elsevier; 2011:627-629. [ Links ]
14. Cowett RM. The Infant of the diabetic mother. Neonat Rev 2002;3:173e-189e. [ Links ]
15. Pedersen J. The pregnant diabetic and her newborn: Problems and management. 2nd ed. Baltimore: William and Wilkins; 1977. [ Links ]
16. Cornblath M, Hawdon JM, Williams AF, Aynsley-Green A, Ward-Platt MP, Schwartz R, et al. Controversies regarding definition of neonatal hypoglycaemia: Suggested operational thresholds. Pediatrics 2000;105(5):1141-1145. https://doi.org/10.1542/peds.105.5.1141 [ Links ]
17. Sharma A, Davis A, Shekhawat PS. Hypoglycaemia in the preterm neonate: etiopathogenesis, diagnosis, management and long-term outcomes. Transl Pediatr 2017;6(4):335-348.https://doi.org/10.21037/tp.2017.10.06 [ Links ]
18. Williams AF. Hypoglycaemia of the newborn: A review. Bull World Health Organ 1997;75(3):261-290. [ Links ]
19. Holtrop PC .The frequency of hypoglycaemia in full-term large and small for gestational age newborns. Am J Perinatal 1993;10(2):150-154. https://doi.org/10.1055/s-2007-994649 [ Links ]
20. Engle WA. A recommendation for the definition of late pre-term (near-term) and the birth weight-gestational age classification system. Semin Perinatol 2006;30(1):2-7. https://doi.org/10.1053/j.semperi.2006.01.007 [ Links ]
21. Maso G, Piccoli M, Parolin S, Restaino S, Alberico S. Diabetes in pregnancy: Timing and mode of delivery. Curr Diab Rep 2014; 14(7):506:1 -11 https://doi.10.1007/s11892-01400506-0 [ Links ]
22. Catalano PM, Tyzbir ED, Allen SR, McBean JH, McAuliffe TL. Evaluation of fetal growth by estimation of neonatal body composition. Obstet Gynecol 1992;79:46-50. [ Links ]
23. Macaulay S, Ngobeni M, Dunger DB, Norris SA. The prevalence of gestational diabetes mellitus amongst black South African women is a public health concern. Diabetes Res Clin Pract 2018;139:278-287. https://doi.org/10.10167j.diabres.2018.03.012 [ Links ]
24. Das S, Irigoyen M, Patterson MB, Salvador A, Schutzman DL. Neonatal outcomes of macrosomic births in diabetic and non-diabetic women. Arch Dis Child Fetal Neonatal Ed 2009;94:F419-F422. https://doi.org/10.1136/adc.2008156026. [ Links ]
25. Armangil D, Yurdakok M, Korkmaz A, Yigit S, Tekinalp G. Ponderal index of large-for-gestational age infants: Comparison between infants of diabetic and non-diabetic mothers. Turk J Pediatr 2011;53:169-172. [ Links ]
26. El-Masry SA, El-Ganzoury MM, El-Farrash RA, Anwar M, Abd Ellatife RZ. Size at birth and insulin-like growth factor-I and its binding protein-1 among infants of diabetic mothers. J Matern Fetal Neonatal Med 2013;26:5-9. https://doi.org/10.3109/14767058.2012.718000. [ Links ]
27. Stenninger E, Schollin J, Aman J. Early posnatal hypoglycaemia in newborn infants of diabetic mothers. Acta Paediatric 1997;86:137420. https://doi.org/10.1111/j.1651-2227.1997.tb14916.x [ Links ]
28. Savits DA, Terry JW Jr, Dole N, Thorp JM Jr, Siega-Riz AM, Herring AH. Comparison of pregnancy dating by last menstrual period, ultrasound scanning, and their combination. Am J Obs Gynecol 2002;187(6):1660-1666. https://doi.org/10.1067/mob.2002.127601 [ Links ]
29. Blank C, van Dillen J, Hogeveen M. Primum non nocere: Earlier cessation of glucose monitoring is possible. Eur J of Pediatr 2018;177(8):1239-1245. https://doi.org/10.1007/s00431-018-3169-z [ Links ]
30. Adamkin DH. Committe on fetus and newborn. Clinical report on postnatal glucose homeostasis in late term and preterm. Paediatrics 2011;127:175 [ Links ]
31. Thornton ST, Stanley CA, De Leon DD, et al. Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycaemia in Neonates, Infants and Children. J Pediatr 2015;167(2):238-245. https://doi.org/10.1016/jpeds.2015.03.057 [ Links ]
 Correspondence:
Correspondence:
Y Magadla
dryoza@yahoo.com
Accepted 17 September 2018


{kind=link}
{kind=link}
{kind=link}